Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
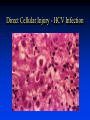
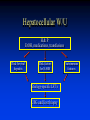
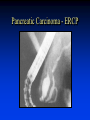
Evaluation of Liver Injury Mark J. Czaja Liver Research Center Albert Einstein College of Medicine Bronx, N.Y. Liver Function Tests • • • • • • Alanine aminotransferase (ALT) Aspartate aminotransferase (AST) Lactate dehydrogenase (LDH) Alkaline phosphatase Bilirubin Albumin Mechanisms of Liver Dysfunction • Direct cellular injury • Blockage in bile flow • Impaired blood flow Direct Cellular Injury - HCV Infection Blockage in Bile Flow - Biliary Atresia Impaired Blood Flow - CHF Consequences of Liver Injury liver cell injury liver cell death proliferation matrix deposition sufficient inadequate recovery liver failure altered architecture cirrhosis Types of Liver Tests • True tests of liver function • Biochemical markers of liver injury • Biochemical markers of specific liver diseases Testable Biochemical Liver Function • Ability to transport organic anions • Capacity to metabolize certain substances • Capability to synthesize various proteins Steps in Organic Anion Transport • Delivery and uptake • Metabolic alteration • Secretion and excretion Bilirubin • Tetrapyrole • Toxic in neonates - kernicterus • Derived from: Senescent RBC (70-80%) Hemoproteins (20-30%) Ineffective erythropoiesis Bilirubin Formation heme heme oxygenasebiliverdin biliverdin reductase bilirubin Transport: hydrophobic due to internal H-bonding circulates bound to albumin Bilirubin Metabolism Plasma Bile Hepatocyte Alb UCB BMG BDG UCB ligandin glucuronyl BMG BMG transferase BDG BDG Bilirubin Elimination Intestine • BMG (20%) + BDG (80%) +UCB (trace) • Deconjugated to urobilinogen • Excreted or reabsorbed (20%) Urine • BMG and BDG • No UCB Measurement of Serum Bilirubin • • • • Normal concentration < 1 mg/dl Conjugated < 5% Jaundice if > 3 mg/dl Detected by diazo reaction - cleaved to colored azo-dipyrole Conjugated reacts rapidly (direct) Unconjugated reacts slowly (indirect) Differential Diagnosis I • Prehepatic • Intrahepatic Congenital Acquired • Posthepatic Differential Diagnosis II • Unconjugated hyperbilirubinemia Increased bilirubin production (hematological) Decreased uptake (drug) Decreased conjugation (congenital) • Conjugated hyperbilirubinemia Congenital Drug Liver disease Biliary obstruction Inherited Disorders Causing Unconjugated Hyperbilirubinemia • Crigler-Najjar syndrome Type 1 – absent GT Type 2 – reduced GT activity • Gilbert’s syndrome – reduced GT activity due to genetic defect in TATAA element of GT promoter Inherited Disorders Causing Conjugated Hyperbilirubinemia • Dubin-Johnson syndrome – mutations in multidrug resistance associated protein 2 (MRP2) • Rotor’s syndrome – genetic defect Hepatic Metabolic Capacity • Clearance must depend on total functional mass or metabolic activity • Hepatic drug metabolism [14C]amino-pyrine breath test • Galactose elimination • Not used clinically Hepatic Synthetic Capacity • Most major plasma proteins are made in the liver • Decreased hepatocytes = decreased protein synthesis and release • Albumin and coagulation factors are clinically important Albumin • 50% of all synthesized hepatic protein • Determinant of plasma oncotic pressure • Important transport protein Serum Albumin Levels • Long half-life of 20 days • Large hepatic synthetic reserve • Decreased with persistent, large injury • Decreased in chronic liver disease • Poor prognostic sign Non-hepatic Causes of Hypoalbuminemia • Severe malnutrition • Renal or GI loss Glomerulopathy, HIV enteropathy • High catabolism Infections, burns Coagulation Factors • Half-lives of hours to days • Liver synthesizes I, II, V, VII, IX, and X • Large synthetic reserve Prothrombin Time (PT) • PT detects abnormalities in I, II, V, VII and X (extrinsic pathway) • PT is increased in liver disease • Best prognostic indicator Acute liver disease Chronic liver disease Non-hepatic Causes of Elevated PT • Congenital coagulation factor deficiencies • Consumptive coagulopathies • Vitamin K deficiency (II, VII, IX, X) To Rule Out Vitamin K Deficiency • Any patient with an elevated PT • Parental vitamin K for 3 days • Normalization of PT - vitamin K deficiency • Failure to normalize - hepatocellular disease Serum Immunoglobulins • Not produced by