Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Prescription costs wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
Discovery and development of non-nucleoside reverse-transcriptase inhibitors wikipedia , lookup
Polysubstance dependence wikipedia , lookup
History of general anesthesia wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Neuropharmacology wikipedia , lookup
Drug interaction wikipedia , lookup
Psychopharmacology wikipedia , lookup
Drug discovery wikipedia , lookup
Plateau principle wikipedia , lookup
Theralizumab wikipedia , lookup
Pharmacognosy wikipedia , lookup
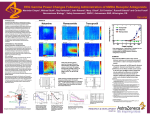
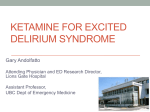
Development of Rapidly Metabolized and Ultra-Short-Acting Ketamine Analogs Martyn Harvey, MD, FACEM,* Jamie Sleigh, MD,* Logan Voss, PhD,* Jiney Jose, PhD,† Swarna Gamage, PhD,† Frederik Pruijn, PhD,† Sarath Liyanage, PhD,† and William Denny, PhD† BACKGROUND: Ketamine is a well-established, rapidly acting dissociative anesthetic. Clinical use is limited by prolonged psychotomimetic phenomena on emergence, often requiring the coadministration of additional hypnotic drugs. We hypothesized that the development of ketamine ester analogs with ultrashort offset times might markedly reduce the dysphoric emergence phenomena and, hence, increase the utility of a ketamine-like hypnotic and analgesic. Here, we describe the results of studies that seek to define the pharmacology of 5 esters of ((1-(2-chlorophenyl)-2-oxocyclohexyl)amino)pentanoate hydrochloride, the first ketamine analogs designed to be susceptible to ultrarapid metabolism. METHODS: Five norketamine ester analogs (R1–R5) were compared by ability to produce loss of righting and nociceptive blunting in rats. Toxicity testing was performed for 2 analogs (R1, R5) with 50% lethal dose (LD50) estimation in rats. In vitro metabolic stability was tested in rabbit plasma and whole blood by high-performance liquid chromatography. Behavioral and hemodynamic effects were observed in rabbits. We estimated the pharmacokinetics of these analogs in rabbits. RESULTS: All 5 norketamine esters produced rapid loss of righting reflex and diminished pedal withdrawal with ultrarapid offset in the models studied (return of righting reflex 87 seconds [interquartile range (IQR) 78–131] R1 vs 996 seconds [IQR 840–1304] ketamine in rats; P < 0.01). The LD50 was comparable to that of ketamine (LD50 R1 50.2 mg/kg [95% confidence interval, 30–63]). For all analogs, hydrolysis to sole carboxylic acid derivatives was most rapid in vivo (clearance 1.61 L/kg/min R1 [IQR 0.40–2.42]), followed by whole blood and then plasma. Analog R5 demonstrated relatively greater nociceptive blunting than hypnotic effect (P < 0.001; pedal withdrawal score comparison with R1). CONCLUSIONS: The 5 norketamine ester analogs retain the hypnotic characteristics of the parent compound, yet display rapid offset due to ultrarapid metabolism. (Anesth Analg 2015;XXX:00–00) K etamine [racemic (2-(2-chlorophenyl)-2-(methylamino) cyclohexanone] is a dissociative anesthetic with profound analgesic and sympathomimetic properties. It has major advantages over opioids: minimal respiratory depression, preservation of protective airway reflexes, no hyperalgesic effects, a reduction in analgesic tolerance, and efficacy in opioid-resistant pain.1,2 Analgesic effects are achieved at approximately 400 ng/mL.3 A dissociative anesthetic state develops when the plasma concentration exceeds 2000 ng/mL. The most important adverse effects of ketamine are its psychotomimetic properties, which occur at drug concentrations of just 100 ng/mL.4 Because ketamine has an elimination half-life of 2 to 3 hours,2,5,6 patients may experience prolonged (20–120 minutes) psychic disturbances after anesthesia. This limits the clinical utility of ketamine in adults. Ketamine analogs with very rapid clearance might limit the psychomimetic period to only a few minutes. From the *Waikato Clinical School, University of Auckland, Hamilton, New Zealand; and †Auckland Cancer Society Research Center, School of Medical Sciences, Auckland, New Zealand. Accepted for publication January 12, 2015. Funding: Biopharma funding Grant No 76650. Conflict of Interest: See Disclosures at the end of the article. Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s website (www.anesthesia-analgesia.org). Reprints will not be available from the authors. Address correspondence to Martyn Harvey, MD, FACEM, Emergency Department, Waikato Hospital, Pembroke St., Hamilton, New Zealand. Address e-mail to [email protected]. Copyright © 2015 International Anesthesia Research Society DOI: 10.1213/ANE.0000000000000719 XXX 2015 ڇVolume XXX ڇNumber XXX This would reduce the need for adjunctive hypnotics and extend the utility of such ketamine-like compounds, particularly in remote locations where analgesia is important, such as the radiological suite, the emergency department, or an out-of-hospital accident scene. We pursued a strategy similar to “soft” designer drugs (remifentanil,7 remimazolam,8,9 methoxycarbonyl-etomidate10,11), to create pharmacologically active esters that would be rapidly inactivated via hydrolysis to inactive metabolites. Our initial experience with development and testing of these agents has been described elsewhere.12 From these experiments in rodents, 5 norketamine ester analogs were identified with ketamine-like sedative effects but with significantly reduced duration of action. In this study, we determined the behavioral effects in rats and rabbits. We also characterized the in vivo toxicity in rats and pharmacokinetic characteristics in rabbits. METHODS Animals Animal studies were conducted at the Ruakura Animal