Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
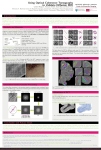
Photoreceptor cell wikipedia , lookup
Idiopathic intracranial hypertension wikipedia , lookup
Mitochondrial optic neuropathies wikipedia , lookup
Fundus photography wikipedia , lookup
Retinal waves wikipedia , lookup
Macular degeneration wikipedia , lookup
Diabetic retinopathy wikipedia , lookup
■ R E V I E W Optical Coherence Tomography in Pediatric Ophthalmology: Current Roles and Future Directions Tarek Alasil, MD; Pearse A. Keane, MD; Dawn A. Sim, MD; Adnan Tufail, MD; Michael E. Rauser, MD ABSTRACT: The application of existing optical coherence tomography (OCT) technology to the pediatric population is limited in both the design specification of the device and its hardware. However, the potential of OCT in the pediatric population has not been fully realized. The authors review the literature, highlighting the currently available spectral-domain OCT technology and summarizing the reported normal pediatric OCT parameters for retinal nerve fiber layer and macular thickness. They also review the pediatric ophthalmological conditions in which OCT has been used and discuss advancements in OCT design and their potential applications to the pediatric population. The use of OCT in pediatric populations is likely to increase greatly in the coming years, aiding clinical decision-making and providing new insights into pediatric disease pathophysiology. [Ophthalmic Surg Lasers Imaging Retina. 2013;44:S19-S29.] From the Department of Ophthalmology, Massachusetts Eye and Ear Infirmary, Boston, Massachusetts (TA); NIHR Biomedical Research Centre for Ophthalmology, Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology, London, United Kingdom (PAK, DAS, AT); and Department of Ophthalmology, Loma Linda University, Loma Linda, California (MER). Originally submitted February 11, 2013. Accepted for publication May 7, 2013. Drs. Keane and Tufail received a proportion of their funding from the Department of Health’s NIHR Biomedical Research Centre for Ophthalmology at Moorfields Eye Hospital and UCL Institute of Ophthalmology. Dr. Sim receives funding from Fight For Sight (UK), Grant 1987. The authors have no financial or proprietary interest in the materials presented herein. Address correspondence to Tarek Alasil, MD, Department of Ophthalmology, Massachusetts Eye and Ear Infirmary, 243 Charles Street, Boston, MA 02114. doi: 10.3928/23258160-20131101-04 November/December 2013 · Vol. 44, No. 6 (Suppl) ■ INTRODUCTION In the past decade, optical coherence tomography (OCT) has not only gained popularity in the practice of clinical ophthalmology, but its parameters serve as endpoint measures in many large multicenter clinical trials.1,2 The popularity of OCT is largely because of its properties as a noninvasive investigative technique, its speed of image acquisition, and its ability to provide clinically relevant and reproducible measures useful in the diagnosis and monitoring of disease. In adult populations, OCT was initially adopted for assessment of diseases with subtle clinical findings, such as abnormalities of the vitreoretinal interface.3 With the introduction of new pharmacotherapies for age-related macular degeneration (AMD), and more recently for retinal vascular diseases such as diabetic macular edema (DME), its use has become ubiquitous among retina specialists. In contrast, the use of OCT in pediatric populations has lagged behind that in adult populations. This may be explained in large part by the differing nature of diseases affecting pediatric populations, with the absence of a major disease such as neovascular AMD driving adoption. Limitations of OCT devices may also be a contributing factor, however, leading to difficulties in acquisition of OCT images in noncompliant younger children and infants. Furthermore, OCT image acquisition protocols are currently focused on scanning of the macula, a potential disadvantage given that many pediatric ophthalmic diseases involve extramacular pathologies. The application of existing OCT technology to the pediatric population is limited both in the design specification of the machine and in its hardware. The size of the machines, the height and position of their headrests, the time taken to acquire images, and sensitivity to small changes in positioning often preclude use in a moving child. As a result, OCT is sometimes performed in anesthetized children (an invasive requirement that significantly impacts the frequency of usage). In anesthesia, the requirement for supine positioning may also lead to changes in the anatomical positioning of normal ocular structures (eg, the lens and ciliary body) and fluctuations in pathologic features (eg, fluidic shifts in the cases of edema or subretinal fluid). This may affect OCT’s ability to accurately assess disease activity and make direct comparisons with adult populations difficult. Rapid advances in OCT technology, with enhanced image acquisition speeds and wide-field technology, S19 may allow OCT to be used as a routine investigative tool in the pediatric population in the near future. In this review, we summarize the pediatric ophthalmological conditions in which OCT has been used and discuss advancements in OCT design, and their potential applications in pediatric patients. surgery. The use of microscope-mounted SD-OCT has enabled wide-field noncontact real-time crosssectional imaging of