Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
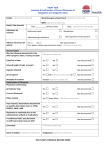
Agency Name/Logo Clinical Documentation Review Client name: Acct #: MR#: Other Disciplines: Date of Review Please Check One: Focused Review on Comprehensive Review for Orientation -- Review of SOC Time Period Reviewed: Primary HV Staff: SOC Date: Area: Reviewer: KEY to Focused Measures: Focus 1Focus 2 Focus 3 See Comments Directions: Put a check mark in one of the boxes (Yes, No, or NA) after every statement. Comments are optional. Y N N E O A S * A. Assessments and Planning (Incl. Recertifications) 1. For OASIS patients, Correct type of assessment is marked in MO100. 2. Medicare/Medicaid numbers on assessments match face sheets. 3. Assessment is complete and consistent, addressing all identified problems with interventions. 4. Primary and pertinent diagnoses match physical/psycho-social assessment, medication profile, past medical history, and active treatment plan & 485 (also, home care referral, if appropriate)? 5. Diagnoses are ranked appropriately based on assessment and plan of care? 6. Assessments support the need for ancillary service(aide, PDN, etc.), if being ordered, including level and extent of care, hours & frequency of service ordered, and the backup plan? 7. Assessments support correct payor selection (Medicare. Medicaid, HMO, Private, etc)? (Finance staff must be informed if there are any problems with insurance.) 8. Non-MO & PC assessment items are complete, including (but not limited to) correct use of S, O, NA, NP in observation areas, completion of pain assessment in Part G., use of Braden Scale, and documentation of wound size, description and location (incl. diagram) as appropriate to the patient. 9. Assessments reflect and support a clear, safe plan of care established with Patient/ PCG input. 10. Discussion of POC with the client/PCG is documented, including patient/primary care giver participation, and agreement (or disagreement)? 11. Discrepancies identified during assessments were clarified with physician and response documented? (Incl.: Medications, interventions, new problems/issues identified during assessment.) 12. Client specific emergency plan is developed and included in assessments and ancillary care plans. 13. Documentation of teaching done during assessment visits include what was taught, to whom it was taught, and the level of understanding demonstrated. 14. Documentation of homebound status is measurable and correlates to functional assessments. 15. Narratives on assessments summarize conclusions, impressions, and skilled interventions planned. * NA = Not Applicable (patient does not require this service, paperwork, etc.) CONFIDENTIAL Quality Review Tool: For Performance Improvement Use Only Y E S N O N A * Y E S N O N A * See Comments A. Assessments and Planning (Incl. Recertifications) con’t. 16. Plans established are reasonable and necessary, requiring skilled care (Nurse/PT/OT/SLP). 17. Plans for ancillary services are established jointly with patient/PCG and CHN. B. Physician Orders & Plan of Care 21. All 485s are present and signed. 22. 485 medical orders/interventions match the problems on assessments? (Interventions treatments/procedures, assessment, teaching, and evaluation & management.) 23. All appropriate disciplines, consistent with needs identified in the assessment, are listed on the 485s? 24. Frequency and duration for each discipline is based on identified client problems documented in the referral and/or assessment? 25. Ranges are based on client need and are reasonable? 26. Frequency and duration of service is stated in correct Medicare language? 27. PRN visits, when used, include number and specific client reason for visit(s)? 28. If client has daily care, a finite and predictable end date is documented? 29. For client with daily care, the ability and willingness of pt/PCG to learn and perform care is documented? 30. If aide service ordered, interventions match pt’s assessed needs and are listed in broad categories? 31. If PDN service is ordered, interventions include orders for specific treatments on activity sheet? 32. When needed, parameters are given for when Aide/PDN is to call the CHN (i.e. TPR). 33. 485 medical order goals match the interventions selected. 34. Goals are appropriate, measurable, based on assessment and include both short and long term goals with end dates? 35. Goals are updated/changed from certification period to certification period. 36. VSOC call documented and matches Locator box #23 on 485. 37. The update section provides a pertinent summary of patient information, is measurable and addresses progress towards goals. 38. Discharge plan is documented on 485. 39. An IMO is present for each change in POC. 40. All fields on each IMO are complete. * NA = Not Applicable (patient does not require this service, paperwork, etc.) CONFIDENTIAL Quality Review Tool-For Performance Improvement Use Only See Comments 18. Documentation reflects communication of assessment findings and POC across disciplines, including CHN to CHN, and PT/OT/SLP/SW, as appropriate. 19. Assessments indicate all ordered disciplines began services per MD Orders and per VHHC timeframe policy. 20. Discharge planning is evident in documentation at onset of case and ongoing. N O N A * Y E S N O N A * See Comments C. Medication Profile Y E S 41. Medications are written in the correct format and are legible. 42. When PRN medications ordered, reason for use is documented in the right column of the form. 43. All medications listed have a start date, and, where appropriate, a stop date. D. Progress Notes 48. Clinical Progress Notes are present documenting compliance with visit frequency as specified in 485 orders and matching billing history. 49. Progress Note documentation is complete, legible, dated, and signed. 50. Homebound determination re-evaluated by primary HV Staff is documented. 51. Clinical Progress Note documentation shows evidence of teaching and outcome of teaching 52. Clinical Progress Note documentation demonstrates client awareness, response to and participation in POC, and progression towards goals. 53. The established Plan of Care is followed as evidenced by documentation in the clinical record (i.e. vitals signs order, blood glucose regime, etc.) 54. Documentation reflects appropriate communication across disciplines at start of care and throughout Case management. 55. Documentation of patient care conferencing is present. 56. Progress towards and/or regression from goals is documented and coordination of care is evident. 57. Documentation reflects follow-through with identified patient problems. 58. Communications with MD are documented when patient’s condition warrants contact, incl.: Change in condition, lab values, variances in parameters from POC, (i.e. BGs, Vital Signs, O2 sats, etc.). 59. Ineffective visits are documented completely, including timely and appropriate follow-up calls to pt., Back-up, MD, TL or Area Manager. 60. Documentation reflects payor change as appropriate. 61. Discharge plan is documented and includes who, where, and how client will be cared for once home care service is no longer provided. (continued) * NA = Not Applicable (patient does not require this service, paperwork, etc.) CONFIDENTIAL Quality Review Tool-For Performance Improvement Use Only See Comments 44. Medication profile is complete, accurate and updated, including additions, deletions, and use of (N) or (C) to denote changes. 45. Allergy section is completed. 46. No medication for which the patient has a documented allergy is included on the medication list. 47. “Recorded by” signatures are present for any changes made on the Medication Profile. N O N A* Y E S N O N A* See Comments E. Ancillary Service Sheets (HHA, PDN, etc.): Y E S F. Miscellaneous 66. Client Information form present and complete. 67. Rate Agreement form present and complete. 68. Medical Necessity of SW is documented, i.e. SW needed to resolve social, emotional problems that are impeding (or are expected to impede) effective treatment or rate of recovery. 69. When warranted, the need for issuing a HHABN is identified within an acceptable timeframe, form is completed appropriately, including patient/patient representative’s signature and date. 70. Other (Specify): COMMENTS: Please number comments to correspond with question(s) being addressed. (if additional space needed, con’t on back.) * NA = Not Applicable (patient does not require this service, paperwork, etc.) CONFIDENTIAL Quality Review Tool-For Performance Improvement Use Only See Comments 62. Ancillary activity sheets present, complete and updated every 4 months (also should be done if case transferred to another CHN). 63. Ancillary service frequency and duration matches 485. 64. Ancillary service supervisions documented reflect agency protocol and required frequency. 65. HHA documentation of personal care is present.