Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
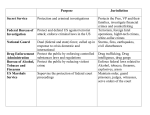
Welcome to NHSO Thailand’s UHC development National Health Security Office 23 June 2014 Thailand: country profiles • Population - 64 million • GNI 2012 US$5,090 per capita • UHC achieved in 2001 under 3 scheme • • civil servants, social security and UCS Health status Life expectancy at birth 74 years IMR 20/1000 LB, MMR 30/100,000 LB Physicians per capita 5/10,000 • Total Health Expenditure (NHA 2011) 4.1% GDP 12.4% out of pocket 3 3 Before 1974 1974 1975 1978 FFS with max ceiling WCF Fee Exemption FFS reimbursement Capitation contract model LICS Capitation for OP DRG weighted global budget for IP CSMBS Type B fee exemption 1981 1990 1991 1998 Health care reform project SSS HCS Traffic Accident Protection Program (TAP) 1993 1994 MWS 1999 SIP in 6 provinces Poor people Near poor Uninsured Oct. 2000 Fund-holding autonomous hospital (1 district) Apr. 2001 UCS in pilot 6 provinces Apr. 2002 UCS implemented nationwide Year Private employee Government employee Population covered by Universal Coverage 4 Scheme (UCS) Long march towards universal health coverage in Thailand using National Health Accounts (NHA) data GNI per capita, 1970-2009 Health service delivery system in Thailand Specialized hospitals 48 Province Regional hospitals 26 Provincial hospitals 71 District District hospitals 734 Subdistrict Health centers 9,768 MOPH facilities University hospitals 11 25 Private hospitals 322 Other public hospitals 60 Community Medical Centers 365 LGUs Private clinics 17,671 Pharmacy 11,154 Adequate and appropriately manned rural health facilities Rural health centers with 3-6 nurses n CHWs cover 2,000-5,000 population Extensive production of appropriate cadres and motivated health personnel with mandatory public works and adequate support are essential. 7 Rural community hospital with 2-8 doctors cover 30-80,000 population Seamless Health Service Networks For more complex service, secondary and tertiary hospitals with specialized personnel , highly diagnostic and treatment technology are available . Referral system was set up . Medical school hospital General hospital in every province Regional hospital in every region 8 3 main schemes’ characteristics CSMBS Fringe benefit Government employees, pensioners and their dependants5 Million (8%) Nature Population Source of finance General tax (~400 US$/Cap) Management organization Benefit package Comptroller general under ministry of finance No preventive care No explicit exclusion Special bed Providers Public provider only, Private in emergency, elective surgery (2011) Free choice public hospitals Choice of provider Payment OP: Fee-for-service IP: DRGs (2007) SSS Mandatory Formal-sector private employees, 10 Million (16%) UCS Citizen entitlement The rest of population who are not covered by SSS and CSMBS 47 Million (75%) General tax (84 US$/Cap) Tripartite rate 1.5% of salary (maximum salary: 500 US$) (health care 106 US$ /Cap, total 397 US$/Cap) Social security office under ministry of labor Small number of limited condition eg. Non medical plastic surgery National Health Security Office (NHSO) Small number of limited condition Prevention & promotion for all Public and private hospital more than 100 beds (50% private) Contracted hospital and its network Capitation OP and IP (DRG for IP DRG RW> 2) Public and private contracting unit for primary care(CUP), mainly District hospitals Primary care contractor services, plus referral OP: Capitation IP: DRGs with global budget CSMBS = Civil Servant Medical Benefit scheme, SSS = Social Security Scheme, UCS= Universal Coverage Scheme 9 Achieving efficiency and equity: role of strategic purchaser Provider payment: efficiency and cost containment • Budget • Hard budget: annual expenditure exactly equal to budget • Provider payment: Closed-end • Send strong signal – Use generic medicines, appropriate dispensing of medical technologies, – Effective prevention of supplier-induced demand – LOS stays at 4 in last 7-8 years • Risk of under-service provision, counteracted by – Complaint management through 1330 call centre, – Quality