Research Center, Hamilton, New Zealand. All experimental protocols were reviewed and approved by the Ruakura Animal Ethics Committee. Adult female Sprague-Dawley rats (350–400 g) were obtained from breeding stock from the Ruakura site. Adult male New Zealand white rabbits (2910–3340 g) were purchased from a credentialed supplier and quarantined at the Ruakura site for 3 weeks before use. All animals were housed in gender-specific enclosures with no chance of pregnancy. Standard, 12-hour day–night www.anesthesia-analgesia.org 1 Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited. Ketamine Analog Development lighting was maintained, and free access to feed and water was allowed until the day of the animal study. Synthesis of N-Alkylated Norketamine Esters R1 to R5 We previously reported our initial synthesis and screening of 24 norketamine analog test compounds12 and identified 5 of these compounds as having the most desirable characteristics of potent sedative effects with rapid offset. In this report, the following alkylated norketamine esters were interrogated for behavioral effects and toxicity in rats, and behavioral effects and pharmacokinetic analysis in rabbits: SN35210 = racemic-methyl 4-((1-(2-chlorophenyl)2-oxocyclohexyl)amino)pentanoate hydrochloride (R1); SN35371 = (S)-methyl 4-((1-(2-chlorophenyl)-2-oxocyclohexyl)amino)pentanoate hydrochloride (R2); SN35476 = racemic ethyl 3-((1-(2-chlorophenyl)-2-oxocyclohexyl)amino) propanoate hydrochloride (R3); SN35486 = racemic isopropyl 4-((1-(2-chlorophenyl)-2-oxocyclohexyl)amino)butanoate hydrochloride (R4); and SN35563 = racemic isopropyl 3-((1-(2-chlorophenyl)-2-oxocyclohexyl)amino)propanoate hydrochloride (R5). The compounds of interest were synthesized from norketamine, prepared from commercially available (2-chlorophenyl)(cyclopentyl)methanone.13 Esters were then prepared by treatment of norketamine with the appropriate alkyl halides Br(CH2)nCO2(CH2)R, and converted to the hydrochloride salts with HCl gas (Fig. 1). Purity was determined by high-performance liquid chromatography (HPLC) monitoring at 272 nm and was ≥95% for all compounds. Enantiomeric purity was analyzed by chiral HPLC (Chiralcel OJ-H column, 0.46 × 45 cm) (Chiral Technologies, Illkirch, France). The mobile phase was 85% hexane/15% EtOH (v/v) with a flow rate of 0.6 mL/min. The purity for R2 was determined by monitoring at 254 and 280 nm and was ≥95%. All compounds were solubilized in 0.9% saline solution before administration. Synthesis of N-Alkylated Norketamine Carboxylic Acids M1 to M5 N-Alkylated norketamine esters (R1–R5) and sodium hydroxide solution were dissolved in MeOH/EtOH. The reaction mixture was stirred at 50°C overnight. After completion of reaction, the solvent was evaporated and the residue obtained was acidified with 2 N HCl in ether. EtOAc was added to the above solution and stirred for 5 minutes. The solution was filtered, and the filtrate was evaporated to obtain a white solid that was triturated with EtOAc and filtered, and then dried to obtain the product as white solid. The purity of the carboxylic acids (M1–M5) was determined by monitoring at 254 and 280 nm and was ≥95% for all compounds. All compounds were synthesized by the laboratory of the Auckland Cancer Society Research Centre, Auckland, New Zealand. Calibration Standards/Analysis Final products were analyzed by reverse-phase HPLC (Alltima C18 5-μm column, 150 × 3.2 mm; Alltech Associated, Inc., Deerfield, IL) using an Agilent 1100 LC equipped with a diode array detector. The mobile phase was 80% CH3CN/20% H2O (v/v) in 45 mM HCO2NH4 at pH 3.5 and 0.5 mL/min. Calibration for each compound was performed using 100% fetal calf serum spiked with a range of ester/carboxylic acid concentrations (1–3, 10, 30, 60, and 100 μM). Concentrations of norketamine esters and carboxylic acids for subsequent in vitro and in vivo experiments were determined by HPLC analysis using the above parameters. After thawing, all experimental samples were Figure 1. Synthesis of study drugs (R1– R5) from norketamine (1). Structure of ketamine provided for comparison. All analogs are racemic save R2, which is the S-enantiomer of R1. Me = methyl; Et = ethyl; iPr = isopropyl. 2 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited. completely dried in a vacuum evaporator, and 75 μL of 1:3 acetonitrile formate buffer (0.45 M, pH 4.5) was added, vortexed, and centrifuged again; 50 μL was injected to HPLC. Standard curves were prepared from known stock solutions of the compounds to determine HPLC area peaks for each for the 5 compounds and for the 4 carboxylic acids. Standard curves were estimated by linear regression. The regression curves were used to determine the relevant concentrations of test compounds via correlation with measures of HPLC peaks. The lowest stock concentration for each analyte was variably 1to 3 μM. Concentrations below this were extrapolated to 0. The lowest recorded values for the esters were: R1 0.1 μM, R2 0.21 μM, R3 0.31 μM, R4 2.29 μM, and R5 0.86 μM. The lowest recorded carboxylic acid concentrations were M1 4.95 μM, M2 5.49 μM, M3/M5 6.29 μM, and M4 3.65 μM. Each test sample was assayed only once for ester and carboxylic acid. The method does not readily provide for determination of variability coefficients. Behavioral Effects in Rats Norketamine esters were evaluated for effect on responsiveness (hypnosis/analgesia) in rats. Sedative activity (demonstrated primarily by loss of righting reflex [LORR]) and nociceptive blunting (demonstrated by attenuation of pedal withdrawal score [PWS], a graduated response to standardized digital pressure [Supplemental Digital Content 1, http://links.lww.com/AA/B94, Table 1]) served as key