Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
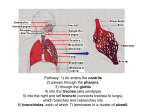
Pulmonary Ventilation Pulmonary Functions Conducting Airways • Lead inspired air to gas exchanging regions • Anatomic dead space – 150 ml – Nose – Mouth • Process by which ambient air moves into and exchanges with the air in the lungs Conducting Airways – Trachea • Add H2O vapor to inspired air • Warm air to body temperature (sometimes cooling) • Trap particulate matter and fumes to prevent them from reaching the alveolar membranes – – – – – Dust Yeast Bacteria Smoke Ozone – Right and left main bronchi – Bronchioles – Terminal bronchioles 1 Respiratory Zone • Where gas exchange occurs • 2.5 – 3 L Respiratory Zone • Provides a large surface area for gas exchange – Respiratory bronchiole • Occasional alveoli budding from walls – Alveolar ducts • Lined with alveoli The Lungs • • • • Gas exchange – O2 and CO2 Volume = 4-6 L Weight = 1 kg Vascularized with infoldings which provide a high surface area for blood aeration • Rest – RBC remains in pulmonary capillary for .5 – 1 sec only • >300 million alveoli Alveoli • Sacs ~ 0.3 mm in diameter • Alveolar tissue receives the largest blood supply of any of the body’s organs • Very thin pulmonary blood-gas barrier • Each minute – 250 mL O2 leave alveoli and enter blood - 25 X during 2 Minimum of distance and tissue between alveolar air and RBC’s Ventilation • Caused by changes in thoracic volume which results in intrapulmonary pressure changes Movement of Air • Airflow (L/min) = pressure gradient (mm Hg)/resistance • Resistance – sum of forces opposing flow of gas – 20% - tissue friction during inspiration and expiration – 80% due to friction between gas molecules and walls of airway and internal friction between gas molecules themselves • Pressure gradient > Resistance to obtain flow • Boyle’s Law – pressure of a gas in inversely related to its volume under constant temperature Diaphragm • Primary ventilatory muscle • Creates an airtight separation between abdominal and thoracic cavities with openings for esophagus, vessels, and nerves • Greatest capacity of all respiratory muscles for shortening and volume displacement Mechanics of Ventilation • Inspiration – chest cavity increases – Ribs move up and out – external intercostals lift ribs up and away from body – Floor of thorax descends - diaphragm contracts (up to 10 cm) – Volume is increased, intrapulmonary pressure decreases below ambient/atmospheric conditions – Atmospheric air rushes into lungs • 70% of lung expansion from A-P enlargement • 30% of lung expansion from diaphragmatic descent – Inspiration ends when thoracic cavity expansion ceases, causing intrapulmonary pressure to increase to ambient pressure 3 Inspiration • As air moves into the smaller branches of the lungs, the increase in surface area significantly slows airflow into alveoli Mechanics of Ventilation • Expiration – passive at rest – Natural recoil of stretched lung tissue – Relaxation of respiratory muscles – – – – Diaphragm and external intercostals relax Diaphragm recoils raising floor of thorax Ribs return to original position Decreases the volume of thorax, increasing intrapulmonary pressure – Air rushes out of lungs – Expiration ends when intrapulmonary pressure decreases to atmospheric pressure Ventilation During Exercise • Expiration – active movement results in more rapid and extensive exhalation • Internal intercostals pull ribs down and in • Abdominals contract to increase abdominal pressure forcing diaphragm up into thorax • Muscle involvement greatly increases maximal rate of ventilatory flow • During exercise, tidal volume (VT) increases more than breathing frequency (f) which provides sufficient time for gas exchange in the alveoli 4 Surface Tension • Early physiologists found that lungs inflated with saline have more compliance (easier to distend) than air-filled lungs • Surface tension relates to the resistance created at the lining of the alveoli where a liquid contacts a gas • Surface tension is the force acting across an imaginary line 1 cm long • Surface tension in the alveoli during inspiration increases resistance Surface Tension • Attractive forces between adjacent molecules of the liquid are much stronger than those between the liquid and gas – LaPlace’s Law: pressure = 4 X surface tension/radius • Pressure difference across the alveolar wall will be greater for alveoli with smaller radii for a given surface tension • Smaller alveoli would generate more pressure than a larger alveoli and would tend to empty into larger alveoli Surfactant to the Rescue • Surfactant is secreted by some of the alveolar epithelial cells • Synthesized in lungs from FA • Surfactant decreases surface tension in small alveoli more than large