Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
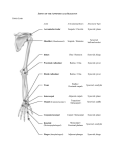
The pectoral girdle and bones of the free part of the upper limb form the superior appendicular skeleton. The pelvic girdle and bones of the free part of the lower limb form the inferior appendicular skeleton. The superior appendicular skeleton articulates with the axial skeleton only at the sternoclavicular joint, allowing great mobility. Connects the upper limb to the trunk. The shaft of the clavicle has a double curve in a horizontal plane. Its medial half is convex anteriorly, and its sternal end is enlarged and triangular where it articulates with the manubrium of the sternum at the sternoclavicular (SC) joint. Its lateral half is concave anteriorly, and its acromial end is flat where it articulates with the acromion of the scapula at the acromioclavicular (AC) joint. The clavicle Serves as a moveable, rigid support from which the scapula and free limb are suspended, keeping them away from the trunk so that the limb has maximum freedom of motion. Fixing the strut in position Forms one of the bony boundaries of the cervico-axillary canal (passageway between the neck and the arm), affording protection to the neurovascular bundle supplying the upper limb. Transmits shocks (traumatic impacts) from the upper limb to the axial skeleton. The conoid tubercle, near the acromial end of the clavicle, gives attachment to the conoid ligament, suspends the remainder of the upper limb is passively from the clavicle. Near the acromial end of the clavicle is the trapezoid line, to which the trapezoid ligament attaches. The subclavian groove (groove for the subclavius) in the medial third of the shaft of the clavicle is the site of attachment of the subclavius muscle. More medially is the impression for the costoclavicular ligament, a rough, often depressed, oval area that gives attachment to the ligament binding the 1st rib to the clavicle, limiting elevation of the shoulder. Scapula (Shoulder blade) A triangular flat bone Lies on the posterolateral aspect of the thorax, overlying the 2nd-7th ribs. The convex posterior surface of the scapula is unevenly divided by a thick projecting ridge of bone, the spine of the scapula, into a small supraspinous fossa and a much larger infraspinous fossa. The concave costal surface of most of the scapula forms a large subscapular fossa. The spine continues laterally as the flat expanded acromion (G. akros, point), which forms the subcutaneous point of the shoulder and articulates with the acromial end of the clavicle. The deltoid tubercle of the scapular spine is the prominence indicating the medial point of attachment of the deltoid. The spine and acromion serve as levers for the attached muscles, particularly the trapezius. Superolaterally, the lateral surface of the scapula has a glenoid cavity (G. socket), which receives and articulates with the head of the humerus at the glenohumeral joint. The beak-like coracoid process (G. korakōdés, like a crow's beak) is superior to the glenoid cavity. The scapula has medial, lateral, and superior borders and superior, lateral, and inferior angles. The glenoid cavity is the primary feature of the head. The shallow constriction between the head and the body defines the neck of the scapula. The largest bone in the upper limb Articulates with the scapula at the glenohumeral joint. Artciulates with the radius and ulna at the elbow joint. The proximal end of the humerus has a head, surgical and anatomical necks, and greater and lesser tubercles. The spherical head of the humerus articulates with the glenoid cavity of the scapula. The surgical neck of the humerus, a common site of fracture, is the narrow part distal to the head and tubercles. . The greater tubercle is at the lateral margin of the humerus, whereas the lesser tubercle projects anteriorly from the bone. The intertubercular (bicipital) groove separates the tubercles and provides protected passage for the slender tendon of the long head of the biceps muscle. The shaft of the humerus has two prominent features: the deltoid tuberosity laterally, for attachment of the deltoid muscle The oblique radial groove (groove for radial nerve, spiral groove) posteriorly, in which the radial nerve and deep artery of the arm lie. The inferior end of the humeral shaft widens as the sharp medial and lateral supraepicondylar (supracondylar) ridges form and then end distally in the especially prominent medial epicondyle and the lateral epicondyle, providing for muscle attachment. The distal end of the humerus—including the trochlea; the capitulum; and the olecranon, coronoid, and radial fossae—makes up the condyle of the humerus. The condyle has two articular surfaces: Laterally Capitulum (L. little head) for articulation with the head of the radius Medially Trochlea (L. pulley) for