Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
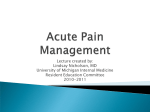
SYMPTOM RESPONSE KIT – Prescription/Order form First Kit Replacement Kit (pick up old kit) Name: Address: DOB: OHIN: Allergies: Phone: Date Ordered: NOTE: Consider any potential risks to storing injectable opioids in the home Symptom Pain/Dyspnea MD initials Oropharyngeal secretions Agitation/Nausea Persistent seizures Medications Morphine Hydromorphone Hydromorphone Atropine Sulfate Haloperidol Diazepam* Midazolam* Midazolam* Furosemide* Dexamethasone Concentration 15 mg/ml (parenteral) 2 mg/ml (parenteral) 10 mg/ml (parenteral) 1% drops 1 drop ~ 0.5 mg 5 mg/ml (parenteral) 5 mg/ml (parenteral) 5 mg/ml (parenteral) 5 mg/ml (parenteral) 10 mg/ml (parenteral) 4 mg/ml (parenteral) Specific Order mg sc q4h + mg sc q1h prn mg sc q4h + mg sc q1h prn mg sc q4h + mg sc q1h prn 1 drop sublingual q4h prn If not effective → 2 drops sl q4h prn 1 mg sc q12h + 0.5 mg sc q1h prn mg per rectum once mg sc once 1 mg sc q2h + 0.5 mg sc q1h prn 20 mg IM once mg sc at (times): Dispense 1 ml amp 1 ml amp 1 ml amp 5 ml bottle 2 x 1 ml amps 3 x 2 ml amps 6 x 1 ml amps 10 x 1 ml amps 3 x 2 ml amps 3 x 5 ml vials Agitation (for sedation) Pulmonary edema Symptom Management Other: Other: *Medications covered only if ordered by MD listed on Palliative Care Facilitated Access list or if expedited request made by calling 1-866-811-9893. Insert Foley Catheter to straight drainage PRN Irrigate Foley PRN and change Foley monthly PRN CONTACT A PHYSICIAN PRIOR TO ADMINISTERING ANY OF THE ABOVE MEDICATIONS YES NO Physician’s name: Physician’s signature: Address: CPSO# Office phone number: Pager number: Fax number: Secondary phone number: Alternate physician information Name: Phone number: Pager number: Nurses name: LOCATION OF SYMPTOM RESPONSE KIT IN HOME: For information or advice any time of day contact: Ontario Medical Supply (OMS) (Mon – Sun 0800 – 2000) : 1-800-461-3599 x 5900 After hours pager number: 1-888-290-8226 Queen’s Palliative Care Medicine (Mon – Fri 0800 – 1700): 613-548-2485 After hours: 613-548-3232 (KGH Switchboard) Palliative Pain & Symptom Management Consultation Service: (Mon – Fri 0830 – 1630): 1-888-547-7744 SE CCAC #15 (Dev. Feb 2012) Instructions for physicians: 1) Place your initials in the column of the table for any medications you want included in the kit. 2) Complete the order and prescription in the row for each selected medication. 3) Fax this completed form to the CCAC Case Manager responsible for the patient’s care: CCAC Location Kingston Bancroft Belleville Selby Northbrook Smiths Falls Brockville Fax number 613-544-1494 613-332-4873 613-966-0996 613-388-2646 613-336-9104 613-283-0308 613-283-0308 4) Reorder a symptom response kit using a fresh Prescription/Order Form: When the expiry date on the outside of the kit passes When medications need to be added or changed When the kit is used for a crisis, the nurse and physician decide whether or not items need to be replaced. Replacements can be obtained at any pharmacy. Opioid Conversion Doses (from Cancer Care Ontario) Drug Approximate Equivalent Dose (mg) Parenteral Oral Codeine 120 200 Fentanyl 0.1-0.2 n/a Morphine 10 20-30 Hydromorphone 2 4-6 Oxycodone n/a 30 Persistent generalized seizures lasting over 5 minutes: Diazepam 0.2 mg/kg rectally (maximum 20mg) or Midazolam 0.2mg/kg subcutaneously (maximum 15mg) Resource: Cancer Care Ontario Guides to Practice: https://www.cancercare.on.ca/toolbox/symptools/ 2 - 12F Foley Catheters 2 - 14F Foley Catheters Foley catheter insertion kit 1 Foley night bag 12 – 1cc syringes Supplies for All Kits 12 - 3cc syringes 12 – 25g 5/8”needles 12 – 25g 1” needles 4 – 21g 1.5” needles 4 – injection caps 2 – 23g and 2 – 25g Butterflies 24 - syringe cannulas 50 – alcohol swabs/ 1 roll paper tape 4 - transparent dressings 1 - sharps container