Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Onchocerciasis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Marburg virus disease wikipedia , lookup
Leptospirosis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Hepatitis B wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Neonatal infection wikipedia , lookup
Sarcocystis wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Schistosomiasis wikipedia , lookup
Multiple sclerosis wikipedia , lookup
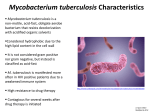
CHAPTER 27 Mycobacteria Mycobacterium is a genus of Gram-positive bacilli that demonstrate the staining characteristic of acid-fastness. Its most important species, Mycobacterium tuberculosis, is the etiologic agent of tuberculosis, the dread disease once called consumption. One of the oldest and most devastating of human afflictions, tuberculosis remains a leading cause of infectious deaths worldwide today. A second mycobacterium, Mycobacterium leprae, is the causative agent of leprosy. A large number of less pathogenic species are assuming increasing importance as disease agents in immunocompromised patients, particularly those with acquired immunodeficiency syndrome (AIDS). MYCOBACTERIUM: GENERAL CHARACTERISTICS I. BACTERIOLOGY A. MORPHOLOGY AND STRUCTURE 1. Slim, poorly staining bacilli which demonstrate the property of acid-fastness 2. Cell wall has high lipid content 3. Mycolic acids and lipoarabinomannan (LAM) form waxy coat 4. Acid fastness: Once stained, difficult to decolorize B. GROWTH 1. Strict aerobes, many species grow slowly 2. M. leprae does not grow in artificial media or cell culture C. CLASSIFICATION 1. Distinguished by cultural features, biochemical reactions, and pathogenicity 2. Identification of species-specific rRNA and DNA sequences has resulted in the revision and expansion of the older phenotype-based classification system II. MYCOBACTERIAL DISEASE 1. Includes human and animal pathogens 2. Slowly progressive diseases 3. Lack exotoxins or endotoxins MYCOBACTERIUM TUBERCULOSIS I. BACTERIOLOGY 1. Growth takes weeks 2. Biochemical tests distinguish from other mycobacteria 3. Unusual resistance to drying and disinfectants but not to heat 4. Purified protein derivative (PPD) is mix of tuberculin proteins II. TUBERCULOSIS A. EPIDEMIOLOGY 1. Dominant infection of 18th and 19th centuries 2. Attack rates still high in many developing countries 3. Most infections are by respiratory route 4. Repeated coughing generates infectious dose into air 5. Poor ventilation increases risk 6. AIDS and drug resistance enhance spread B. PATHOGENESIS a. Primary Infection 1. Mycobacterium tuberculosis is an intracellular pathogen whose success depends on avoiding the killing mechanisms of professional phagocytes 2. MTB multiplies in alveolar macrophages 3. Acidification of phagosome blocked 4. TH1 responses triggered 5. MTB disseminates to lymph nodes and bloodstream 6. Cytokines attract T cells and TH1 response 7. MTB proteins also trigger DTH and injury 8. The granuloma includes macrophages, lymphocytes, fibroblasts 9. Caseous necrosis is due to DTH 10. Primary lesions heal once immunity develops 11. Some MTB enter dormant state rather than dying b. Reactivation (Adult) Tuberculosis 1. Dormant MTB reactivates at aerobic sites 2. Destruction forms pulmonary cavities 3. No toxins 4. Progressive delayed-type hypersensitivity (DTH) causes injury C. IMMUNITY 1. Innate immunity is high and genetically variable 2. TH1 immunity is most important 3. Cytotoxic CD8 lymphocytes may participate III. TUBERCULOSIS: CLINICAL ASPECTS A. MANIFESTATIONS a. Primary Tuberculosis 1. Mid-lung infiltrates and adenopathy are produced 2. Primary infection may progress to reactivation or dissemination b. Reactivation Tuberculosis 1. Reactivation is most common in older men 2. Predisposing factors include