articulation with the proximal end (trochlear notch) of the ulna Anteriorly, the coronoid fossa receives the coronoid process of the ulna during full flexion of the elbow. Posteriorly, the olecranon fossa accommodates the olecranon of the ulna during full extension of the elbow. Superior to the capitulum anteriorly, a shallower radial fossa accommodates the edge of the head of the radius when the forearm is fully flexed. Bones of Forearm The two forearm bones serve together to form the second unit of an articulated mobile strut (the first unit being the humerus), with a mobile base formed by the shoulder, that positions the hand. However, because this unit is formed by two parallel bones, one of which (the radius) can pivot about the other (the ulna), supination and pronation are possible. This makes it possible to rotate the hand when the elbow is flexed. Stabilizing bone of the forearm Medial and longer of the two forearm bones. Its more massive proximal end is specialized for articulation with the humerus proximally and the head of the radius laterally. For articulation with the humerus, the ulna has two prominent projections: (1) olecranon, projects proximally from its posterior aspect (forming the point of the elbow). (2) coronoid process, projects anteriorly. The olecranon and coronoid processes form the walls of the trochlear notch. Inferior to the coronoid process is the tuberosity of the ulna for attachment of the tendon of the brachialis muscle. Inferior to the radial notch on the lateral surface of the ulnar shaft is a prominent ridge, the supinator crest. On the lateral side of the coronoid process is a smooth, rounded concavity, the radial notch, which receives the broad periphery of the head of the radius. Between the radial notch and the distal part of the coronoid process is a concavity, the supinator fossa. At the distal end of the ulna a small, conical ulnar styloid process. The ulna does not reach—and therefore does not participate in—the wrist (radiocarpal) joint. The radius is the lateral and shorter of the two forearm bones. Its proximal end includes a short head, neck, and medially directed tuberosity. Head of the radius articulation with capitulum of the humerus radial notch of the ulna The neck of the radius is a constriction distal to the head. The oval radial tuberosity is distal to the medial part of the neck and demarcates the proximal end (head and neck) of the radius from the shaft. The medial aspect of the distal end of the radius forms a concavity, the ulnar notch, which accommodates the head of the ulna. The radial styloid process is larger than the ulnar styloid process and extends farther distally. This relationship is of clinical importance when the ulna and/or the radius is fractured. The wrist, or carpus, is composed of eight carpal bones (carpals) arranged in proximal and distal rows of 4. These small bones give flexibility to the wrist. Augmenting movement at the wrist joint, the two rows of carpals glide on each other; in addition, each bone glides on those adjacent to it. From lateral to medial, proximal row of carpals Scaphoid (G. skaphé, skiff, boat) Lunate (L. luna, moon) Triquetrum (L. triquetrus, three-cornered) Pisiform (L. pisum, pea) From lateral to medial, distal row of carpals Trapezium (G. trapeze, table) Trapezoid Capitate (L. caput, head) Hamate (L. hamulus, a little hook) The proximal surfaces of the distal row of carpals articulate with the proximal row of carpals, and their distal surfaces articulate with the metacarpals. The metacarpus forms the skeleton of the palm of the hand between the carpus and the phalanges. It is composed of five metacarpal bones (metacarpals). Each metacarpal consists of a base, shaft, and head. Each digit has three phalanges except for the first (the thumb), which has only two; however, the phalanges of the first digit are stouter than those in the other fingers. Each phalanx has a base proximally, a shaft (body), and a head distally. Movement of the pectoral girdle involves the sternoclavicular, acromioclavicular, and glenohumeral joints, usually all moving simultaneously. Functional defects in any of the joints impair movements of the pectoral girdle. Mobility of the scapula is essential for free movement of the upper limb. The clavicle forms a strut that holds the scapula, and hence the glenohumeral joint, away from the thorax so it can move freely. The clavicle establishes the radius at which the shoulder (half of the pectoral girdle and glenohumeral joint) rotates at the SC joint. The 15-20° of movement at the AC joint permits positioning of the glenoid cavity that is necessary for arm movements. When testing the range of motion of the pectoral girdle, both scapulothoracic (movement of the scapula on the thoracic wall) and glenohumeral movements must be considered. Although the initial 30° of