retinal structure and augmented intrasurgical microscopy for intraocular visualization.9,10 This technology may be of particular interest for use in children. CURRENT TECHNOLOGY Anterior-Segment OCT Spectral-Domain OCT Stratus OCT (Carl Zeiss Meditec, Dublin, CA), the first OCT system to be widely adopted by ophthalmologists, provides images with relatively high axial resolution (~10 μm in tissue). However, the major limitation of Stratus OCT is its need for a moving reference mirror and thus a relatively slow image acquisition speed (400 A-scans per second). In Stratus OCT, A-scans are acquired as a function of time, and thus such devices are often referred to as timedomain OCT (TD-OCT). More recently, commercial OCT systems have employed techniques to measure OCT A-scans as a function of frequency, and this generation of OCT technology is referred to as spectral-domain or Fourier-domain OCT. The major advantage of this approach is a greatly enhanced image acquisition speed, 50 to 100 times faster than Stratus OCT.4 Greater speed also allows more of the retina to be sampled in a single image set and may also facilitate OCT image acquisition in pediatric populations. Commercially available spectral-domain OCT (SDOCT) devices (eg, Spectralis, Heidelberg Engineering, Germany) have also incorporated eye-tracking technology. Using this technology, multiple images can be obtained from the same location and averaged to enhance visualization of fine structures.5,6 Real-time eye tracking also compensates for many of the involuntary eye movements that can occur during image acquisition and result in motion artifacts, which may prove useful in poorly compliant pediatric populations. Anterior-segment OCT (AS-OCT) is a noninvasive technology capable of capturing high-resolution images of the anterior segment, particularly of the cornea and anterior chamber angles. Because ASOCT requires less patient cooperation relative to ultrasound biomicroscopy, it may prove particularly useful in pediatric populations.11 Despite this, its potential in this regard remains largely untapped. HEALTHY PEDIATRIC POPULATIONS SD-OCT has been successfully converted into a handheld device by disassembling the camera unit from the base (by removing the M6 Allen screw from the rotational bearing at the bottom of the arc guide). Subsequently, the camera head turns free and is supported by holding the camera handle at the back of the mount and gently lifting it off the base of the instrument. This modification enabled the imaging of supine and unanesthetized infants in the office.7,8 Intraoperative SD-OCT has provided new insight into the changes to retinal anatomy during macular To make full use of the OCT information, a comparison with age-matched population-derived normative data is needed to identify deviations from the normal range. Unfortunately, only limited information is available for healthy human populations younger than 18 years of age. Normative pediatric OCT data should facilitate the use of OCT in assessing childhood glaucoma and a variety of other pediatric ocular diseases. Using Stratus OCT, Samarawickrama et al., recently reported the results of the Sydney Childhood Eye Study, a population-based study examining childhood eye conditions in Australia.12 During the 2003-2005 period, students in grades 1 (median age: six years) and 7 (median age: 12 years) were examined. This study concluded that normal children, 6 and 12 years of age and of East Asian ethnicity, had a significantly thicker retinal nerve fiber layer (RNFL) — 3% and 12%, respectively — when compared to those of European Caucasian ethnicity (P < .001). El-Dairi et al collected a normative database of RNFL thicknesses in the eyes of 286 healthy children aged 3 to 17 years using Stratus OCT.13 Black children had a larger RNFL thickness, when compared with white children. Leung et al studied the normative RNFL thickness values of 104 children in Hong Kong, aged between 6 and 18 years, using Stratus OCT.14 In these children, the thickness of the RNFL showed a significant negative correlation with the axial length of the eye. Salchow et al measured the peripapillary RNFL thickness in 92 eyes of 92 healthy children (ages 4 to 17 years) by using OCT.15 They observed a large variation in RNFL thicknesses in healthy children, with a significant refractive effect on measurements. S20 Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina Handheld and Intraoperative OCT TABLE Stratus OCT RNFL normative values in pediatric populations Year Author N Ethnicity Age range (years) Average RNFL ± SD (μm) 2005 Ahn et al16 144 Korean 9 - 18 105.5±10.3 2006 Salchow et al15 92 92% Hispanic 4 - 17 107.0±11.1 2009 El-Dairi13 154 Black 109 White 2010 Leung MM14 194 Chinese 2010 Samarawickrama12 909 White 213 East Asian 2011 Qian23 398 Chinese 3 - 17 6 - 17 6 - 12 5 - 18 110.7±8.8 105.9±10.2 113.3±10.3 102.7±1.7 107.7±1.3 112.4±9.2 N = number of healthy eyes; RNFL = retinal nerve fiber layer thickness; SD = standard deviation. Ahn et al16 studied the RNFL thickness in 144 eyes of 72 healthy Korean children and adolescents (ages 9 to 18 years) using Stratus OCT. The mean RNFL thickness was 105.5 ± 10.3 μm. The Table summarizes the stratus OCT RNFL normative values in pediatric populations, which are similar to the range (99 to 103 μm) reported in the adult TD-OCT literature.17-22 Recent studies have used SD-OCT to evaluate RNFL thickness in healthy children. Turk