underlying disease and life events 3. Cough is universal 4. Cavities form in lung apices 5. Multiple organs are involved B. DIAGNOSIS a. Tuberculin Test 1. PPD test measures DTH to tuberculoprotein 2. Positive PPD indicates past or current infection 3. Anergy may develop with immune compromise 4. Predictive value depends on prevalence 5. BCG immunization compromises public health value b. Laboratory Diagnosis i. Acid-fast Smears 1. Mycobacteria are detected in direct smears of clinical material 2. Little more than half (~65%) of culture-positive sputum samples yield positive smears. 3. Contaminating mycobacteria may yield “false” positives in some specimens ii. Culture 1. Material contaminated with normal flora is chemically treated 2. Mucolytic agents used in sputum 3. Cultures take 3+ weeks 4. Radiometric procedures are faster 5. NAA Nucleic acid amplification (NAA) procedures lack sensitivity 6. Susceptibility testing essential C. TREATMENT 1. The term first-line is used to describe the primary drugs of choice (isoniazid, ethambutol, rifampin, pyrazinamide, streptomycin) which have long clinical experience 2. Resistance to first-line causes use of second-line drugs 3. Antimicrobics act intra and extracellularly 4. Resistance or toxicity may limit some agents 5. Multidrug therapy limits expression of resistance 6. Multidrug-resistant tuberculosis (MDR-TB) is resistant to isoniazid and rifampin 7. Treatment is 6-9 months 8. Resistance and HIV require longer 9. Compliance a major problem D. PREVENTION 1. Exposure and PPD conversion warrant isoniazid chemoprophylaxis 2. BCG is a live vaccine derived originally from a strain of M. bovis 3. BCG stimulates tuberculin DTH 4. BCG effectiveness is variable, contraindicated in AIDS MYCOBACTERIUM LEPRAE I. BACTERIOLOGY 1. Fails to grow in culture 2. Slow growth in animals II. LEPROSY A. EPIDEMIOLOGY 1. Nasal droplets transmit infection 2. Rare in North America B. PATHOGENESIS 1. In the tuberculoid form few M. leprae are seen in lesions, which are granulomatous with extensive epithelioid cells, giant cells, and lymphocytic infiltration 2. In lepromatous leprosy the cellular response is minimal, and growth of M. leprae is, thus, relatively unimpeded 3. Obligate intracellular parasite of macrophages and Schwann cells C. IMMUNITY 1. TH1 immunity determines extent of disease III. LEPROSY: CLINICAL ASPECTS A. MANIFESTATIONS a. Tuberculoid Leprosy 1. Skin and nerve involvement 2. Anaesthetic lesions b. Lepromatous Leprosy 1. Lesions are infiltrative and diffuse B. DIAGNOSIS 1. Acid-fast smears and biopsies are primary diagnostic methods C. TREATMENT AND PREVENTION 1. Sulfones combined with rifampin primary treatment is effective 2. Prevention requires early diagnosis and treatment of cases Other Mycobacterial Diseases I. MYCOBACTERIA CAUSING TUBERCULOSIS-LIKE DISEASES 1. Acquired from the environment; no case-to-case transmission 2. Resistance is common A. Mycobacterium kansasii 1. Resembles tuberculosis 2. Infection may cause PPD conversion B. Mycobacterium avium–Intracellulare Complex 1. MAC associated with birds and mammals 2. 2nd mycobacterial cause of disease in developed countries 3. Wide range of diseases; most common are pulmonary 4. Relative resistance to antituberculous drugs 5. Common complication of AIDS 6. Organisms isolated from blood C. Mycobacterium scrofulaceum 1. Granulomatous cervical lymphadenitis in children II. MYCOBACTERIAL SOFT TISSUE INFECTIONS A. Mycobacterium fortuitum Complex 1. Rapid growers cause abscesses and infections of prostheses B. Mycobacterium marinum 1. Cause of fish tuberculosis 2. Swimmer who abrades elbows or forearms in a pool develops a superficial granulomatous lesion that finally ulcerates C. Mycobacterium ulcerans 1. Occurs in tropical areas 2. Severe, progressive ulcerations require surgical removal