Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
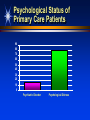
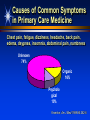
Patient as Partners Improving Health and Cost Outcomes with Self-Care and Chronic Disease Self-Management NatPaCT Conference Programme Learning from Kaiser Permanente – How can the NHS make better use of its resources and improve patient care? Tuesday 4 November 2003 – The Brewery, London David S. Sobel, MD, MPH Director, Patient Education and Health Promotion Kaiser Permanente Northern California 1950 Franklin Street., 13th Floor, Oakland, CA 94612 Phone: 510-987-3579 Fax: 510-873-5379 E-mail: [email protected] Strategy for Changing Culture and Practice Look for inefficiencies, mismatches, and capacity overlooked evidence and data “win, win, win” opportunities Strategy for Changing Culture and Practice Rethink Care 1. Patients as primary providers of acute illness 2. Self-management of chronic illness 3. Behavioral interventions to address psychosocial needs Restructure Care Telephone, group appointments, web-based care Retrain for Collaborative Care Enhance understanding, skills, and confidence of members and professional staff as partners in care Rethinking Care 1: Self-Care for Acute Illness Patient as Consumer Patient as Provider Hidden Health Care System 3 2 Professional Care 20% 1 Self-Care 80% Self-Care: Patients as Providers Over 80% of all medical symptoms are selfdiagnosed and self-treated without professional care. Patients are the true primary care providers of medical care for themselves and their families. How can health care systems educate, equip, and empower the true primary care providers… patients? Kaiser Permanente Self-Care Program Vision: “Partners in Health” A system intervention that changes the culture of care and supports members making safe, appropriate, and informed health care choices KP Healthwise Handbooks distributed to all members Provider training and reinforcement Continuing systemwide reinforcement Kaiser Permanente Healthwise Handbook Kaiser Permanente Self-Care Program Results High use of the KP Healthwise Handbook 70% in previous 6 months Improved member self-care confidence 71% more confident Increased member satisfaction 60% more positive about Kaiser Permanente More appropriate utilization & improved accessibility 50% report saving a call or visit to MD 6% medical visits and 5%telephone calls Improved provider and staff satisfaction Rethinking Care 2: Self-Management of Chronic Illness Patient as Consumer Patient as Provider Chronic Care Model Community Health System Health Care Organization Resources and Policies SelfManagement Support Informed, Activated Patient Delivery System Design Productive Interactions Decision Support Clinical Information Systems Prepared, Proactive Practice Team Improved Outcomes E. Wagner Living with Chronic Disease Managing the Illness Taking medications Changing diet and exercise Managing symptoms of pain, fatigue, insomnia, shortness of breath, etc. Interacting with the medical care system Managing Daily Activities and Roles Maintaining roles as spouse, parent, worker, etc. Managing the Emotions Managing anger, fear, depression, isolation, etc. Lorig K, Holman H, Sobel D, Laurent D, Gonzalez V, Minor M: Living a Healthy Life with Chronic Conditions, Palo Alto, CA: Bull Pub. Co., 2000 Healthier Living with Ongoing Health Conditions* Lay-led, small interactive groups (2 hours/week for 7 weeks) Mixed chronic disease and co-morbidities Content Goal setting and problem-solving Cognitive symptom management Design of exercise programs Management of fatigue, sleep, pain, anger, depression Appropriate use of medications Patient/physician communication Use of advanced directives *aka Chronic Conditions Self-Management Program, Expert Patient Programme Lorig K et al Medical Care 1999;37:5-14. http://patienteducation.stanford.edu/ Healthier Living with Ongoing Health Conditions Improves health behaviors and health status Cost effective (estimated 5:1 to 10:1 ROI) Outcomes are long-lasting and robust (2+yrs.) Replicable and dissemination can yield outcomes as good, or better. Lorig KR, Sobel DS, Effective Clin Practice 2001;4:256-262 Lorig KR, Medical Care 2001;39:1217-1223 Chronic Disease Self-Management Program LESSONS General coping skills education for heterogeneous conditions complements disease specific information Patients are the “experts” in living and coping with chronic illness Modeling more effective than “save and rescue” No significant difference in participants’ outcome with lay vs professional leaders Confidence