et al24 reported an average RNFL thickness of 106.5 ± 9.4 μm in 107 healthy Turkish children. Tsai et al25 reported an average RNFL thickness of 109 ±10 μm in 470 healthy Chinese children. Those values are slightly higher than the adult range (97 to 102 μm) reported by SD-OCT studies.26-28 Using TD-OCT, Samarawickrama et al12 reported central macular thickness of 192.5 μm for the 6-yearold healthy group and 197.5 μm for the 12-year-old healthy group. El-Dairi et al reported the central macular thickness as 189 μm by using TD-OCT in healthy children. In their study, black children had a smaller macular volume and reduced foveal thickness when compared with white children.13 Turk et al reported central macular thickness of 211.4 μm in healthy children by using SD-OCT.24 AMBLYOPIA AND STRABISMUS Amblyopia is characterized by unilateral or bilateral decreased visual acuity, which is caused by abnormal binocular interaction or visual deprivation during the development of vision.29 There has been inconsistency about the involvement of the retina and optic nerve in amblyopia. Recent studies have used OCT in pediatric populations to investi- November/December 2013 · Vol. 44, No. 6 (Suppl) gate whether decreased visual acuity in amblyopia can be correlated with anatomical abnormalities in macula and RNFL. Al-Haddad et al studied the macular thickness in amblyopia using SD-OCT.30 Central macular thickness was significantly increased in children with anisometropic amblyopia. Anisometropia alone did not produce this difference, pointing to a possible correlation between amblyopia and the development of the retinal layers. Furthermore, Liu et al found that some children with various types of amblyopia who had failed to achieve normal visual acuity after treatment showed thickened RNFL in the macular area with no fovea on OCT examination.31 Interestingly, Pang et al concluded that children who have amblyopia and unilateral high myopia tend to have a thicker fovea and thinner inner and outer macula in the amblyopic eye compared with the healthy fellow eye.32 Future studies are warranted to determine whether the mechanism of the macular changes is due to high myopia, amblyopia, or a combination of the two. Many studies have demonstrated no difference in the OCT-measured RNFL thickness in amblyopic eyes compared with healthy fellow eyes of children with strabismic amblyopia.30,33,34 Yen et al observed a thicker RNFL in amblyopic eyes compared with sound eyes of children with anisometropic amblyopia.33 Nevertheless, Al-Haddad et al and Repka et al found no such difference.30,34 GLAUCOMA Diagnosis and monitoring of glaucoma are more difficult in children than adults because of the chal- S21 Figure 1. Spectralis optical coherence tomography retinal nerve fiber layer (RNFL) map of the left eye of a 15-year-old girl with juvenile glaucoma delineates the superotemporal and inferotemporal RNFL thinning. lenges in obtaining reproducible and reliable IOPs and visual fields in the pediatric population.35 Pediatric glaucoma is typically categorized by age of onset into three types: congenital (infants younger than 3 months old), infantile (between 3 months and 3 years of age), and juvenile (between 3 and 35 years of age). Infants with congenital or infantile glaucoma are usually examined under anesthesia because of the technical difficulties encountered with using OCT in such a noncompliant group of patients. Therefore, there is a lack of OCT literature in congenital and infantile glaucoma, whereas many OCT studies have evaluated children with juvenile glaucoma. Figure 1 demonstrates the Spectralis RNFL map of the left eye of a 15-year-old girl with juvenile glaucoma and delineates the superotemporal and inferotemporal RNFL thinning. Using Stratus OCT, children with juvenile glaucoma were found to have thinner RNFL and macula when compared to healthy peers.36 Furthermore, RNFL and macular thickness declined with progression of glaucomatous damage.37 Those findings support the value of OCT in the early diagnosis and monitoring of pediatric glaucoma. Retinopathy of prematurity (ROP) is characterized by vasoproliferative retinopathy and occurs almost exclusively in infants born prematurely. Maldonado et al found cystoid macular edema (CME) in more than half of the neonates with ROP by using handheld SD-OCT.38 Baker et al used OCT to study eyes with ROP that had no significant macular pathology on ophthalmoscopy and demonstrated subclinical changes in foveal anatomy, including relative loss of foveal depression, increased macular thickness, and preservation of inner retinal layers within the fovea.39 Macular abnormalities that are evident on OCT, which are not always seen on ophthalmoscopy, may explain poor visual outcome in many of these patients. It has been hypothesized that macular edema in eyes with severe ROP could be either a mechanical traction exerted on the macula or a response to biochemical modulators, including higher concentrations of vascular endothelial growth factor (VEGF), which could facilitate increased vascular permeability leading to retinal edema.38 In a study of 27 cytokines in the vitreous of 27 eyes of 19 infants with stage 4 ROP, VEGF was found to have the strongest correlation with vascular activity in the disease. Nevertheless, it is difficult to obtain vitreous samples from infants with ROP to monitor the progression of the disease.40 OCT provides a noninvasive