outcome measures. Using a crossover experimental design, each norketamine analog was compared with ketamine in the same 3 animals (total 15 rats). An interval of 24 hours was allowed between agent evaluation. Rats were restrained in a 3-inch-diameter, 9-inch-long acrylic chamber and underwent venous cannulation of a lateral tail vein. Mini-bore extension tubing was attached, and the animal was released to a solitary enclosure. Infusion of study agents (R1–R5) at 10 mg/mL was begun at 20 mg/kg/min and maintained until LORR (defined as inability of the animal to spontaneously right from a position of dorsal recumbency to that of sternal recumbency). Thereafter, the infusion was continued at identical rate until the animal exhibited a PWS of 1.1 On reaching a PWS of 1, the infusion was decreased to 6.7 mg/kg/min and titrated in an up-and-down fashion (increment or decrement of 1 mg/kg/min at 30-second intervals) in an attempt to maintain a goal level of sedation defined as constant LORR and stable PWS of 1. Infusions were continued for a total of 10 minutes before cessation. Righting reflex status and PWS were recorded at 1-minute intervals from commencement until these parameters returned to baseline. Sedation index (defined as weightadjusted mean drug dose [mg] per minute of righting reflex loss) and nociceptive index (defined as weight-adjusted mean analog dose [mg] per unit decrease in PWS score from baseline) were computed to enable comparison of in vivo potency. Time from cessation of infusion to return of righting reflex was recorded. Toxicity: IV LD50 Determination Determination of 50% lethal dose (LD50) by the IV route for norketamine esters R1 and R5 was performed in 14 female Sprague-Dawley rats weighing 280 to 320 g. After XXX 2015 ڇVolume XXX ڇNumber XXX catheterization of the lateral tail vein, study drugs were injected for 30 seconds. Initial drug dosing was at 9.5 mg/kg with subsequent dosing in accord with the AOT 425 statistical programa using an up-and-down methodology for LD50 determination. All drugs were administered in 1 mL of 0.9% saline solution regardless of dosage. Limb lead electrocardiogram and visual inspection of respiratory effort was monitored throughout. Death was confirmed by the absence of respiratory and cardiac activity. Metabolic Stability in Plasma and Whole Blood The metabolic stability of the norketamine esters was tested in rabbit plasma and whole blood. For each compound, 20 mL of whole blood was drawn from arterial puncture of the central ear artery from one male New Zealand white rabbit. Animals were then returned to enclosures and later used for study no less than 2 weeks later. Blood was anticoagulated (100 IU heparin) and divided. A volume of 10 mL of whole blood was centrifuged at 2300g for 3 minutes, with plasma then pipetted from underlying red call mass and buffy coat. At time 0, study drugs were added to plasma/whole blood to a concentration of 0.0335 mg/mL (approximately 100 μM). Plasma/whole blood was then continuously vortexed at 37°C. At time equals 1, 3, 5, 10, and 20 minutes, 0.3-mL samples were withdrawn and immediately added to equal volumes of ice-cold acetonitrile (Sigma-Aldrich Co, St Louis, MO) to arrest metabolic activity. Samples were manually agitated before undergoing centrifugation at 9000g for 4 minutes, before aliquoting, and freezing at −80°C before analysis. Norketamine ester concentrations (R1–R5) and corresponding norketamine carboxylic acid (M1–M5) concentrations were determined by HPLC analysis according to the method described above. Behavioral Effects and Population Pharmacokinetic Evaluation in Rabbits Preliminary pharmacokinetic analysis of the norketamine eaters R1 to R5 was conducted in 5 male adult New Zealand white rabbits (average weight of 3.07 kg; range 2.91–3.34 kg) after rapid loading and subsequent maintenance infusions. Norketamine esters and ketamine were evaluated in the same animals at an interval of at least 3 days to minimize intersubject variation in behavioral and pharmacokinetic metrics. Venous cannulation of the marginal ear vein was undertaken for the purpose of study drug administration. Arterial cannulation of both ears was performed to enable continuous invasive monitoring of hemodynamic variables and arterial blood sampling. Ketamine or norketamine esters at 10 mg/mL were infused at the rate of 20 mg/kg/min to LORR (nominally time 0). Thereafter, infusion rates were reduced to 2 mg/kg/min and continued to 10 minutes before cessation. Assessment of behavioral parameters (LORR, PWS, anesthetic score [a 6-point score describing levels of rabbit anesthesia14; Supplemental Digital Content 2, http://links.lww.com/ AA/B95, Table 2]), and hemodynamic parameters were obtained at 1-minute intervals. During and after the infusion, blood was sampled via arterial catheter at 1, 3, 5, 10, 11, Available at: http://www.epa.gov/oppfead1/harmonization/. Accessed December 2013. a www.anesthesia-analgesia.org 3 Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited. Ketamine Analog Development Table 1. Norketamine Ester In Vivo Potency and Speed of Offset in Rats Dose to LORR (mg/kg) Dose to PWS =1 (mg/kg) SI NI Time to righting from cessation infusion (sec) R1 29.4 (23.9–47.5) 45.1 (27.3–60) 11.3 (10.1–11.3) 6.4 (6.3–7.2) 87* (78–131) R2 38.4 (30.5–38.9) 41.8 (40.5–48.6) 19.7 (17.9–25.5) 10.6 (9.0–15.3) 110* (60–115) R3 25.6 (24.6–94.1) 31.6 (27.8–105.9) 14.8 (10.9–32.5) 6.6 (4.8–19.5) 133* (118–280) R4 43.8 (25.6–55.3) 73.6 (34.4–91.6) 18.1 (13.1–18.4) 11.3 (9.2–24.1) 20* (10–80) R5 32.6 (23.4–43.2) 39.7 (25.7–44.6) 14.7 (9.9–24.5) 4.7 (3.9–5.1) 68* (60–120) Ketamine 20.3 (17.2–26.1) 25.8 (20.8–30.5) 4.3 (3.6–4.6) 1.6 (1.5–2.1) 996 (840–1304) All