Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
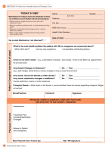
IMMACULATA HIGH SCHOOL 240 Mountain Ave. Somerville, NJ 08876 (908) 722-0200, Fax (908) 218-7765 Health Office Dear Parents, Guardians, and Students, It is the policy of Immaculata High School that no medication is to be kept in the student’s possession or locker. This includes simple over the counter drugs such as aspirin, Tylenol, vitamins, etc. All students who require medication for whatever reason must do the following: 1. Present a written consent signed by the parent or legal guardian requesting the administration of the prescribed medication at school. Verbal consent is not acceptable. It must be written out and signed. 2. Written orders are to be provided to the school from the private physician, detailing the diagnosis of type of illness involved in the name of the drug, dosage and time of administration. 3. The medication should be brought to the school in the original container, appropriately labeled by the pharmacy or physician, with the student’s name. Absolutely no medication will be given to a student without any of the proper consents and written orders by a physician. There are no exceptions. TO BE COMPLETED BY PHYSICIAN Name of Student _____________________________________________________________________ Diagnosis ___________________________________________________________________________ Name of Medication __________________________________________________________________ Time to be given _____________________________________________________________________ Dosage to be given ____________________________________________________________________ Length of treatment ___________________________________________________________________ Standing order for ____Tylenol 500 mg po PRN q 4 hours or Ibuprofen 400 mg po PRN q 4 hours_____ Name of Physician (Please Print) ________________________________________________________ Signature of Physician Date ____________________________________________________________ Parent Permission _____________________________________________________________________