alveoli to eliminate the pressure difference Sphere has smallest SA for a given volume Advantages of Surfactant • A low surface tension in alveoli increases lung compliance and reduces work of expanding lungs • Alveoli are more stable – small do not empty into large alveoli • Helps keep alveoli dry – As surface tension forces tend to collapse the alveoli, they tend to suck fluid into the alveolar spaces from capillaries 5 Respiratory Zone Functions • • • • Surfactant production Endocrine functions Molecule activation and inactivation Blood clotting regulation Fick’s law • Gas diffuses through a sheet of tissue at a rate… – Directly proportional to tissue area (diffusion constant) – Directly proportional to pressure differential of gas on each side of membrane – Inversely proportional to tissue thickness – CO2 diffuses 20X faster than oxygen due to higher solubility of CO2 Gas Exchange • Body’s supply of oxygen depends on… – Concentration • 20.93% oxygen • 79.04% nitrogen • 0.03% carbon dioxide Diffusion • Primary means for gas movement and distribution • Gas pressures rapidly equilibrate on each side of the alveolar-capillary membrane • Fick’s law – governs gas diffusion through the alveolar membrane Pressure Changes • Pressure differential between air in lungs and lung-chest wall interface causes lungs to adhere to chest wall • Any change in thoracic cavity volume alters lung volume • Important as lungs contain no skeletal muscles to alter their volume ***Multimuscle respiratory pump system alters the volume of the lungs during inspiration and expiration Gas Exchange – Pressure in ambient air • Mixture of gases, total pressure exerted by gases is sum of the pressure of individual gases making up the mixture – Pressure is standardized to sea-level • Barometric pressure of 760 mm Hg • Above sea-level, barometric pressure is measured (PB) – PG is the portion of total pressure exerted by any single gas within the mixture and proportional to its percentage in the total gas mixture (Dalton’s law of partial pressures) 6 Partial Pressure •PG = PB X FG • Partial pressure of a gas (mm Hg) = total pressure (mm Hg) X fraction of the gas • PG = PB X FG • Note that as air enters the nasal cavities it completely saturates with water vapor, diluting the inspired mixture • At body temperature (37° C) water pressure is 47 mm Hg (760 – 47 = 713 mm Hg) • Effective PO2 = .2093 X 713 = 149 mm Hg • Humidification little effect on inspired PCO2 Alveolar Air Henry’s Law • CO2 enters alveoli from blood and O2 leaves lungs and enters blood • Gases diffuse from high pressure to low pressure • Rate of diffusion depends on… – Pressure difference between gas above the fluid and the gas dissolved in the fluid – Solubility of gas in the fluid • Quantity of Gas in a Fluid = Solubility Coefficient X (PG/total barometric pressure) Body • Dissolved O2 ~ 4% total oxygen consumed by body each minute at rest and <2% during maximal exercise For every unit of pressure favoring diffusion, ~ 25X more carbon dioxide than oxygen moves into/from a fluid 7 Gas Exchange in Lungs • Pressure gradients for gas transfer at rest – Oxygen - 60 mm Hg – Carbon dioxide – 6 mm Hg • Transfers rapidly due to solubility – Nitrogen – not used or produced in metabolic reactions so essentially unchanged – Gas exchanges occurs in ~0.25 which is 1/3 of time required for transit through the lungs (.75 sec) at rest and ½ this with exercise (transit time is .4 sec ) Exercise and Flow • During exercise, pulmonary capillaries increase blood volume X 3 • Maintain oxygenation during exercise • PO2 arterial blood slightly lower than alveolar PO2 Gas Transfer in Tissues • Rest – PO2 in muscle tissue is 40 mm Hg – Intracellular PCO2 av. 46 mm Hg • Vigorous Exercise – PO2 in muscle tissue falls toward 0 mm Hg – Intracellular PCO2 av. 90 mm Hg – Pressure differences between plasma and tissues facilitate oxygen delivery and carbon dioxide removal – Some blood in alveolar capillaries passes through poorly ventilated alveoli – Blood leaving the lungs joins venous blood from the bronchial and cardiac circulations • Note • Each liter of blood leaving the lungs contains about 50 mL of carbon dioxide – Provides the background level of carbon dioxide that is the chemical basis for ventilatory control through its stimulating effect on neurons of the pons and medullary centers of the brainstem Transport of Oxygen • Low solubility – 3 mL/L • Sustain life for ~ 4 sec • If dissolved oxygen provided the sole source of oxygen, need a Q of 80 L/min to supply resting metabolism (2X maximal exercise) • ??????????????????????????????????????? 