Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
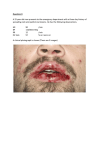
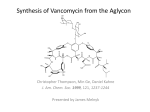
Vancomycin Vancomycin hydrochloride is used increasingly to treat methicillin -resistant S. aureus, which has become a major concern in different parts of the world. Because of the emergence of vancomycin -resistant enterococci, vancomycin must be used judiciously. As a rule of thumb, it should be used only when culture and sensitivity test results confirm the need for it. A. Mechanism of action Vancomycin inhibits synthesis of bacterial cell wall phospholipids as well as peptidoglycan polymerization weakening the cell wall and damaging the underlying cell membrane. B. Antibacterial spectrum Vancomycin is effective against gram-positive organisms. It has been lifesaving in the treatment of MRSA and methicillin-resistant Staphylo coccus epidermidis (MRSE) infections as well as enterococcal infections. With the emergence of resistant strains, it is important to curtail the increase in vancomycin-resistant bacteria (for example, Enterococcus faecium and Enterococcus faecalis) by restricting the use of vancomycin to the treatment of serious infections caused byβlactam resistant, gram-positive microorganisms or for patients with gram-positive infections who have a serious allergy to the β-lactams. Oral vancomycin is limited to treatment for potentially life-threatening, antibiotic-associated colitis due to C. difficile. Intravenous vancomycin is used in individuals with prosthetic heart valves and in patients undergoing implantation with prosthetic devices, especially in those hospitals where there is a problem with MRSA or MRSE. Vancomycin acts synergistically with the aminoglycosides, and this combination can be used in the treatment of enterococcal endocarditis. Daptomycin, a cyclic lipopeptide antibiotic, and two protein synthesis inhibitors— quinopristin/ dalfopristin and linezolid—are currently available for the treatment of vancomycinresistant organisms. Pharmacokinetics Because vancomycin is absorbed poorly from the GI tract, it must be given I.V. to treat systemic infections. However, an oral form of vancomycin is used to treat pseudomembranous colitis. Vancomycin diffuses well into pleural (around the lungs), pericardial (around the heart), synovial (joint), and ascitic (in the peritoneal cavity) fluids. Remember that I.V. vancomycin can’t be used in place of oral vancomycin and vice versa. The two forms aren’t interchangeable. Slow IV infusion (60–90 minutes) of vancomycin is employed for treatment of systemic infections or for prophylaxis. Because vancomycin is not absorbed after oral administration, this route is employed only for the treatment of antibiotic-induced colitis due to C. diffi cile. Infl ammation allows the intravenous formulation to penetrate into the meninges. However, it is often necessary to combine vancomycin with other antibiotics, such as ceftriaxone for synergistic effects when treating meningitis. Metabolism of the drug is minimal, and 90 to 100 percent is excreted by glomerular filtration. Metabolism and excretion The metabolism of vancomycin is unknown. About 85% of the dose is excreted unchanged in urine within 24 hours. A small amount may be eliminated through the liver and biliary tract. Pharmacodynamics Vancomycin inhibits bacterial cell -wall synthesis, damaging the bacterial plasma membrane. When the bacterial cell wall is damaged, the body’s natural defenses can attack the organism. Pharmacotherapeutics Vancomycin is active against gram -positive organisms, such as S. aureus, S. epidermidis, S. pyogenes, Enterococcus, and S. pneumoniae. I.V. vancomycin is the therapy of choice for the patient with a serious resistant staphylococcal infection who’s hypersensitive to penicillins. Oral vancomycin is used for the patient with antibiotic-associated Clostridium difficile colitis who can’t take or has responded poorly to metronidazole. Vancomycin, when used with an aminoglycoside, is also the treatment of choice for E. faecalis endocarditis in the patient who’s allergic to penicillin. Drug interactions Vancomycin may increase the risk of toxicity when administered with other drugs toxic to the kidneys and organs of hearing, such as aminoglycosides, amphotericin B, bacitracin, cisplatin, colistin, and polymyxin B. Adverse reactions to vancomycin Adverse reactions to vancomycin, although rare, include: - hypersensitivity and anaphylactic reactions - drug fever - eosinophilia (an increased number of eosinophils, a type of white blood cell [WBC]) neutropenia (a decreased number of neutrophils, another type of WBC) - hearing loss (transient or permanent), especially with excessive doses (as when it’s given with other ototoxic drugs). - Severe hypotension may occur with rapid I.V. administration of vancomycin and may be accompanied by a red rash with flat and raised lesions on the face, neck, chest, and arms (red man’s syndrome).