hepatocytes • Frequently elevated in liver disease • Secondary to inflammatory process • ? produced by antigen shunting Biochemical Markers of Liver Injury Liver Enzymes • Low levels always present in serum • Leak out from cell after injury • Very sensitive • Magnitude of abnormality does not correlate well with degree of injury Aspartate Aminotransferase (AST) • Serum glutamic-oxaloacetic transaminase (SGOT) • Transfers an a-amino group of aspartate to a-keto group of ketoglutaric acid • Present in skeletal muscle, kidney, brain Alanine Aminotransferase (ALT) • Serum glutamic-pyruvic transaminase (SGPT) • Transfers an a-amino group of alanine to a-keto group of ketoglutaric acid • Present principally in liver AST and ALT • Elevated in most liver diseases • Highest levels are in acute liver diseases • Only slight elevations in chronic liver diseases • Usually increase in parallel AST/ALT in Alcoholic Hepatitis • Transaminases rarely exceed 300 • AST:ALT >2 Factors Affecting AST/ALT • Depressed by pyridoxine (vit. B6) deficiency • Decreased by uremia and renal dialysis AST/ALT Controversies • Should lower normal limits be used in females? Females < 30 vs. males < 40 • Are the normal limits too high? Females < 20 and males < 30 Lactate Dehydrogenase (LDH) • Component of classic LFT’s • Highly non-specific Tests of Impaired Hepatic Excretion Increased In • Cholestasis • Intra-hepatic biliary tract obstruction • Extra-hepatic biliary obstruction Alkaline Phosphatase • Hydrolyzes phosphate esters at alkaline pH • Also present in bone, kidney, placenta, intestine • Mainly liver and bone in adults • Increased in children from bone growth • Placental form during pregnancy Elevated Alkaline Phosphatase • Can occur in any liver disease • Highest with cholestasis or biliary tract obstruction • Elevated in infiltrative diseases • Due to increase synthesis and secretion Alkaline Phosphatase Isoenzymes Source Heat Inactivation 5' NT GGTP Liver Moderate + + Bone Rapid - - Placenta Slow - - Intestine Slow - - 5'-Nucleotidase • Hydrolyzes 5'- adenosine monophosphate • Mainly present in liver • Increases along with alkaline phosphatase g-Glutamyl Transpeptidase (GGTP) • • • • Transfers g-glutamyl groups Widely distributed Sensitive correlate to alkaline phosphatase Non-specific (alcoholism, MI, DM, pancreatic disease, renal failure) Biochemical Markers of Specific Liver Diseases Etiology-specific Liver Tests • • • • • Viral hepatitis serologies Serum ferritin level Ceruloplasmin level Alpha1-antitrypsin level Antimitochondrial antibody titer Viral Hepatitis Serology • HAV – anti-HAV IgM and IgG • HBV – HBsAg, anti-HBsAg, and anti-HBcAg • HCV – anti-HCV, HCV RNA Serum Ferritin • Widely distributed storage protein • Levels reflect body iron stores • Elevated in primary hemochromatosis • Elevated in acute inflammation and cirrhosis Serum Ceruloplasmin • Copper-binding protein • Decreased in 95% of patients with Wilson’s disease • 20% of heterozygotes have decreased levels a1-Antitrypsin • Inhibits serum trypsin • Major component of a1-globulin • Deficiency cause of neonatal hepatitis Antimitochondrial Antibody (AMA) • Directed against mitochondrial enzyme pyruvate dehydrogenase complex • Positive in 90% of patients with primary biliary cirrhosis Interpretation of Abnormal LFT’s • Examine multiple tests • Consider non-hepatic causes • Determine the most abnormal tests Hepatocellular vs. Cholestatic Test Hepatocellular Cholestatic ALT/AST 2-3 NL-1 Alk Phos NL-1 2-3 Bilirubin NL-3 NL-3 Albumin NL-3 NL PT NL-3 NL Case 1 25 yo IVDA c/o 1 week of nausea, vomiting, and myalgias. Physical exam revealed jaundice. • ALT 2045 (15-45) • AST 2300 (15-45) • Alk Phos 273 (50-150) • Bili 3.9 (0.1-1.0) • Alb 4.2 (3.5-5.5) • PT 11.5 (10-12) Hepatocellular W/U H&P EtOH, medications, transfusions Risk for viral hepatitis Risk factors for NASH Etiology-specific LFT’s USG and liver biopsy Autoimmune features HBV Infection - HBcAg Staining Case 2 67 yo c/o several months of weight loss, and 1 week of nausea, vomiting, and myalgias. Physical exam revealed cachexia and jaundice. • ALT 75 (15-45) • AST 115 (15-45) • Alk Phos 650 (50-150) • Bili 10.2 (0.1-1.0) • Alb 4.2 (3.5-5.5) • PT 11.0 (10-12) Cholestatic W/U H&P medications, gallstones, weight loss USG normal AMA liver biopsy dilated ducts ERCP Pancreatic Carcinoma - ERCP