assurance, accreditation, medical audit – Setting separated payments for high cost previously underprovided services. Benefit package designs • Benefit package – Initial package: historical precedence, no application of cost effectiveness – Later inclusion guided by evidence • Benefit Package Sub-committee, NHSO – Key platform for decision on what new medical intervention is included into the package – National capacity (HITAP and IHPP) to generate evidence on • Cost effectiveness, incremental cost effectiveness ratio – ICER: not more than one GNI per capita for a QALY gain • • • • 12 Catastrophic prevention Medium to long term budget impact assessment Ethical concerns Supply side capacity to scale up new interventions Increase fiscal space & deepen financial risk protection • NHSO [single purchaser from multiple sellers] – Bargaining power over price, quantity and quality of products and services, e.g. • Central purchasing of assured quality products or constraint fee » Hemo-dialysis, down from US$ 67 to US$ 50 per session, approx 1 million sessions per annum, saving US$ 170 million per annum » Cataract soft lens, down from US$130 to US$90 with assured quality, saving US$ 40 million per annum » Erythropoietin, down from US$ 21 to US$ 8, saving US$ 12 million per annum » Drug coated Stent for coronary artery, down from US$2,700 to US$ 600, saving US$ 21 million per annum Service management: PHC orientation • District health system is a typical contractor provider network • Gate keeping role for OP and IP • Patient bypassing contractor provider network without referral are liable for full payment • Rationale use of service by level: lower unit cost • Better access: lower transport cost shouldered by patients • Better outcome: continuity of NCD control, DM, HT • Referral backups • Provincial hospitals with specialists • Regional excellent centres strengthened for sub-specialty care – e.g. heart, cancer, trauma, premature newborns 14 Expanding benefit package 2013 (B.E.2556) - Expand target group for seasoning influenza vaccines - stem cell transplantation in Leukemia and lymphoma with indication - Strategic plan for long-term care in frail elderly in Home care and community care 2012 (B.E.2555) - Liver transplantation in patient age <18 years - Heart transplantation 2009 (B.E.2552) - High cost drug in J2-National drug lists - Seasoning Influenza drug list 2007 (B.E.2550) - Thai traditional medicine services 2010 (B.E.2553) - Orphan drug, Thai traditional medicines - Psychosis admission without limitation 2008 (B.E.2551) - Renal replacement therapy (CAPD, HD, KT) - Methadone drug as a replacement drug in drug addicts 2005 (B.E. 2548) Benefit package for HIV/AIDS include ARV, Laboratory, counseling, Voluntary Counseling and Testing (VCT), condoms. 2002 (B.E. 2545) Universal health coverage for Thai citizen including health promotion, disease prevention, diagnosis, treatment, dental care, drug listed in national drug list, rehabilitation 15 UCS institutional arrangements Fund and system manager provider Head Quarter & Branch Address of NHSO NHSO Bureau of Audit Office of the secretariat Cluster of Strategy and evaluation Bureua of Strategic management Cluster of Fund administration Bureau of Registration administration Bureau of Planning and evaluation Bureau of Quality and health outcome monitoring Bureau of Executive information administration Bureau of International universal health coverage Bureau of Fund allocation and reimbursement Bureau of Finance and accounting for universal health care fund Bureau of Medical audit Cluster of Universal health care services delivery management Cluster of Office administration Bureau of primary health care promotion Bureau of General administration Bureau of Medicines, medical supplies and vaccines management Bureau of Legal affairs Bureau of secondary, tertiary and specifics cares HIV/AIDS and tuberculosis Program Chronic diseases and special diseases Program Renal diseases Program Bureau of Finance and accounting for administrative fund Bureau of Health insurance information technology management Bureau of Human resources and change management Bureau of Quality and good governanace