Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
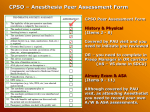
AUDIT TOOL Insertion & Confirmation of Correct Placement of Nasogastric and Orogastric Tubes Facility: Click here to enter text. Ward/Emergency Department: Click here to enter text. MRN: Click here to enter text. Gastric Tube inserted Indications for insertion Adverse outcome/s for patient Time: __ __: __ __ (24 hour clock) Date: Click here to enter a date. Nutritional needs ☐ Administering medications ☐ ☐ Rehydration ☐ Decompression of the stomach Yes ☐ No ☐ Not documented ☐ If so, please indicate type of adverse event: Click here to enter text. Documentation Was the following documented in the child’s progress notes / nursing care plan Click here to enter text. Type/Size of tube Yes ☐ No ☐ Not documented ☐ External length of tube at nostril Yes ☐ No ☐ Not documented ☐ Aspirate obtained Yes ☐ No ☐ Not documented ☐ pH of aspirate Yes ☐pHClick here to enter text. No ☐ Not documented Attempts at insertion Confirmation of Placement Placement confirmed by: Number Click here to enter text. Not documented ☐ pH indicator strip Yes ☐ No ☐ Not documented ☐ X-ray or Ultrasound Yes ☐ No ☐ Not documented ☐ Other method Yes ☐ State Which Click here to enter text. Post insertion, observations documented on specific observation chart i.e. SPOC, EDSPOC, SNOC, eMR Yes ☐ No ☐ Not documented ☐ Placement re-confirmed prior to the administration of fluids or medications Yes ☐ No ☐ Not documented ☐ If continuous feeds, was placement reconfirmed at least once per shift Yes ☐ No ☐ Not documented ☐ Comments: Click here to enter text. Name of Auditor: Click here to enter text. Designation: Click here to enter text. THIS IS NOT A MEDICAL RECORD FORM ☐ AUDIT TOOL Insertion & Confirmation of Correct Placement of Nasogastric and Orogastric Tubes COMPLETING THE AUDIT TOOL This audit tool accompanies the Insertion & Confirmation of Correct Placement of Nasogastric and Orogastric Tubes All dates are in DD/MM/YY format. All times are in HH:MM 24 hour clock format. All fields are mandatory and N/A is provided where required. Please use the comments box to record information which may assist in the data analysis. This includes explanations of blank fields etc. Do not use the comments box as a pathology or medical record. The name of auditor and designation boxes are to record the name of the person completing the form. THIS IS NOT A MEDICAL RECORD FORM