data = median (IQR). LORR = loss of righting reflex; PWS = pedal withdrawal score; SI = sedation index; NI = nocioceptive index. *P < 0.01, comparison with ketamine 13, 15, 20, and 40 minutes. Whole blood samples of 0.3 mL were immediately spiked with 0.3 mL ice-cold acetonitrile and manually agitated to effect complete precipitation of proteins. Samples were than centrifuged at 9000g for 4 minutes and the supernatant aliquotted before freezing at −80 °C until analysis by HPLC for study agent and acid metabolite according to the method described above. Basic pharmacokinetic parameters, clearance (CL), volume of distribution (V), and elimination half-life (t½), were calculated from the arterial concentrations of norketamine analogs R1 to R5. A 1-compartment population (i.e., all-in) pharmacokinetic model was used (FOCE-L-B algorithm) with the NLME7 engine in Phoenix NMLE 1.1 (Pharsight Corporation, St Louis, MO). Because the data were well described by a 1-compartment model, we did not undertake evaluation using further compartmental analysis. The model parameter and associated error estimates (theta values) reported all returned relatively small error estimates. In addition, visual inspection of the fitted data and the numerous residual plots all confirmed good and statistically sound model fits. Preliminary modeling of pharmacokinetic (PK)– pharmacodynamic (PD) parameters was furthermore performed using a sigmoid Emax model. Simulations of the plasma concentrations of norketamine esters R1 to R5 based on population PK metrics were constructed and linked to PD models of PWS and anesthetic scores. Statistical Analysis Statistical analyses were conducted using GraphPad Prism 5.0 (GraphPad Software Inc., La Jolla, CA). All data are reported as median (interquartile range) unless otherwise stated. Comparison of time metrics was conducted using the Mann-Whitney statistic. Continuous metrics were compared over time using 2-way repeated measures analysis of variance. A P value of <0.05 was deemed statistically significant. RESULTS Responsiveness in Rats with Norketamine Ester Infusion All agents (R1–R5) demonstrated lesser in vivo potencies with a 1.5- to 2-fold increase in dosing required to reach LORR and PWS end points compared with ketamine. Consistent with hypothesized rapid metabolism, all analogs demonstrated lightening of sedation after cessation of the initial rapid infusion, therefore requiring upward titration of subsequent maintenance infusion rates. Recovery, as demonstrated by 4 www.anesthesia-analgesia.org return of righting reflex, was approximately 10 times faster than ketamine for all the norketamine esters. Dose to LORR and dose to a PWS of 1, sedation and nociceptive indices, and time to regaining righting reflex for all agents are presented in Table 1. The quality of sedation achieved with ketamine analog infusion differed between agents. In particular, R1 exhibited the most ketamine-like effect with consistent LORR and depressed PWS, whereas R5 exhibited less consistent LORR yet more profound PWS blunting (Supplemental Digital Content 3, http://links.lww.com/AA/B96, Fig. 1). Toxicity Norketamine ester R1 was administered to 7 rats at doses of 9.5, 30, 95, 30, 95, 30, and 95 mg/kg. Death was observed to occur in animals 3, 5, and 7 after administration of 95, 63, and 73 mg/kg, respectively (death occurring before administration of the full dose in the latter 2 animals). Therefore, the final score is OOOOXXX and LD50 50.2 mg/kg (95% confidence interval [CI], 30–63 mg/kg). R5 was administered to 7 rats at dose 9.5, 30, 95, 30, 95, 30, and 95 mg/kg. Death was observed in animals 3, 5, and 7 after administration of 95 mg/kg. Therefore, the final score is OOOOXXX and LD50 56.0 mg/kg (95% CI 30– 95 mg/kg). IV LD50 for ketamine in rats is previously reported at 58.9 mg/kg (Pfizer ketamine material safety datasheet.b Metabolic Stability in Plasma and Whole Blood Initial assessment of the metabolic stability of compounds R1 to R5 was performed in rabbit plasma and rabbit whole blood. Consistent with our hypothesis of degradation by hydrolysis of the distal ester moiety, fragmentation to the appropriate carboxylic acid and corresponding alcohol was proposed (Fig. 2). Plots of norketamine ester (R1–R5) and associated carboxylic acid metabolite (M1–M5) concentration in rabbit plasma and whole blood are presented in Figure 3. Each data point represents the mean of 2 separate experiments. Maximal variation in values was 11% and 21% for drug and metabolite, respectively. Percentage decrease in analog concentration from time 1 minute (assumed complete mixing) to 20 minutes in plasma was greatest for R1 (42%), followed by R4 (26%), R5 (20%), and R3 (−33%). Percentage decrease in analog concentration from time 1 minute (assumed complete mixing) to 20 minutes in whole blood was greatest for R2 (83%), followed Available at: http://www.pfizer.com/files/products/material_safety_ data/526.pdf. Accessed December 22, 2013. b ANESTHESIA & ANALGESIA Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited. by R3 (76%), R1 (70%), R4 (63%), and R5 (−1.5%). For each test agent, HPLC analysis showed the presence of only one major metabolite. On the basis of these results, we conclude that the rapid metabolism of norketamine esters R1 to R5 occurs exclusively via the proposed pathway outlined for R1 in Figure 2. Responsiveness in Rabbits and Pharmacokinetic Evaluation Hypnotic effect was then evaluated in whole rabbits with loss of righting and strength of pedal withdrawal serving Figure 2. Proposed fragmentation pathway for compound racemicmethyl 4-((1-(2-chlorophenyl)-2-oxocyclohexyl)amino)pentanoate hydrochloride (R1) to its carboxylic acid derivative (M1) and methanol. as primary outcome measures. All agents exhibited rapid induction of ketamine-like sedation characterized by lost righting reflex and blunted nociceptive responses. Hemodynamic parameters and behavioral metrics during sedation with norketamine analogs and ketamine are presented in Figure 4. All norketamine ester analogs displayed relative stability of heart rate and mean arterial pressure throughout the monitoring period. Myotonic activity was observed early in the course of drug administration with agent R3, and to a lesser extent with agents R4 and R5. Offset of sedation was most rapid in agent R3, with animals righting 3 minutes into the maintenance infusion and PWS normalization before cessation of maintenance infusion (Table 2, Fig. 4). Analog R1 exhibited the most consistent LORR and PWS reduction, yet still maintained rapid offset. Consistent with the pattern of sedation previously observed in our rat experiments, the analog R5 exhibited more profound, and prolonged, nociceptive attenuation (Supplemental Digital Content 4, http://links.lww.com/ Figure 3. Metabolic stability of norketamine esters in rabbit plasma and rabbit whole blood. Test agents are represented with closed icons (R1–R5). Carboxylic acid metabolites are represented with open icons (M1–M5). The metabolites of R3 and R5 (M3 and M5, respectively) are identical compounds; R2 was not analyzed in rabbit plasma due to technical difficulty. Figure 4. Hemodynamic parameters and behavioral effects of analog R1–R5 and ketamine infusion in rabbits. Shaded portion represents initial loading infusion. Dotted lines at 0 and 10 minutes represent initiation and cessation of maintenance infusion, respectively. Closed circles (● ) represent heart rate (beats/min); closed squares (◼) represent mean arterial pressure (mm Hg); upright triangles (▲) represent pedal withdrawal score; inverted triangles (▼) represent anesthetic score; grey bars represent fraction righting. All data mean (SD). XXX 2015 ڇVolume XXX ڇNumber XXX www.anesthesia-analgesia.org 5 Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited. Ketamine Analog Development Table 2. Norketamine Ester Doses, Pharmacokinetic Parameters, and Behavioral Effects Summary in Rabbits Dose to LORR (mg/kg) Total dose (mg/kg) CL (L/kg/min) V (L/kg) t½ (min) Time to righting (sec) Time to anesthetic score normalization (sec) Time to PWS normalization (sec) R1 26.5 (25.7–27.6) 46.4 (45.7–48.0) 0.72 (0.137) 0.65 (0.182) 0.65 (0.162) 42† (−42.5 to 58.5) 180* (120–210) 0 (−240 to 60) R2 23.3 (21.8–28.5) 42.7 (40–47.4) 0.69 (0.100) 3.39 (0.694) 3.3 (1.07) −122† (−187 to 0) 120* (0–270) −120 (−270 to 30) R3 23.2 (22.7–25.2) 44.2 (42.5–44.8) 0.35 (0.066) 1.68 (0.186) 3.3 (0.73) −450† (−479 to −330) 60* (−240 to 120) −300* (−390 to −120) R4 25.6 (23.0–26.0) 47.2 (42.8–50.5) 0.19 (0.017) 1.01 (0.104) 3.7 (0.51) 192† (94 to 280) 600* (240–600) 180 (90–240) R5 27.5 (26.5–34.1) 47.1 (46.3–54.2) 0.21 (0.026) 1.02 (0.126) 3.4 (0.68) 80† (−155 to 174) 1800 (1350–1800) 1800 † (1650–1800) Ketamine 10.3 (9.7–12.8) 28.6 (26.6–29.9) NA NA NA 1320 (960 to 1560) 1500 (1350–1800) 300 (−150 to 750) All times from cessation infusion (t=10minutes). Data = median (IQR); population PK data = mean (SD). LORR = loss of righting reflex; CL = clearance; V = volume of distribution; T½ = half-life; PWS = pedal withdrawal score; NA = ketamine pharmacokinetic analysis not undertaken. *P < 0.05. †P < 0.01, comparisons with ketamine. AA/B97, Fig. 2). In rabbits, the return to baseline PWS for R5 occurred very slowly, far outlasting the sedative effects of the drug (Fig. 4). By this measure, the analgesic effects of R5 lasted more than twice as long as ketamine, despite animals righting in approximately one-third of the time shown for the parent compound. Maximal test substance concentrations were achieved early in the course of infusion with concentrations declining rapidly after completion of loading infusion, and subsequently after cessation of maintenance infusion (Fig. 5). Ultrarapid metabolism was observed, which caused the carboxylic acid metabolite concentrations to exceed those of study agents at all time points, with maximal concentrations (5- to17-fold study agent concentration) observed at 10 minutes—the time of cessation of infusion of study agents. The PK parameters obtained from population modeling are presented in Table 2. These were subsequently linked with real and simulated PD measures and are presented graphically for R1 in Figure 6, with additional compounds outlined in Online Supplemental Digital Content 5 (http://links. lww.com/AA/B98, Fig. 3. While basic, these demonstrate reasonable agreement between measured and simulated metrics, suggesting the absence of significant hysteresis between the plasma drug concentration over time and the onset and offset of drug effect. DISCUSSION In the present study, we report experimental findings of 5 novel norketamine esters designed to exhibit ketamine-like sedation while providing extremely rapid offset of action secondary to hydrolysis to water-soluble carboxylic acid metabolites. Our synthetic design strategy of including a labile carboxylate ester moiety joined to the original compound mirrors that of previous investigators in developing esmolol, remifentanil, methoxycarbonyl-etomidate, and remimazolam, from their respective parents. Such “soft” designer drugs might have clinical appeal because of their rapid and predictable metabolism after exerting therapeutic actions, and hence the ability to readily titrate dosing to clinical effect. 