abduction may occur without scapular motion, in the overall movement of fully elevating the arm, the movement occurs in a 2:1 ratio: For every 3° of elevation 2° occurs at the glenohumeral joint 1° at the physiological scapulothoracic joint When the upper limb has been elevated so that the arm is vertical at the side of the head (180° of arm abduction or flexion), 120° occurred at the glenohumeral joint and 60° occurred at the scapulothoracic joint. Scapulohumeral rhythm The important movements of the pectoral girdle are scapular movements: Elevation and depression, Protraction (lateral or forward movement of the scapula) Retraction (medial or backward movement of the scapula) Rotation of the scapula A saddle type of synovial joint but functions as a ball-and-socket joint. Divided into two compartments by an articular disc. The disc is firmly attached to the anterior and posterior sternoclavicular ligaments, thickenings of the fibrous layer of the joint capsule, as well as the interclavicular ligament. The great strength of the SC joint is a consequence of these attachments. The SC joint is the only articulation between the upper limb and the axial skeleton, and it can be readily palpated because the sternal end of the clavicle lies superior to the manubrium of the sternum. ARTICULATION OF STERNOCLAVICULAR JOINT Sternal end of the clavicle articulates with Manubrium & 1st costal cartilage LIGAMENTS OF STERNOCLAVICULAR JOINT The strength of the SC joint depends on ligaments and its articular disc. Anterior & posterior sternoclavicular ligaments Interclavicular ligament Costoclavicular ligament MOVEMENTS OF STERNOCLAVICULAR JOINT Although the SC joint is extremely strong, it is significantly mobile to allow movements of the pectoral girdle and upper limb. During full elevation of the limb, the clavicle is raised to approximately a 60° angle. The acromioclavicular joint (AC joint) is a plane type of synovial joint, which is located 2-3 cm from the “point” of the shoulder formed by the lateral part of the acromion. ARTICULATION OF ACROMIOCLAVICULAR JOINT Acromial end of the clavicle articulates with Acromion of the scapula LIGAMENTS OF ACROMIOCLAVICULAR JOINT Acromioclavicular ligament strengthens the AC joint superiorly. Coracoclavicular ligament anchorsthe clavicle to the coracoid process. consists of two ligaments, the conoid and trapezoid ligaments, which are often separated by a bursa. LIGAMENTS OF ACROMIOCLAVICULAR JOINT Acromioclavicular ligament Coracoclavicular ligament MOVEMENTS OF ACROMIOCLAVICULAR JOINT The acromion of the scapula rotates on the acromial end of the clavicle. These movements are associated with motion at the physiological scapulothoracic joint. A ball-and-socket type of synovial joint Permits a wide range of movement; however, its mobility makes the joint relatively unstable. ARTICULATION OF GLENOHUMERAL JOINT Humeral head articulates with Genoid cavity of the scapula deepened slightly but effectively by the ring-like, fibrocartilaginous glenoid labrum (L., lip) LIGAMENTS OF GLENOHUMERAL JOINT Glenohumeral ligaments Coracohumeral ligament Transverse humeral ligament runs more or less obliquely from the greater to the lesser tubercle of the humerus, bridging over the intertubercular sulcus. The coraco-acromial arch is an extrinsic, protective structure formed by the inferior aspect of the acromion and the coracoid process of the scapula, with the coracoacromial ligament spanning between them. The coraco-acromial arch is so strong that a forceful superior thrust of the humerus will not fracture it; the humeral shaft or clavicle fractures first. MOVEMENTS OF GLENOHUMERAL JOINT The glenohumeral joint has more freedom of movement than any other joint in the body. The glenohumeral joint allows movements around three axes and permits flexion-extension, abduction-adduction, rotation (medial and lateral) of the humerus, and circumduction. BURSAE AROUND GLENOHUMERAL JOINT Several bursae (sac-like cavities), containing capillary films of synovial fluid secreted by the synovial membrane, are situated near the glenohumeral joint. Bursae are located where tendons rub against bone, ligaments, or other tendons and where skin moves over a bony prominence. The bursae around the glenohumeral joint are of special clinical importance because some of them communicate with the joint cavity (e.g., the subscapular bursa). Consequently, opening a bursa may mean entering the cavity of the glenohumeral joint. Subscapular Bursa The subscapular bursa is located between the tendon of the subscapularis and the neck of the scapula. Subacromial Bursa Sometimes referred to as the subdeltoid bursa, the subacromial bursa is located between the acromion, coraco-acromial ligament superiorly and joint capsule of the glenohumeral joint inferiorly. The elbow joint, a hinge type of synovial joint, is