Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
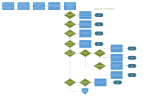
Running head: QUALITY IMPROVEMENT PROCESS: DECREASING THE NUMBER 1 Quality Improvement Process: Decreasing the Number of Left Without Being Seen Patients With a Physician at Triage Sarah DeLaat Ferris State University QUALITY IMPROVEMENT PROCESS: DECREASING THE NUMBER Abstract Emergency Department (ED) overcrowding is a serious public health issue in the United States. ED overcrowding has been associated with decreased patient satisfaction, prolonged waiting room times, and increased left without being seen (LWBS) rates. Correcting this problem is critical. Placing a physician at triage to start diagnostic workups and treatments for patients in the waiting room is a potential solution. 2 QUALITY IMPROVEMENT PROCESS: DECREASING THE NUMBER 3 Quality Improvement Process: Decreasing the Number of Left Without Being Seen Patients With a Physician at Triage Overview Throughput in the emergency department is very challenging. Overcrowding in the ED is becoming more and more common due to the lack of health care options for most people in the United States because of no insurance. Therefore, they get their primary care through the ED. This is a problem that will not be solved in the near future. However, the process in which we see patients through the ED can be modified to make it faster and more efficient. Placing a physician at triage to start diagnostic workups on patients in the waiting room is a potential solution to this not only national problem, but a problem that is currently happening at Butterworth Emergency Department. Problem “Numerous reports have questioned the ability of the United States emergency departments to handle the increasing demand for emergency services. ED overcrowding is widespread in US cities and has reportedly reached crisis proportions”, ( Trzeciak and Rivers, 2003). This statement alone led to further research in the Butterworth ED. According to Kevin Throop, nursing supervisor for Butterworth ED, “We are the 7th busiest ED in the nation. We are equipped to see approximately 80,000 patients per year and we saw over 107,000 patients through the department last year.” With those numbers alone, one has to question the effect of overcrowding in the ED. “Of those 107,000 patients, roughly 14% were admitted to the hospital and 52% of those admitted patients were held in the ED waiting for admission beds”, states Throop. QUALITY IMPROVEMENT PROCESS: DECREASING THE NUMBER 4 Butterworth’s average left without being seen rate for 2011 was 2.4%. The main cause for people leaving the ED was increased waiting room times. The waiting room gets backed up due to the fact that there are patients being held in the ED for admission because the hospital is full. In 2011 alone, Butterworth ED admitted 13.6% of their 107,000 patients seen (Spectrum Health Butterworth ED statistics, 2012). It’s a never ending cascading effect that continues to put ED patients at risk while having to wait to be seen by a physician. Interdisciplinary Team Trialing a physician at triage has been discussed by Butterworth ED managers, physicians, and charge nurses. A few of the physicians have been doing some extensive research on the topic in order to determine whether or not this will actually benefit our department. These staff members are key members in getting this trial started. Joshua Kooistra D.O. at Butterworth ED has been researching other hospitals comparable to our department size and their methods for placing a physician at triage. Kooistra states, “With the increase number of patients coming through the ED, protocol orders at triage are not going to be enough. The nurses do a fantastic job in triaging patients, but now is the time when we need a physician resource at triage to assist in determining a plan of care for the patient the minute they walk through the door.” Data Collection and Outcomes With the current number of LWBS patients at an average of 2.4% at Butterworth ED, the most logical data to collect is the number of patients that leave without being seen after placing a physician at triage and compare those numbers to the already established data. The collection method will be done through the already established computer program utilized to track patients QUALITY IMPROVEMENT PROCESS: DECREASING THE NUMBER 5 through the ED. The data will then be placed into a histogram form in order to have a visual as well as statistical comparison for leadership to determine whether or not a physician at triage is beneficial. If it is noted that the number of LWBS patients in the ED has decreased with the physician at triage method, the goal would be to keep this number at 1% or below. Implementation Strategies The plan is to continue the triage process much as it has in the past. One lead triage nurse and two nurses performing assessments in the two rooms behind the lead triage nurse. The physician will be stationed at the second computer at the lead triage desk. This will allow the physician to stay in the immediate triage area, listen to and view the patients presenting to the lead desk, as well as listen to a more in depth triage from the nurses interviewing patients in the triage rooms. The physician will place orders from the triage area which will be carried out by a consult nurse. There will be a fourth triage nurse acting as the consult nurse; drawing labs, medicating patients, and doing simple procedures such as discharging some patients from the waiting room. This nurse should never be pulled away from the triage area if we are busy. In order for this process to succeed, there needs to be a dedicated nurse to carry out the physician orders. There will be some ground rules on medications that can be given at triage. No patient will be allowed to have an IV and be placed back in the waiting room. No intramuscular or intravenous narcotics shall be given to patients. However, patients may take oral narcotics if ordered by the physician and placed back in the waiting room. The physician and consult nurse will be responsible for keeping tabs on lab and radiology results of patients still waiting in the waiting room. If the physician deems fit to discharge the patient from the waiting room, the consult nurse will bring the patient back to the consult room QUALITY IMPROVEMENT PROCESS: DECREASING THE NUMBER 6 where the physician can speak to them, and appropriately discharge them from there. No patients will actually be placed in the consult room as a permanent holding room. Conclusion Optimal care for arriving ED patients traditionally entails being treated rapidly by a physician in a private ED bed to which they are assigned throughout their stay. Unfortunately because many EDs have such high census, more innovative processes must be explored to provide the best care possible for those patients who are unable to get a bed immediately in the department. Effective strategies like placing a physician at triage optimizes patient outcomes as well as contributing to maintaining high quality care during high census times. QUALITY IMPROVEMENT PROCESS: DECREASING THE NUMBER References Kooistra, J. interviewed by Sarah DeLaat, 2012 Throop, K. interviewed by Sarah DeLaat, 2012 Trzeciak, S. and Rivers, E.P. Emergency department overcrowding in the United States: an emerging threat to patient safety and public health. Emergency Medicine Journal 2003. 7