6 www.anesthesia-analgesia.org The application of such a rationale to the N-methyl-daspartate antagonist, ketamine, has resulted in 5 ester analogs (R1–R5) with broadly similar PD and PK properties. All agents, when administered IV, exhibited ketamine-like hypnotic states characterized by LORR and attenuated nociceptive responses. Rapid recovery after cessation of infusions, or indeed even during slower infusion rates (as seen with R3 in particular), was apparent for all esters. While congruous across the 2 species under study, offset of sedation was faster in rats (return of righting reflex was approximately 10-fold less than that of ketamine compared with 3-fold in rabbits) for all study drugs. This is in keeping with what is known about the rate of drug metabolism in rodents.10,15 Such ultrarapid metabolism may have contributed to the wide CIs for measured sedative and nociceptive indices observed in R3-treated rats in particular. Although it is difficult to be sure about psychotomimetic drug effects in animal models, it was apparent in both species receiving norketamine esters that, once normal righting had been achieved, each animal exhibited normal exploratory and grooming behaviors, which were qualitatively very different from the prolonged passivity and stereotypical movements seen in animals recovering from ketamine sedation. Such an observation, although it cannot be quantified, suggests any psychotomimetic phenomena, such as the emergence reaction often reported by adults undergoing ketamine-based sedation, was attenuated in animals receiving R1 to R5. This was the goal of our design of rapidly cleared analogs. Clinical studies will be required to see whether these suggestive animal findings translate into reduced emergence phenomena in humans. We did not attempt to identify the site or the enzymatic system responsible for norketamine analog degradation. Nevertheless, these preliminary data in rabbits indicate an appreciable gradient of esterase activity beginning with plasma, followed by whole blood, then by in vivo metabolism. The huge and rapid increase in metabolites observed when the ketamine analogs were injected into live animals suggests that almost all significant esterase activity resides ANESTHESIA & ANALGESIA Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited. Figure 5. Arterial concentrations of norketamine esters R1–R5 and carboxylic acid metabolites M1–M5, to 40 minutes in rabbits. Dotted lines at 0 and 10 minutes represent initiation and cessation of maintenance infusion, respectively. Figure 6. Simulated plasma PK to PD models of pedal withdrawal score and anesthetic score for R1 in rabbits. PK = pharmacokinetic; PD = pharmacodynamic; PWS = pedal withdrawal score. in the tissues, with breakdown occurring predominantly as the result of tissue esterases similar to that found for remimazolam.16 The relatively low potency of the active ester, combined with rapid buildup of its (slowly excreted and to date unstudied) metabolites, might prove problematic when administered as an infusion for extended periods. Nevertheless, ketamine is relatively more potent in humans than in rodents, and obviously the human dosing regimen has still to be determined. Perhaps more intriguing is the spectrum of slightly different actions we observed among the different ketamine analogs investigated, despite small differences in molecular structure. At one extreme, we have R1, which has a relatively smooth hypnotic effect. At the other, we have R5, which has a relatively weak hypnotic effect and which demonstrated some degree of myotonus, but which also exerted a potent and long-acting analgesic action extending after the plasma drug levels were almost undetectable. Such findings were reproducible in both animal models under investigation, and have also been reported in our previous work.12 The origins of the observed differences in behavioral effects (and those of R5 in particular) are not immediately apparent. The mechanism of action for ketamine-mediated XXX 2015 ڇVolume XXX ڇNumber XXX analgesia remains to be fully elucidated. Antinociceptive activity nevertheless likely originates from synergy between monoamine descending inhibitory system activation,17 NR2B N-methyl-d-aspartate antagonism,18 and direct effects on opioid receptors.19 On the basis of the present work, we do not believe this to be an effect of the major metabolite (M3), because this is the same metabolite produced by R3, which did not exhibit an excessive prolonged analgesic effect. Furth ermore, the levels of isopropyl alcohol, the other significant breakdown product of R5, are nowhere near those that might produce any systemic analgesia. While mechanistic uncertainty as to the cause of these observed discrepancies remains, their existence raises the interesting possibility that we might be able to dissociate analgesia from hypnosis, and perhaps even from psychotomimetic effects, by further exploration of this group of ketamine-like drugs. These studies are subject to a number of limitations. The use of the same animals for sequential PK evaluation of ketamine analogs, while controlling for interanimal variability in responses, could have introduced bias due to the effects of study drugs on agent metabolism. Ketamine is a known cytochrome P-450 inducer,20 and its administration may have enhanced hepatic elimination of analogs administered later. Similarly, while at present unstudied, all analogs may exert similar effects on hepatic enzymes. The serial use of animals for assessment of noxious stimulus may furthermore have introduced bias from potential adaption of acute pain mechanisms to repeat testing. We have not sought to quantify the magnitude of any such phenomenon in the present work. The designated sampling frequency during PK evaluation furthermore negates more comprehensive analysis that