alternative with the ability to detect traction on the macula and quantify macular edema. Future OCT studies should focus on whether the OCT morphological findings S22 Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina PEDIATRIC CHORIORETINAL VASCULAR DISEASE Retinopathy of Prematurity A B A B Figure 2. Fundus photograph (A) and optical coherence tomography (OCT) image (B) of the right eye of a 4-year-old girl with Coats’ disease. Fundus picture reveals dilated and telangiectatic blood vessels with exudation and severe lipid deposition in the macula. Longstanding submacular exudates stimulated in-growth of fibrous tissue or blood vessels, which lead to retinal pigment epithelial (RPE) migration and hyperplasia, the formation of RPE detachment seen on OCT. Intraretinal fluid collection is noted as well. can serve as a useful predictor of future visual acuity and development of visual pathway and cortical mapping. Measurement of choroidal thickness using OCT may also be of interest. Coats’ Disease Coats’ disease is an idiopathic disease characterized by vascular abnormalities of the retina. It typically presents as telangiectatic and aneurysmal retinal blood vessels associated with subretinal and intraretinal exudation and often subtotal or total exudative retinal detachment (Figures 2 and 3).41 Kaul et al used OCT to quantify the resolution of CME in a 16-yearold boy with Coats’ disease after intravitreal injection with anti-VEGF (pegaptanib sodium).42 Using OCT, the absence of vitreoretinal traction was confirmed in November/December 2013 · Vol. 44, No. 6 (Suppl) C Figure 3. Fundus photograph (A), optical coherence tomography (OCT) generated fundus image (B), and OCT image (C) of the right eye of a 16-year-old girl with Coats’ disease. Fundus picture reveals exudation and severe lipid deposition in the macula. OCT shows retinal pigment epithelial migration and hyperplasia, and the formation of fibrous scars. a full thickness macular hole encountered in a 9-yearold boy with Coats’ disease.43 Hence, the chronic macular exudation from telangiectatic vessels in the setting of Coats’ disease could have caused cystoid degeneration of the inner retinal layers and resulted in a full-thickness macular hole. S23 Figure 4. Fundus photograph and optical coherence tomography (OCT) image of the left eye of an 8-year-old boy with oculocutaneous albinism. Note the hypopigmented fundus. OCT demonstrated the persistence of an abnormal highly reflective band across the fovea, multiple inner retinal layers normally absent at the center of the fovea, and loss of the normally thickened photoreceptor nuclear layer usually encountered at the fovea. Choroidal Neovascularization Shaken-Baby Syndrome Kohly et al reported the results of pediatric choroidal neovascular membranes secondary to a variety of etiologies treated with intravitreal antiVEGF agents. Progress was monitored by clinical exam, OCT, and fluorescein angiography. By using OCT, they were able to quantitatively prove that anti-VEGF agents were effective in the treatment of pediatric choroidal neovascular membranes in this case series.44 Shaken-baby syndrome is an important complication of child abuse. It is most common in children younger than 3 years old. It has been reported that 30% to 40% of children subjected to child abuse will have ophthalmic sequelae.48 Hand-held SD-OCT can provide invaluable high-resolution imaging of the vitreoretinal interface and retina in infants with shaken-baby syndrome and reveal vitreoretinal abnormalities not easily detected on clinical examination that may be indicative of poor visual outcome.49,50 The most frequent OCT findings in shaken-baby syndrome were preretinal and multilayered retinal hemorrhages, perimacular folds, focal posterior vitreous separation with multilayered hemorrhagic retinoschisis, disruption of the foveal architecture, and foveolar detachment.48-51 Those OCT findings supported the pathophysiological theory of a direct mechanical effect caused by preretinal blood accumulation, localized vitreous detachment, and vitreoretinal traction. Toxoplasmosis Ocular toxoplasmosis results from retinal infection with the Apicomplexan protozoan Toxoplasma gondii. Toxoplasmic retinochoroiditis is the most common form of posterior uveitis in many countries.45 The infection can be congenital or acquired. Toxoplasma retinochoroiditis typically affects the posterior pole, and the lesions can be solitary, multiple or satellite to a pigmented retinal scar. Active lesions present as grey-white focus of retinal necrosis with adjacent choroiditis, vasculitis, hemorrhage, and vitritis. The prognosis of ocular toxoplasmosis is usually good in immunocompetent individuals, as long as the central macula is not directly involved.46 Garg et al used OCT to document the appearance of macular toxoplasmosis scars in 13 eyes of 10 consecutive patients (average age: 13 years).47 OCT features included retinal thinning, retinal pigment epithelial hyper-reflectivity, excavation, intraretinal cysts, and fibrosis. In patients with better than expected visual acuity, parafoveal lesions or an intact neurosensory layer were seen on OCT. S24 INHERITED RETINAL DISORDERS Albinism SD-OCT has been used to study the spectrum of foveal architecture in pediatric albinism and clarify the morphology of foveal hypoplasia seen clinically in ocular albinism (Figure 4). 