Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
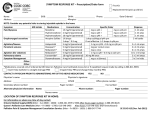
BRN#:___________ Appendix 2 – HPC Teams for Central LHIN Symptom Relief Kit PALLIATIVE SYMPTOM RELIEF KIT (SRK) PRESCRIPTION Hospice Palliative Care Teams for Central LHIN POLICY 1. This is a physician’s order to be implemented by a Registered Nurse when symptoms require urgent intervention to facilitate a comfortable home death. 2. The attending physician is to be notified as soon as possible regarding change in patient’s condition and need for ongoing prescription(s). 3. EDITH (Expected Death in the Home) protocol should be in place. 4. Completed prescription to be FAXED to CCAC 416-222-6517 (South) / 905-952-2404 (North) AND the pharmacy; Calea 905- 629-0123 or Bayshore 1-888-287-8577 (Applicable pharmacy determined by CCAC) URGENT DELIVERY RN TO VISIT ASAP TO INITIATE KIT Date: Patient Name: (Last Name, First Name) dd/mm/yy DOB: HIN: dd/mm/yy Address for Delivery: ANXIETY or SEIZURE: Lorazepam tab 1mg Dispense: 10 tabs PO (not SL formulation) 1-2 tabs PO/SL q2h PRN. May crush or dissolve in water to put under tongue. DELIRIUM OR NAUSEA: Haloperidol Inj 5mg/ml Dispense: 3 amps of 5mg 2mg SC q1h until settled, then 2mg q3-4h PRN (2 mg = 0.4 ml) Midazolam 5 mg/ml injectable 1 ml amp Dispense: 5 amps 1 mg-2 mg SC q1h PRN (1 mg = 0.2 ml) Palliative Care Facilitated Access license required for coverage under ODB (Nurse must contact physician before initiating) Olanzapine Sublingual (Zyprexa Zydis) 5mg Rapid Dissolve Tab Dispense: 5 tabs 5mg PO once daily, placed on tongue EXCESS PULMONARY SECRETIONS: Atropine 1% Eye Drops Dispense: 5ml 2 drops SL or buccal q3h PRN Methotrimeprazine (Nozinan) 25 mg/ml Dispense: 5 amps 12.5 mg- 25 mg SC q3h PRN (12.5 mg = 0.5 ml) (Nurse must contact physician before initiating) Scopolamine 0.4 mg/ml injectable 1 ml Dispense: 5 amps 0.4 mg SC q3h PRN Palliative Care Facilitated Access license required for coverage under ODB PAIN and/or SHORTNESS OF BREATH: CHOOSE ONLY ONE OPIOID Hydromorphone (Dilaudid) Inj 10mg/ml Morphine Inj 15mg/ml Dispense: 4 amps Dispense: 10 amps Opioid naïve patients with moderate to severe pain or dyspnea require 1mg SC q1h PRN. (Contact the physician for increased dosing if symptoms are unmanaged) Opioid naïve patients with moderate to severe pain or dyspnea require 3mg SC q1h PRN. (Contact the physician for increased dosing if symptoms are unmanaged) (1 mg = 0.1ml) use 1cc syringe with needle (3mg = 0.2ml) use 1cc syringe with needle For Physician information: If patient is already on oral Hydromorphone / Morphine, to convert from patient’s usual dose, take total daily dose and calculate half to give total parenteral daily dose. Parenteral daily dose should be divided up over 24 hours to calculate an hourly dosage. ADDITIONAL MEDICATIONS Note: Nurse to use a separate butterfly for each medication and label. Nurse to begin with lowest dose first. INSERT INDWELLING FOLEY CATHETER PRN CCAC TO USE ESTABLISHED PROCESSES TO ORDER THE FOLLOWING SUPPLIES: FOLEY CATHETER KIT: Yes No PRN adaptor (4), Gloves (2 pairs),Transpore tape Size: 14 and 16 SUPPLIES: Alcohol swabs (20), TB syringes (10), Butterfly (4),Tegaderm (4), Physician Contact Information: Office Pager Physician Signature Cell Print Physician Name Palliative Symptom Relief Kit Prescription – CCAC 159 April 2014 Fax OPSC#