located 2-3 cm inferior to the epicondyles of the humerus. Trochlea & capitulum of the humerus articulate with the trochlear notch of the ulna and the head of the radius, respectively; therefore, there are humeroulnar and humeroradial articulations. LIGAMENTS OF ELBOW JOINT Collateral ligaments of the elbow joint Radial collateral ligament extends from the lateral epicondyle of the humerus and blends distally with the anular ligament of the radius. The medial, triangular ulnar collateral ligament extends from the medial epicondyle of the humerus to the coronoid process and olecranon of the ulna and consists of three bands: (1) the anterior cord-like band is the strongest, (2) the posterior fan-like band is the weakest, (3) the slender oblique band deepens the socket for the trochlea of the humerus. MOVEMENTS OF ELBOW JOINT Flexion and extension occur at the elbow joint. The long axis of the fully extended ulna makes an angle of approximately 170° with the long axis of the humerus. This angle is called the carrying angle, named for the way the forearm angles away from the body when something is carried. This angle permits the forearms to clear the hips in swinging movements during walking, and is important when carrying objects. This angle is 155–1800 or, if one uses the supplementary angle, usually 0–250. Supplementary angle the smaller angle of deflection. Supplementary angle = 1800 – carrying angle. Various authors have used term carrying angle for both angles. Another article MOVEMENTS OF ELBOW JOINT . Acta Med Okayama. 2009 Dec;63(6):359-65. Estimation of carrying angle based on CT images in preoperative surgical planning for cubitus deformities. Park S, Kim E. Department of Mechanical Engineering, Korea University, Seoul, Republic of Korea BURSAE AROUND ELBOW JOINT Only some of the bursae around the elbow joint are clinically important. The three olecranon bursae: Intratendinous olecranon bursa, sometimes present in the tendon of triceps brachii. Subtendinous olecranon bursa, located between the olecranon and the triceps tendon Subcutaneous olecranon bursa, located in the subcutaneous connective tissue over the olecranon. Proximal Radio-Ulnar Joint The proximal (superior) radio-ulnar joint is a pivot type of synovial joint that allows movement of the head of the radius on the ulna. The head of the radius articulates with the radial notch of the ulna. The radial head is held in position by the anular ligament of the radius. MOVEMENTS OF PROXIMAL RADIO-ULNAR JOINT During pronation and supination of the forearm, the head of the radius rotates within the collar formed by the anular ligament and the radial notch of the ulna. The distal (inferior) radio-ulnar joint is a pivot type of synovial joint. The radius moves around the relatively fixed distal end of the ulna. ARTICULATION OF DISTAL RADIO-ULNAR JOINT The head of the ulna articulates with the ulnar notch of the radius. The articular disc separates the cavity of the distal radio-ulnar joint from the cavity of the wrist joint. LIGAMENTS OF DISTAL RADIO-ULNAR JOINT Anterior and posterior ligaments strengthen the fibrous layer of the joint capsule of the distal radio-ulnar joint. MOVEMENTS OF DISTAL RADIO-ULNAR JOINT During pronation of the forearm and hand, the distal end of the radius moves (rotates) anteriorly and medially, crossing over the ulna anteriorly. During supination, the radius uncrosses from the ulna, its distal end moving (rotating) laterally and posteriorly so the bones become parallel. The wrist (radiocarpal) joint is a condyloid (ellipsoid) type of synovial joint. The position of the joint is indicated approximately by a line joining the styloid processes of the radius and ulna, or by the proximal wrist crease. The wrist (carpus), the proximal segment of the hand, is a complex of eight carpal bones, articulating proximally with the forearm via the wrist joint and distally with the five metacarpals. ARTICULATION OF WRIST JOINT The ulna does not participate in the wrist joint. The distal end of the radius and the articular disc of the distal radioulnar joint articulate with the proximal row of carpal bones, except for the pisiform. LIGAMENTS OF WRIST JOINT The fibrous layer of the joint capsule is strengthened by strong dorsal and palmar radiocarpal ligaments. The joint capsule is also strengthened medially by the ulnar collateral ligament, which is attached to the ulnar styloid process and triquetrum. The joint capsule is also strengthened laterally by the radial collateral ligament, which is attached to the radial styloid process and scaphoid. MOVEMENTS OF WRIST JOINT The movements at the wrist joint may be augmented by additional smaller movements at the intercarpal and midcarpal joints. The movements are flexion—extension, abduction—adduction (radial deviation-ulnar deviation), and circumduction. JOINTS OF THE HAND