might have been achieved with greater initial sampling rates. This is best evidenced in R1 with a calculated half life less than the minimal sampling interval. Sampling intervals were, however, adopted in line with tolerable limits of blood loss for rabbits. Given the rapidity of drug degradation, future evaluation in larger animal models will require far more frequent drug assays to more accurately model early drug degradation. www.anesthesia-analgesia.org 7 Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited. Ketamine Analog Development We did not undertake PK evaluation of the parent compound ketamine using the method described. Prior investigators investigating ketamine pharmacokinetics in identical rabbits have reported a plasma half-life of 0.74 ± 0.13 hours21 consistent with the behavioral metrics reported in this work. Differences in experimental design and the use of multicompartmental modeling techniques, however, render comparison of additional PK metrics between these studies impossible. We have not performed in-house LD50 estimation for ketamine. Our reported values for R1 and R5 are nevertheless in line with those for ketamine in similar rodent models. From these studies, it is apparent that R1 to R5 exhibit many characteristics favorable to IV administered hypnotics. Blood clearance in vivo is rapid, with commensurate reversal of behavioral effects occurring soon after cessation of infusion. Possible advantages over commonly used GABAergictype hypnotic drugs might include augmented procedural analgesia, lesser incidence of respiratory depression, and reduced potential for airway obstruction.22 Demonstration of hemodynamic stability (in line with the known sympathomimetic effects of the parent drug ketamine) provides additional advantages over short-acting hypnotics now used. The potential for clinical use may be offset by the seemingly narrower therapeutic indices of these analogs compared with those of ketamine. Our observed in vivo potencies (approximately 1.5- to 2-fold less than ketamine for LORR and PWS end points in rats) when combined with similar LD50 metrics suggest a therapeutic index less than that of the parent. However, the more relevant comparison may be with the therapeutic index of the IV opioids and hypnotics that these novel drugs may replace in clinical use. CONCLUSIONS Incorporation of rapidly degraded ester moieties into the parent compound resulted in retention of ketamine-like hypnotic properties, yet rapid offset due to degradation to carboxylic acid metabolites, in the 5 norketamine esters studied. Analgesic activity persisted well beyond that of any sedative action for one analog (R5). E DISCLOSURES Name: Martyn Harvey, MD, FACEM. Contribution: This author helped design the study, conduct the study, analyze the data, and write the manuscript. Attestation: Martyn Harvey has seen the original study data, reviewed the analysis of the data, approved the final manuscript, and is the author responsible for archiving the study files. Conflicts of Interest: Martyn Harvey is a co-inventor on a patent application for test compounds. He, his department, or his institution could receive royalties relating to the development of test compounds or their analogs. Name: Jamie Sleigh, MD. Contribution: This author helped design the study, conduct the study, analyze the data, and write the manuscript. Attestation: Jamie Sleigh has seen the original study data, reviewed the analysis of the data, and approved the final manuscript. Conflicts of Interest: Jamie Sleighis a co-inventor on a patent application for test compounds. The author or the author’s department or institution could receive royalties relating to the development of test compounds or their analogs. 8 www.anesthesia-analgesia.org Name: Logan Voss, PhD. Contribution: This author helped design the study, conduct the study, analyze the data, and write the manuscript. Attestation: Logan Voss has seen the original study data, reviewed the analysis of the data, and approved the final manuscript. Conflicts of Interest: Logan Voss is a co-inventor on a patent application for test compounds. The author, the author’s department or institution could receive royalties relating to the development of test compounds or their analogs. Name: Jiney Jose, PhD. Contribution: This author helped design the study, analyze the data, and write the manuscript. Attestation: Jiney Jose has seen the original study data and approved the final manuscript. Conflicts of Interest: Jiney Joseis a co-inventor on a patent application for test compounds. The author, or the author’s department or institution could receive royalties relating to the development of test compounds or their analogs. Name: Swarna Gamage, PhD. Contribution: This author helped design the study, conduct the study, and write the manuscript. Attestation: Swarna Gamage has seen the original study data, reviewed the analysis of the data, and approved the final manuscript. Conflicts of Interest: Swarna Gamage is a co-inventor on a patent application for test compounds. The author, or the author’s department or institution could receive royalties relating to the development of test compounds or their analogs. Name: Frederik Pruijn, PhD. Contribution: This author helped design the study, conduct the study, analyze the data, and write the manuscript. Attestation: Frederik Pruijn has seen the original study data, reviewed the analysis of the data, and approved the final manuscript. Conflicts of Interest: The author declares no conflicts of interest. Name: Sarath Liyanage, PhD. Contribution: This author helped analyze the data and write the manuscript. Attestation: Sarath Liyanage has seen the original study data, reviewed