predicts improvement in health outcomes People benefit themselves from helping other people Process is more important than content Rethinking Care 3: Behavioral Medicine Body as Machine Mind as HMO Sobel DS: The cost-effectiveness of mind-body medicine interventions. In The Biological Basis for Mind Body Interactions, Progress in Brain Research, Vol 122, EA Mayer and CB Saper (Eds.), Elsevier, 2000:393-412. Somatic Symptom Superhighway Final Common Pathway Psychiatric Disorder Emotional Distress Medical Illness Somatic Symptoms Psychological Status of Primary Care Patients 90 80 70 60 50 40 30 20 10 0 Psychiatric Disorder Psychological Distress Causes of Common Symptoms in Primary Care Medicine Chest pain, fatigue, dizziness, headache, back pain, edema, dsypnea, insomnia, abdominal pain, numbness Unknown 74% Organic 16% Psycholo gical 10% Kroenke, Am J Med 1989:86:262-6 Depressive Symptoms Depressive symptoms more debilitating in terms of physical and social functioning than: diabetes arthritis gastrointestinal disorders back problems hypertension Wells et al. JAMA 1989;262:914-930 Psychosocial Dysfunction in Medical Care Common Undiagnosed or inadequately treated Significant impact on: functional status and disability medical utilization and costs medical morbidity and mortality Health Care services mismatched to needs Need to develop integrated behavioral health education services Sobel DS: Rethinking medicine: Improving health outcomes with cost-effective psychosocial interventions. Psychosomatic Medicine 57:234-244, 1995. % Classifed as Psych Outpatient Cases on SCL-90 Mind/Body Medicine Program Evaluation Pre- and Post-Class 70% 60% Intake 62.1% Post-Program 12 NCal Facilities 61.2% 60.0% 50% 40% 30% 20% 31.7% 28.2% 21.5% 10% 0% Depression (n=124) Anxiety (n=121) Somatization (n=120) SCL-90 Sub-scale Measures Nancy Gordon - DOR (June, 2000) Utilization Change for Mind/Body Medicine Participants 6-Mo. Pre 6-Mo. Post 3000 N=609 2500 Total Visits 2000 1500 1000 500 0 ADP +34% ER - 45% Med -37% Urg -22% Psy - 41% Ngissah, Levine, & Walsh (1998 - N. Valley) Rethinking Health Improvement Interventions Attitudes Beliefs Moods Health Behavior Change Health Outcomes Confidence Counts Lorig K, Arthritis and Rheumatism. 1989;32:91-95 Targeting Core Attitudes, Beliefs, and Moods Quality of Life Behavioral Risk Reduction Problems in Living CORE Attitudes Beliefs Moods Mental Illness Psychosocial Skills Medical Conditions Ornstein R, Sobel D: Healthy Pleasures. Addison-Wesley, 1989 Restructuring Care Medical Office Visits Group Appointments and Web-based Care Medical Group Appointments (Group Visits, Cluster Visits, etc.) Scheduled or ‘drop-in’ visit for group of patients with similar or mixed health conditions Under direction of physician or other licensed health care professional Provision of individualized clinical services Medical Assessment history, physical assessment, triage, referral Medical Intervention medication prescription/adjustment, lab tests Diabetes Cooperative Care Clinic Randomized clinical trial, n=185, f/u 1yr, 2hr group monthly x 6 Outcomes lower HgbA1C ( 1.3% vs. 0.22% controls, p<0.0001) more home blood glucose monitoring reduced hospital and outpatient utilization hospitalizations 80% more frequent in control fewer physician and nonphysician visits increased self-efficacy diet, management of low BG and BG when sick increased satisfaction Sadur CN, Diabetes Care, 1999;12:2011-2017 Restructure Care: Web-Based Care at kp.org www.kaiserpermanente.org Get Health Advice Appointment/Rx Refills Physician Personal Home Page: A Personal Portal to Kaiser Permanente Online Services Retraining for Collaborative Care Traditional, Paternalistic Care Collaborative Care How Traditional Care Differs from Collaborative Care Issue Traditional Care/ Patient Education Relationships Professional are expert. Patients are passive. Needs Assessment Content Provider defines what patients need to know. Disease management Process Prescribed behavior change. Provider solves problems. External motivation. Didactic presentations. Knowledge and behavior Outcomes Collaborative Care/ Self-Management Education Shared expertise with active patients. Patient expert in their experience of disease Patient defined problems Disease, role, and emotional management Self-defined goals. Patient learns problem-solving skills. Focus on internal motivation and self-efficacy. Interactive. Health status and appropriate utilization adapted from Bodenheimer, Lorig, et al JAMA 2002;288:2469. Retraining for Collaborative Care Thriving in a Busy Practice: Clinician-Patient Communication (“Four Habits of Effective Clinicians”) Brief Negotiation Practice Essentials for Care Managers Education for Health Action Group Appointment Toolkit Retraining for Collaborative Care: Key Strategies Address member’s needs in 3 domains: 1. Disease and Health Management 2. Role Management 3. Emotional Management Use state-of-art communication/educational strategies: Transform didactic, information-based approaches into interactive, self-efficacy/confidence enhancing communication that strengthens patients’ skills in problem-solving, goal setting and action planning, self-tailoring, using available resources, forming a partnership with clinician Ask questions and elicit patient perspective and engagement in action planning and problem-solving Use nonjudgmental and positive tone Link back to member’s routine source of care and team care and peer support Patients as Partners: Changing Culture and Practice Rethink Care 1. Patients as primary providers of acute illness 2. Self-management of chronic illness 3. Behavioral interventions to address psychosocial needs Restructure Care Telephone, group appointments, web-based care Retrain for Collaborative Care Enhance understanding, skills, and confidence of members and professional staff as partners in care Appendices Four Habits of Highly Effective Clinicians 1. 2. 3. 4. Invest in the Beginning Elicit the Patient’s Perspective Demonstrate Empathy Invest in the End Frankel RM, Stein T. Getting the Most out of the Clinical Encounter: The Four Habits Model. The Permanente Journal, Fall 1999, Vol 3, No. 3 http://www.kaiserpermanente.org/medicine/permjournal/fall99pj/frhabits.html 2003 CMI Evidence-Linked Recommendations Embed Self-Mgt into Pop Mgt: Lower intensity interventions (automated phone messages, staged mailings, videos, online) for all patients Higher intensity (e.g. multi-session programs) for those with higher needs Robert Wood Johnson Foundation and Center for the Advancement of Health. Essential Elements of Self-Management Interventions, 2002. Von Korff M, Tiemens B. West J Med 2000; 172(2):133-137. Piette JD,e al. Am J Med 2000; 108(1):20-27. Serxner S, et al. Congestive Heart Failure; 1998. May/June:23-28. 2003 CMI Evidence-Linked Recommendations, cont’d. During clinical encounter, support member’s central role in health: Collaborative communication (Brief Negotiation, 4 Habits) Assess member’s self-mgt needs; provide tailored feedback and behavioral advise Collaboratively set behavioral goals and action plan. Document and share with member. Offer self-mgt resources; refer to programs F/up to adapt plan and address relapse Glasgow RE et al. Ann Behav Med 2002; 24(2):80-87. Stewart MA. CMAJ 1995; 152(9):1423-1433. Petrella RJ, Lattanzio CN. Can Fam Physician 2002; 48:72-80. Rice VH. Heart Lung 1999; 28(6):438-454. Boulware LE, et al. Am J Prev Med 2001; 21(3):221-232. 2003 CMI Evidence-Linked Recommendations, cont’d. Strengthen Adherence to Prescribed Medications: Anticipate nonadherence: “Have you ever missed or forgot to take your pills?” Identify personal barriers and problem solve. Avoid assuming causes of nonadherence Collaboratively develop a regimen pt is willing and able to follow. Praise efforts to adhere. As needed, refer for pharmacist consultation McDonald HP, et al. JAMA 2002; 288(22):2868-2879. Haynes RB , et al. JAMA 2002; 288(22):2880-2883. Yuan Y, et al. Am J Manag Care 2003; 9(1):45-56. 2003 CMI Evidence-Linked Recommendations, cont’d. Turn didactic pt education into self-mgt education Beyond knowledge to skills & confidence: Problem solving training (incl. medication adherence) Goal setting and action planning Peer modeling and support Experiential exercises (relaxation session, read peak flow meter, pick from a menu) Forming partnership with clinician Bodenheimer T et al. JAMA 2002; 288(19):2469-2475. Norris S et al. Diabetes Care 2002; 25(7):1159-1171. Gibson PGM et al. Cochrane Database Syst Rev 2002;2. Barlow J, et al.Patient Educ Couns 2002; 48(2):177-187. 2003 CMI Evidence-Linked Recommendations, cont’d. Offer multiple options to receive self-mgt education: Staged mailings based on readiness to change Telephone group sessions Group visits Internet-based programs Community and work site programs Serxner S, et al. Congestive Heart Failure 1998; May/June:23-28. Boucher, JL et al. Diabetes Spectrum 1999 12(2).121-123. Wagner EH et al. Diabetes Care 2001; 24(4):695-700. McKay HG, et al. Diabetes Care 2001; 24(8):1328-1334. Norris SL et al. J Prev Med 2002; 22(4 Suppl):39-66. Pelletier KR. Am J Health Promot 2001; 16(2):107-116.