52 Some of the abnormalities noted on OCT were the persistence of an abnormal highly reflective band across the fovea, multiple inner retinal layers normally absent at the center of the fovea, and loss of the Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina A B Figure 5. Cirrus high-definition optical coherence tomography (OCT) generated fundus image (A), and OCT image (B) of the right eye of a 9-year-old boy with Best’s disease: Yolk-like (vitelliform) lesion is noted in the central macula. Figure 6. Optical coherence tomography (OCT) image of the right eye of a 12-year-old girl with inherited retinal dystrophy. OCT demonstrated macular edema and delineated the hyporeflective cystoid spaces within the central macula. normally thickened photoreceptor nuclear layer usually encountered at the fovea. The optic nerve was also elevated in multiple eyes of individuals with ocular albinism.52 Leber Congenital Amaurosis Leber congenital amaurosis is an autosomal recessive inherited retinal degenerative disorder that causes an infant to be born with severely impaired vision. Photoreceptors are lost across a wide region of human central retina as early as the first decade of life in children with the disorder.53 Assessment of visual function is often difficult in infants, leading to a prominent role for electrodiagnostic testing such as electroretinography. OCT may function as an objective diagnostic tool by detecting foveal and extrafoveal photoreceptor loss early in the course of Leber congenital amaurosis. Differences in the topography of residual photoreceptors suggest that it may be advisable to use individualized outer nuclear layer mapping to guide the location of subretinal injections for gene therapy and thereby maximize the potential for efficacy.54 November/December 2013 · Vol. 44, No. 6 (Suppl) Best’s Disease Best’s disease is an autosomal dominant inherited type of macular dystrophy. It is identified by a large yellow yolk-like (vitelliform) lesion in the central macula. OCT can help define the characteristics of this “egg yolk” appearance (Figure 5). Furthermore, OCT has the ability to visualize CME that is associated with inherited retinal dystrophies (Figure 6). UVEITIS The majority of pediatric uveitis cases are idiopathic. Nevertheless, etiological factors can be ascertained in some cases, with juvenile idiopathic arthritis accounting for approximately 75% of all pediatric anterior uveitis.55,56 In a study of macular morphology and retinal complications of juvenile idiopathic arthritis–related uveitis in 24 eyes of 14 children, Stratus OCT was able to detect macular edema in 25% of the eyes, most of which was mild and not clinically evident.57 Because macular involvement could be underestimated by a traditional clinical examination, OCT might provide an S25 Figure 7. Optical coherence tomography (OCT) image of the left eye of an 11-year-old boy with intermediate uveitis. OCT demonstrated cystoid macular edema and delineated the hyporeflective cystoid spaces within the inner retinal layers. additional diagnostic tool with much higher sensitivity for detecting maculopathy as a significant complication of uveitis in children with juvenile idiopathic arthritis. Figure 7 shows OCT imaging of CME in the left eye of an 11-year-old boy with intermediate uveitis. OPTIC NERVE HEAD ANOMALIES OCT has been proven to measure the peripapillary RNFL thickness with excellent reproducibility,58 and its role in the diagnosis and monitoring of various optic nerve head anomalies has grown in the pediatric population. In comparison with healthy controls, an increased RNFL thickness was observed in children with pseudotumor cerebri,59 whereas RNFL measured thinner in the affected eyes of children with multiple sclerosis, acute disseminated encephalomyelitis, and optic neuritis.60 TUMORS diagnose OPGs in children. Using Stratus OCT, Chang et al63 found that NF1 subjects with OPGs had thinner RNFL (61 μm) and smaller macular volume (6.2 mm3) when compared with age-matched healthy control subjects (108 μm, 6.8 mm3) (P < .01). NF1 subjects without OPGs have equivalent RNFL thickness and macular volume as matched healthy control subjects. Therefore, OCT could be used as a noninvasive screening tool to determine the possibility of an OPG, thereby avoiding expensive MRI and possible risks of anesthesia in young children. OCT data can augment neuroimaging findings in children with NF1 with suspected or known OPGs when correlated with clinical examinations and visual field test findings. Critical OCT changes in RNFL and macular thicknesses can establish appropriate treatment timing in children with NF1 with vision-threatening OPGs. Using AS-OCT (Visante OCT 3.0; Carl Zeiss Meditec, Dublin, CA) in 200 eyes (including children), anterior segment tumors involving the iris stroma, ciliary body, iris pigment epithelium, conjunctiva, and sclera were imaged and compared to ultrasound biomicroscopy (OPKO Instrumentation/ OTI, Miami, FL). Ultrasound biomicroscopy provided superior visualization of the posterior margin and entire tumor configuration.64 OCT is more sensitive than clinical examination and ultrasonography in the detection of retinal thinning, cystoid and non-cystoid macular edema, subfoveal fluid, and surface wrinkling maculopathy.61 However, ultrasonography is more sensitive in detection of posterior vitreous detachment. 