the analysis of the data, and approved the final manuscript. Conflicts of Interest: The author declares no conflicts of interest. Name: William Denny, PhD. Contribution: This author helped design the study, conduct the study, analyze the data, and write the manuscript. Attestation: William Denny has seen the original study data, reviewed the analysis of the data, and approved the final manuscript. Conflicts of Interest: William Denny isa co-inventor on a patent application for test compounds. The author, the author’s department or institution could receive royalties relating to the development of test compounds or their analogs. This manuscript was handled by: Steven L. Shafer, MD. REFERENCES 1. Parashchanka A, Schelfout S, Coppens M. Role of novel drugs in sedation outside the operating room: dexmedetomidine, ketamine and remifentanil. Curr Opin Anaesthesiol 2014;27:442–7 2. Niesters M, Dahan A. Pharmacokinetic and pharmacodynamic considerations for NMDA receptor antagonists in the treatment of chronic neuropathic pain. Expert Opin Drug Metab Toxicol 2012;8:1409–17 3. Sigtermans M, Dahan A, Mooren R, Bauer M, Kest B, Sarton E, Olofsen E. S(+)-ketamine effect on experimental pain and ANESTHESIA & ANALGESIA Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited. 4. 5. 6. 7. 8. 9. 10. 11. 12. cardiac output: a population pharmacokinetic-pharmacodynamic modeling study in healthy volunteers. Anesthesiology 2009;111:892–903 Bowdle TA, Radant AD, Cowley DS, Kharasch ED, Strassman RJ, Roy-Byrne PP. Psychedelic effects of ketamine in healthy volunteers: relationship to steady-state plasma concentrations. Anesthesiology 1998;88:82–8 Yanagihara Y, Ohtani M, Kariya S, Uchino K, Hiraishi T, Ashizawa N, Aoyama T, Yamamura Y, Yamada Y, Iga T. Plasma concentration profiles of ketamine and norketamine after administration of various ketamine preparations to healthy Japanese volunteers. Biopharm Drug Dispos 2003;24:37–43 Geisslinger G, Hering W, Kamp HD, Vollmers KO. Pharmacokinetics of ketamine enantiomers. Br J Anaesth 1995;75:506–7 Feldman PL, James MK, Brackeen MF, Bilotta JM, Schuster SV, Lahey AP, Lutz MW, Johnson MR, Leighton HJ. Design, synthesis, and pharmacological evaluation of ultrashort- to longacting opioid analgetics. J Med Chem 1991;34:2202–8 Kilpatrick GJ, McIntyre MS, Cox RF, Stafford JA, Pacofsky GJ, Lovell GG, Wiard RP, Feldman PL, Collins H, Waszczak BL, Tilbrook GS. CNS 7056: a novel ultra-short-acting Benzodiazepine. Anesthesiology 2007;107:60–6 Antonik L, Goldwater R, Kilpatrick G, Tilbrook G, Borkett K. A placebo and midazolam controlled phase 1 single ascending dose study evaluating the safety, pharmacokinetics and pharmacodynamics of remimazolam (CNS 7056): Part 1. Safety, efficacy, and basic pharmacology. Anesth Analg 2012;115:274–83 Cotten JF, Husain SS, Forman SA, Miller KW, Kelly EW, Nguyen HH, Raines DE. Methoxycarbonyl-etomidate: a novel rapidly metabolized and ultra-short-acting etomidate analogue that does not produce prolonged adrenocortical suppression. Anesthesiology 2009;111:240–9 Pejo E, Cotten JF, Kelly EW, Le Ge R, Cuny GD, Laha JK, Liu J, Lin XJ, Raines DE. In vivo and in vitro pharmacological studies of methoxycarbonyl-carboetomidate. Anesth Analg 2012;115:297–304 Jose J, Gamage SA, Harvey MG, Voss LJ, Sleigh JW, Denny WA. Structure-activity relationships for ketamine esters as shortacting anaesthetics. Bioorg Med Chem 2013;21:5098–106 XXX 2015 ڇVolume XXX ڇNumber XXX 13. Hong SC, Davisson JN. Stereochemical studies of demethylated ketamine enantiomers. J Pharm Sci 1982;71:912–4 14. Silva A, Campos S, Monteiro J, Venâncio C, Costa B, Guedes de Pinho P, Antunes L. Performance of anesthetic depth indexes in rabbits under propofol anesthesia: prediction probabilities and concentration-effect relations. Anesthesiology 2011;115:303–14 15. Haidar SH, Liang Z, Selinger K, Hamlett L, Eddington ND. Determination of remifentanil, an ultra-short-acting opioid anesthetic, in rat blood by high performance liquid chromatography with ultraviolet detection. J Pharm Biomed Anal 1996;14:1727–32 16. Upton RN, Somogyi AA, Martinez AM, Colvill J, Grant C. Pharmacokinetics and pharmacodynamics of the short-acting sedative CNS 7056 in sheep. Br J Anaesth 2010;105:798–809 17. Kawamata T, Omote K, Sonoda H, Kawamata M, Namiki A. Analgesic mechanisms of ketamine in the presence and absence of peripheral inflammation. Anesthesiology 2000;93:520–8 18. Petrenko AB, Yamakura T, Baba H, Shimoji K. The role of N-methyl-D-aspartate (NMDA) receptors in pain: a review. Anesth Analg 2003;97:1108–16 19. Sarton E, Teppema LJ, Olievier C, Nieuwenhuijs D, Matthes HW, Kieffer BL, Dahan A. The involvement of the mu-opioid receptor in ketamine-induced respiratory depression and antinociception. Anesth Analg 2001;93:1495–500 20. Chan WH, Su HC, Hung MH, Sun WZ, Fan SZ, Hsiao PN, Ueng TH. Induction of hepatic glutathione S-transferase and UDP-glucuronosyltransferase activities by ketamine in rats. Acta Anaesthesiol Taiwan 2008;46:2–7 21. Pedraz JL, Lanao JM, Dominguez-Gil A. Kinetics of ketamine and its metabolites in rabbits with normal and impaired renal function. Eur J Drug Metab Pharmacokinet 1985;10:33–9 22. Taylor DM, Bell A, Holdgate A, MacBean C, Huynh T, Thom O, Augello M, Millar R, Day R, Williams A, Ritchie P, Pasco J. Risk factors for sedation-related events during procedural sedation in the emergency department. Emerg Med Australas 2011;23:466–73 23. Buitrago S, Martin TE, Tetens-Woodring J, Belicha-Villanueva A, Wilding GE. Safety and efficacy of various combinations of injectable anesthetics in BALB/c mice. J Am Assoc Lab Anim Sci 2008;47:11–7 www.anesthesia-analgesia.org 9 Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.