development Cluster of Branch office mission and participation Bureau of Public and private participation promotion Bureau of Customer services and right protection Bureau of Regional support and coordination NHSO Region 1-13 Administration for UC budgeting Submit a request for annual budget 3 Main scheme Financial sub-board recommendation 13 Branch offices Recommendation Central headquarter Preliminary approved annual budget NHSO Timetable for budget subsidies plan Bureau of the budget Submit annual government budget plan Approved annual budget MOPH Submit the approved annual budget request National health security board Preliminary approved annual budget suggestion MOF Apply annual budget request 1 The Cabinet 2 The Parliament 19 Timetable for UC budgeting , FY2013 Submit Nov. a request for annual budget 2011 Financial sub-board recommendation 13 Branch offices NHSO Sep. 2012 Recommendation Central headquarter Timetable for budget subsidies plan Feb. 2012 Bureau of the budget Preliminary approved annual budget National health security board Preliminary approved Apr. annual budget Apr. 2012 suggestion Submit Apr.annual government 2012 budget plan Approved annual budget Submit the approved Feb. annual budget 2012 request 2012 Apply annual budget Mar. 2012 request 1 The Cabinet 2 May 2012 The Parliament 20 Outcomes of UC Scheme UHC cube: what has been achieved in Thai UHC? • X axis: – 99% pop overage by 3 schemes [UCS 75%, SHI 20%, CSMBS 5%] • Y axis: – Free at point of services, very minimum OOP, – Low incidence of catastrophic health expenditure and health impoverishment • Z axis: – Extensive and comprehensive benefit package, very small exclusion list, – Most high cost interventions were covered: dialysis, chemotherapy, major surgery, medicines (Essential drug list) 23 Outcome: increased government health spending Thailand THE 1994-2010 2010 2009 2008 2007 2006 2005 2004 0.0% 2003 0 2002 1.0% 2001 100,000 2000 2.0% 1999 200,000 1998 3.0% 1997 300,000 1996 4.0% 1995 400,000 Year Government spending Source: NHA1994-2010 non-government spending THE, %GDP % GDP 5.0% UHC achieved 1994 Mil Baht 500,000 Outcome: Protection against health impoverishment UHC achieved Outcome: health impoverishment sub national 1996 to 2008 Per 100 households 0 – 0.5 0.6 – 1.0 1.1 – 2.0 2.1 – 3.0 Per 100 households Per 100 households Per 100 households 0 – 0.5 0 – 0.5 0 – 0.5 0.6 – 1.0 0.6 – 1.0 0.6 – 1.0 1.1 – 2.0 1.1 – 2.0 1.1 – 2.0 2.1 – 3.0 2.1 – 3.0 2.1 – 3.0 3.1+ 3.1+ 3.1+ 3.1+ 1996 2004 1998 2000 2002 Per 100 households Per 100 households Per 100 households Per 100 households 0 – 0.5 0 – 0.5 0 – 0.5 0 – 0.5 0.6 – 1.0 0.6 – 1.0 0.6 – 1.0 0.6 – 1.0 1.1 – 2.0 1.1 – 2.0 1.1 – 2.0 1.1 – 2.0 2.1 – 3.0 2.1 – 3.0 2.1 – 3.0 2.1 – 3.0 3.1+ 3.1+ 3.1+ 3.1+ 2006 2007 2008 Increased utilization, low unmet needs Prevalence of unmet need OP IP National average 1.44% 0.4% Civil Servant Medical Benefit Scheme (CSMBS) 0.8% 0.26% Social Security Scheme (SSS) 0.98% 0.2% Universal Health Coverage Scheme (UCS) 1.61% 0.45% Source: NSO 2009 Panel SES, application of OECD unmet need definitions 27 Changes in utilization: primary secondary and tertiary 1977-2010 1977 1987 2000 2010 46% (5.5) 24% (2.9) 29% (3.5) 27% (11.0) 35% (14.6) 38% (15.7) 18.2% (20.4) 35.7% (40.2) 46.1% (51.8) 12.6% (18.1) 33.4% (33.4) 54.0% (78.0) Regional H./General H. Community H. Rural Health Centres Regional H./General H. Community H. Rural Health Centres Regional H./General H. Community H. Rural Health Centres Regional H./General H. Community H. Rural Health Centres Challenges for further reforms • Harmonization of the three main schemes is challenging as individual fund has its’ own legal framework and governing board • Burden Of Disease challenges – Increased diseases burden from chronic NCD – Little success in controlling traffic injuries • Health systems capacity to cope with – Increased workload and very strained health workforces – Decentralization context –threats and opportunities – Public private dialogues, better trust and collaboration • Medical tourism and internal brain drains • Long term financial sustainability • Aging society 29 Thank you for your attention