61 Shields et al used OCT in the evaluation of pediatric fundus lesions in retinal capillary hemangioma, astrocytic hamartoma, and retinoblastoma.61 Neurofibromatosis type 1 (NF1) is the most common neurocutaneous disorder, with an approximate incidence of one in 3,500.62 Optic pathway gliomas (OPG) develop in 15% of individuals with NF1, commonly in childhood, and are associated with significant visual risks. OPGs are difficult to detect via clinical inspection in children, often requiring magnetic resonance imaging. Therefore, there is a need for improved noninvasive techniques to Using Visante OCT, Bailey et al reported thicker ciliary body measurements with myopia and a longer axial length in children 8 to 15 years of age.65 This AS-OCT finding contradicted the choroidal expansion theory and raised the possibility that there is a physiological response of the ciliary body in myopia rather than simple mechanical stretching. Chow et al reported a case of secondary congenital aphakia diagnosed by using AS-OCT in a S26 Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina MISCELLANEOUS Figure 8. Optical coherence tomgoraphy image of the left eye in a 12-year-old girl with aniridia showing foveal hypoplasia and loss of the foveal depression seen in healthy individuals. CONCLUSION Figure 9. Wide-field swept-source optical coherence tomography (SS-OCT) image of the right eye of a healthy 25-year-old man. SS-OCT has the advantages of providing wide-field view and augmenting visualization of the choroids. 7-year-old boy with nystagmus.66 AS-OCT was of significant prognostic and management value, because it provided high-resolution images of the anterior segment and revealed the presence of lens capsules. The child later benefited from bilateral sulcus-fixated IOL implantation surgery. Intraoperative OCT confirmed the diagnosis of bilateral macular colobomata in a 3-year-old girl with Down syndrome.67 Congenital aniridia is a heritable disease characterized by an obvious iris defect, small cornea, small disc, decreased visual acuity with nystagmus, cataract, and foveal hypoplasia (Figure 8). November/December 2013 · Vol. 44, No. 6 (Suppl) The current generation of OCT technology is based on spectral-domain image acquisition. This involves the use of a spectrometer and a mathematical (Fourier) transformation to generate OCT A-scans as a function of frequency. The next generation of commercial OCT devices is likely to use swept-source technology to generate OCT images. With this approach, a tunable laser is used to generate OCT A-scans as a function of frequency. Sweptsource OCT devices will allow further increases in image acquisition speed.68 For example, DRI OCT1 (Topcon, Tokyo, Japan) will allow acquisition of approximately 100,000 A-scans per second. In fact, research prototypes using swept-source lasers are even faster, with some devices allowing millions of A-scans to be generated per second. This greatly enhanced image acquisition speed will be of particular interest for pediatric populations as it may facilitate wide-field imaging of the fundus, greatly enhancing visualization of extramacular pathologies. Sweptsource devices will also employ long-wavelength OCT light sources, which will greatly augment visualization of the choroid (Figure 9).69 Longitudinal measurements of the choroid may be of particular interest in children because the results from animal studies suggest an important role for this structure in ocular development.70 Greater OCT image acquisition speeds will also facilitate the development of “optical coherence angiography,” the use of OCT to provide noninvasive mapping of the retinal and/or choroidal microvasculature (this technique is also commonly referred to as “phase contrast” or “phase variance” OCT).68 With the exponential growth of these technologies, and their noninvasive nature, it seems clear that the use of OCT in pediatric populations is likely to increase greatly in the coming years, aiding clinical decision making and providing new insights into pediatric disease pathophysiology. S27 REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. S28 CATT Research Group, Martin DF, Maguire MG et al. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med. 2011;364(20):1897-1908. Nguyen QD, Brown DM, Marcus DM et al. Ranibizumab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology. 2012;119(4):789-801. Keane PA, Sadda SR. Imaging chorioretinal vascular disease. Eye (Lond). 2010;24(3):422-427. Kiernan DF, Mieler WF, Hariprasad SM. Spectral-domain optical coherence tomography: a comparison of modern high-resolution retinal imaging systems. Am J Ophthalmol. 2010;149(1):18-31. Hammer DX, Ferguson RD, Magill JC, White MA, Elsner AE, Webb RH. Compact scanning laser ophthalmoscope with highspeed retinal tracker. Appl Opt. 2003;42(22):4621-4632. Hammer DX, Ferguson RD, Magill JC, et al. Active retinal tracker for clinical optical coherence tomography systems. J Biomed Opt. 2005;10(2):024038. Vinekar A, Sivakumar M, Shetty R et al. A novel technique using spectral-domain optical coherence tomography (Spectralis, SDOCT+HRA) to image supine non-anaesthetized infants: utility demonstrated in aggressive posterior retinopathy of prematurity. Eye (Lond). 2010;24(2):379-382. Jung W, Kim J, Jeon M, Chaney EJ, Stewart CN, Boppart SA. Handheld optical coherence tomography scanner for primary care diagnostics. IEEE Trans Biomed Eng. 2011;58(3):741-744. Ray R, Barañano DE, Fortun JA, Schwent BJ, Cribbs BE, Bergstrom CS, Hubbard GB 3rd, Srivastava SK. Intraoperative microscope-mounted spectral domain optical coherence tomography for evaluation of retinal anatomy during macular surgery. Ophthalmology. 2011;118(11):2212-2217. Tao YK, Ehlers JP, Toth CA, Izatt JA. Intraoperative spectral domain optical coherence tomography for vitreoretinal surgery. Opt Lett. 2010;35(20):3315-3317. Chow VW, Wong AL, Fan DS. Use of anterior segment OCT in the evaluation and management of congenital aphakia. J Pediatr Ophthalmol Strabismus. 2009. Samarawickrama C, Wang JJ, Huynh SC, et al. Ethnic differences in optic nerve head and retinal nerve fiber layer thickness parameters in children. Br J Ophthalmol. 2010;94(7):871-876. El-Dairi MA, Asrani SG, Enyedi LB, Freedman SF. Optical coherence tomography in the eyes of normal children. Arch Ophthalmol. 2009;127(1):50-58. Leung MM, Huang RY, Lam AK. Retinal nerve fiber layer thickness in normal Hong Kong chinese children measured with optical coherence tomography. J Glaucoma. 2010;19(2):95-99. Salchow DJ, Oleynikov YS, Chiang MF, et al. Retinal nerve fiber layer thickness in normal children measured with optical coherence tomography. Ophthalmology. 2006;113(5):786-791. Ahn HC, Son HW, Kim JS, Lee JH. Quantitative analysis of retinal nerve fiber layer thickness of normal children and adolescents. Korean J Ophthalmol. 2005;19(3):195-200. Hougaard JL, Ostenfeld C, Heijl A, Bengtsson B. Modelling the normal retinal nerve fiber layer thickness as measured by Stratus optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2006;244(12):1607-1614. Sehi M, Ume S, Greenfield DS. Scanning laser polarimetry with enhanced corneal compensation and optical coherence tomography in normal and glaucomatous eyes. Invest Ophthalmol Vis Sci. 2007;48(5):2099-2104. Lu AT, Wang M, Varma R, et al. Combining nerve fiber layer parameters to optimize glaucoma diagnosis with optical coherence tomography. Ophthalmology. 2008;115(8):1352-1357. Budenz DL, Anderson DR, Varma R, et al. Determinants of normal retinal nerve fiber layer thickness measured by Stratus OCT. Ophthalmology. 2007;114(6):1046-1052. Varma R, Bazzaz S, Lai M. Optical tomography-measured retinal nerve fiber layer thickness in normal latinos. Invest Ophthalmol Vis Sci. 2003;44(8):3369-3373. Nagai-Kusuhara A, Nakamura M, Fujioka M, Tatsumi Y, Negi A. Association of retinal nerve fiber layer thickness measured by 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. confocal scanning laser ophthalmoscopy and optical coherence tomography with disc size and axial length. Br J Ophthalmol. 2008;92(2):186-190. Qian J, Wang W, Zhang X, et al. Optical coherence tomography measurements of retinal nerve fiber layer thickness in chinese children and teenagers. J Glaucoma. 2011;20(8):509-513. Turk A, Ceylan OM, Arici C. Evaluation of the nerve fiber layer and macula in the eyes of healthy children using spectraldomain optical coherence tomography. Am J Ophthalmol. 2012;153(3):552-559. Tsai DC, Huang N, Hwu JJ, Jueng RN, Chou P. Estimating retinal nerve fiber layer thickness in normal schoolchildren with spectral-domain optical coherence tomography. Jpn J Ophthalmol. 2012;56(4):362-370. Bendschneider D, Tornow RP, Horn FK, et al. Retinal nerve fiber layer thickness in normals measured by spectral domain OCT. J Glaucoma. 2010;19(7):475-482. Hirasawa H, Tomidokoro A, Araie M, et al. Peripapillary retinal nerve fiber layer thickness determined by spectral domain optical coherence tomography in ophthalmologically normal eyes. Arch Ophthalmol. 2010;128(11):1420-1426. Alasil T, Wang K, Keane PA, et al. Analysis of Normal Retinal Nerve Fiber Layer Thickness by Age, Sex, and Race Using Spectral Domain Optical Coherence Tomography. J Glaucoma. 2012. The Eye MD Association. Pediatric Ophthalmology and Strabismus. San Francisco: American Academy of Ophthalmology. 2006;67-75. Al-Haddad CE, Mollayess GM, Cherfan CG, Jaafar DF, Bashshur ZF. Retinal nerve fiber layer and macular thickness in amblyopia as measured by spectral-domain optical coherence tomography. Br J Ophthalmol. 2011;95(12):1696-1699. Liu H, Zhong L, Zhou X, Jin QZ. Macular abnormality observed by OCT in children with amblyopia failing to achieve normal visual acuity after long-term treatment. J Pediatr Ophthalmol Strabismus. 2010;47(1):17-23. Pang Y, Goodfellow GW, Allison C, Block S, Frantz KA. A prospective study of macular thickness in amblyopic children with unilateral high myopia. Invest Ophthalmol Vis Sci. 2011;52(5):2444-2449. Yen MY, Cheng CY, Wang AG. Retinal nerve fiber layer thickness in unilateral amblyopia. Invest Ophthalmol Vis Sci. 2004;45(7):2224-2230. Repka MX, Goldenberg-Cohen N, Edwards AR. Retinal nerve fiber layer thickness in amblyopic eyes. Am J Ophthalmol. 2006;142(2):247-251. El-Dairi MA, Asrani SG, Enyedi LB, Freedman SF. Optical coherence tomography in the eyes of normal children. Arch Ophthalmol. 2009;127(1):50-58. Hess DB, Asrani SG, Bhide MG, Enyedi LB, Stinnett SS, Freedman SF. Macular and retinal nerve fiber layer analysis of normal and glaucomatous eyes in children using optical coherence tomography. Am J Ophthalmol. 2005;139(3):509-517. El-Dairi MA, Holgado S, Asrani SG, Enyedi LB, Freedman SF. Correlation between optical coherence tomography and glaucomatous optic nerve head damage in children. Br J Ophthalmol. 2009;93(10):1325-1330. Maldonado RS, O’Connell RV, Sarin N et al. Dynamics of human foveal development after premature birth. Ophthalmology. 2011;118(12):2315-2325. Baker PS, Tasman W. Optical coherence tomography imaging of the fovea in retinopathy of prematurity. Ophthalmic Surg Lasers Imaging. 2010;41(2):201-206. Sato T, Kusaka S, Shimojo H, Fujikado T. Simultaneous analyses of vitreous levels of 27 cytokines in eyes with retinopathy of prematurity. Ophthalmology. 2009;116(11):2165-2169. Shields JA, Shields CL. Review: Coats disease: the 2001 LuEsther T. Mertz lecture. Retina. 2002;22(1):80-91. Kaul S, Uparkar M, Mody K, Walinjkar J, Kothari M, Natarajan S. Intravitreal anti-vascular endothelial growth factor agents as an adjunct in the management of Coats’ disease in children. Indian J Ophthalmol. 2010;58(1):76-78. Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina 43. Kumar V, Goel N, Ghosh B, Raina UK. Full-thickness macular hole and macular telangiectasia in a child with Coats’ disease. Ophthalmic Surg Lasers Imaging. 2010;4:e1-3. 44. Kohly RP, Muni RH, Kertes PJ, Lam WC. Management of pediatric choroidal neovascular membranes with intravitreal anti-VEGF agents: a retrospective consecutive case series. Can J Ophthalmol. 2011 Feb;46(1):46-50. 45. Furtado JM, Winthrop KL, Butler NJ, Smith JR. Ocular toxoplasmosis I: parasitology, epidemiology and public health. Clin Experiment Ophthalmol. 2012;41(1)82-94. 46. Bonfioli AA, Orefice F. Toxoplasmosis. Semin Ophthalmol. 2005;20(3):129-141. 47. Garg S, Mets MB, Bearelly S, Mets R. Imaging of congenital toxoplasmosis macular scars with optical coherence tomography. Retina. 2009;29(5):631-637. 48. Sturm V, Landau K, Menke MN. Optical coherence tomography findings in Shaken Baby syndrome. Am J Ophthalmol. 2008;146(3):363-368. 49. Koozekanani DD, Weinberg DV, Dubis AM, Beringer J, Carroll J. Hemorrhagic Retinoschisis in Shaken Baby Syndrome Imaged with Spectral Domain Optical Coherence Tomography. Ophthalmic Surg Lasers Imaging. 2010;1-3. 50. Muni RH, Kohly RP, Charonis AC, Lee TC. Retinoschisis detected with handheld spectral-domain optical coherence tomography in neonates with advanced retinopathy of prematurity. Arch Ophthalmol. 2010;128(1):57-62. 51. Scott AW, Farsiu S, Enyedi LB, Wallace DK, Toth CA. Imaging the infant retina with a hand-held spectral-domain optical coherence tomography device. Am J Ophthalmol. 2009;147(2):364-373. 52. Chong GT, Farsiu S, Freedman SF, et al. Abnormal foveal morphology in ocular albinism imaged with spectral-domain optical coherence tomography. Arch Ophthalmol. 2009;127(1):3744. 53. Bainbridge JW, Smith AJ, Barker SS, et al. Effect of gene therapy on visual function in Leber’s congenital amaurosis. N Engl J Med. 2008;358(21):2231-2239. 54. Jacobson SG, Cideciyan AV, Aleman TS, et al. Photoreceptor layer topography in children with leber congenital amaurosis caused by RPE65 mutations. Invest Ophthalmol Vis Sci. 2008;49(10):45734577. 55. Foster CS. Diagnosis and treatment of juvenile idiopathic arthritisassociated uveitis. Curr Opin Ophthalmol. 2003;14(6):395-398. 56. Levy-Clarke GA, Nussenblatt RB, Smith JA. Management of chronic pediatric uveitis. Curr Opin Ophthalmol. 2005;16(5):281-288. November/December 2013 · Vol. 44, No. 6 (Suppl) 57. Paroli MP, Spinucci G, Fabiani C, Pivetti-Pezzi P. Retinal complications of juvenile idiopathic arthritis-related uveitis: a microperimetry and optical coherence tomography study. Ocul Immunol Inflamm. 2010;18(1):54-59. 58. Wu H, de Boer JF, Chen TC. Diagnostic capability of spectraldomain optical coherence tomography for glaucoma. Am J Ophthalmol. 2012;153(5):815-826. 59. El-Dairi MA, Holgado S, O’Donnell T, Buckley EG, Asrani S, Freedman SF. Optical coherence tomography as a tool for monitoring pediatric pseudotumor cerebri. J AAPOS. 2007;11(6):564-570. 60. Yeh EA, Weinstock-Guttman B, Lincoff N, et al. Retinal nerve fiber thickness in inflammatory demyelinating diseases of childhood onset. Mult Scler. 2009;15(7):802-810. 61. Shields CL, Mashayekhi A, Luo CK, Materin MA, Shields JA. Optical coherence tomography in children: analysis of 44 eyes with intraocular tumors and simulating conditions. J Pediatr Ophthalmol Strabismus. 2004;41(6):338-344. 62. Listernick R, Ferner RE, Liu GT, Gutmann DH. Optic pathway gliomas in neurofibromatosis-1: Controversies and recommendations. Ann Neurol. 2007;61(3):189-198. 63. Chang L, El-Dairi MA, Frempong TA, et al. Optical coherence tomography in the evaluation of neurofibromatosis type-1 subjects with optic pathway gliomas. J AAPOS. 2010;14(6):511-517. 64. Bianciotto C, Shields CL, Guzman JM, et al. Assessment of anterior segment tumors with ultrasound biomicroscopy versus anterior segment optical coherence tomography in 200 cases. Ophthalmology. 2011;118(7):1297-1302. 65. Bailey MD, Sinnott LT, Mutti DO. Ciliary body thickness and refractive error in children. Invest Ophthalmol Vis Sci. 2008;49(10):4353-4360. 66. Chow VW, Wong AL, Fan DS. Use of anterior segment OCT in the evaluation and management of congenital aphakia. J Pediatr Ophthalmol Strabismus. 2009:1-2. 67. Aziz HA, Ruggeri M, Berrocal AM. Intraoperative OCT of bilateral macular coloboma in a child with Down syndrome. J Pediatr Ophthalmol Strabismus. 2011;48:e37-39. 68. Drexler W, Fujimoto JG. State-of-the-art retinal optical coherence tomography. Prog Retin Eye Res. 2008;27(1):45-88. 69. Keane PA, Ruiz-Garcia H, Sadda SR. Clinical applications of long-wavelength (1,000-nm) optical coherence tomography. Ophthalmic Surg Lasers Imaging. 2011;42 Suppl:S67-74. 70. Nickla DL, Wallman J. The multifunctional choroid. Prog Retin Eye Res. 2010;29(2):144-168. S29