8 Enters: Hemoglobin • Hemoglobin of RBC’s – Iron containing protein pigment – 280 million hemoglobin molecules in each of body’s more than 25 trillion RBC's – Carries 65-70 X more oxygen than dissolved in plasma – Temporarily captures and transports ~197 ml oxygen/L blood Oxygen Carrying Capacity • Men - 15 g Hb/dL • Women – 14 g Hb/dL • Hemoglobin carries nearly 20 mL of oxygen/dL of blood Hemoglobin • Hb4 + 4 O2 Hb4O8 • Each of 4 Fe atoms in hemoglobin can loosely bind one oxygen • No enzymes • Partial pressure of oxygen dissolved in dictates the oxygenation of hemoglobin to oxyhemoglobin Oxyhemoglobin Dissociation Curve • Oxygen saturation of Hb is %age of available binding sites that have oxygen attached – O2 combined with Hb/ O2 capacity X 100 – Arterial blood 97.5% of Hb saturated with oxygen (100 mm Hg) – Mixed venous blood – 75% saturation (40 mm Hg) Oxyhemoglobin Dissociation Curve • Depicts the oxygen % hemoglobin saturation and absolute oxygen concentration of blood for a given PO2 – High PO2 almost complete saturation = 20 ml/dL • PO2 of 100 mm Hg – Hb leaving lungs carries ~19.7 mL of oxygen/dL • Plasma contains 0.3 mL/dL in solution 9 Oxyhemoglobin Dissociation Curve Oxyhemoglobin Dissociation Curve • Hemoglobin saturation changes little until pressure of oxygen declines ~ 60 mm Hg • Steep lower portion of curve –peripheral tissues can withdraw large amounts of oxygen for only a small drop in capillary PO2 • Rest: PO2 in tissue = 40 mm Hg – Flat upper part of curve provides a margin of safety when have fluctuations in ambient PO2 • If alveolar PO2 drops to 75 mm Hg – Hb saturation decreases by only 6% – Hemoglobin loses about 30% of its oxygen • 20 ml to 15 ml/100 mL • Tissue utilized 5 ml/100 mL (a-v O2dif) Oxyhemoglobin Dissociation Curve • Exercise – oxygen utilization increases – Tissue PO2 decreases • 15 mm Hg • a-v O2dif = 15 ml/100 mL • Hb releases more oxygen Oxyhemoglobin Dissociation Curve • Decrease in pH – curve shifts downward and to right – Bohr Effect – – – – – Altered Hb structure (20-50 mm Hg) Oxygen affinity of Hb is decreased For a given PO2, more oxygen unloaded in tissue Increased a-v O2dif Primarily related to effect of increasing PCO2 on H+ concentration Oxyhemoglobin Dissociation Curve • Curve shifts downward and to right – Low pH (acidic) – Hypercarbic – Hot “Conditions associated with exercise” – 2,3-diphosphoglycerate (2,3 DPG) – produced by RBC’s and binds Hb, decreasing its affinity for oxygen – compensatory mechanism • Cardiopulmonary disease • High altitude 10 Altitude • Barometric pressure decreases exponentially with distance above the earth’s surface – 19,000 ft - ½ normal 760 mm Hg (380 mm Hg) – PO2 = 70 mm Hg – Summit of Mt Everest (29,029 ft) inspired PO2 = 43 m Hg Myoglobin vs Hemoglobin • Myoglobin found in skeletal and cardiac muscle fibers • Intramuscular storage of oxygen • Each myoglobin molecule contains one Fe atom • Facilitates the transfer of oxygen to mitochondria when exercise begins and during intense exercise when cellular PO2 declines rapidly • Myoglobin dissociation curve – rectangular hyperbola – Low end of PO2 values – high saturation of myoglobin with small increase in PO2 Acclimatization • Hyperventilation – Reduces PCO2 raising alveolar PO2 • Residents at 15,000 ft - PCO2 = 33 mm Hg vs 40 m Hg at sealevel • Hypoxic stimulation of the peripheral chemoreceptors • Polycythemia – increased RBC concentration of blood • Residents at 15,000 ft – arterial PO2 = 45 mm Hg but arterial oxygen saturation is only 81% due to increased Hg (15 to 19.8 gm/100mL) • Hypoxemia – causes release of erythropoietin from kidney which stimulates bone marrow Myoglobin • PO2 = 40 mm Hg, myoglobin holds 95% of its oxygen (rest and light exercise) • As PO2 drops, the greatest quantity of oxygen is released from myoglobin • Myoglobin is not affected by pH, temperature or carbon dioxide 11 Carbon Dioxide Transport • 3 forms – Dissolved – Bicarbonate (HCO3- ) – In combination with proteins as carbamino compounds Dissolved Carbon Dioxide • ~ 5-10% of arterial carbon dioxide moves into solution • Establishes the PCO2 of blood Bicarbonate (70-75%) • Tissue… Carbonic Anhydrase • CO2 + H2O H2CO3 H+ + HCO3• Reaction facilitated by carbonic anhydrase – enzyme in RBC – 5,000 faster • When HCO3- concentration rises in RBC, it diffuses out • To maintain chemical neutrality, Cl- ions move into RBC (chloride shift) Bicarbonate • Some of H+ ions liberated are bound to Hb – Triggers the Bohr Effect – formation of HCO3enhances oxygen unloading – Hb acts as a buffer, preventing significant increases in acidity • Lungs where PCO2 is low – reaction reverses O2 + HHb HbO2 + H+ + H + HCO3 H2CO3 CO2 + H2O 12 Carbamino Compounds (20%) • CO2 combines with terminal amine group in blood proteins • Most important protein is globin of hemoglobin HbNH2 + CO2 HBNHCOOH – Occurs rapidly without an enzyme • When reach lungs plasma PCO2 decreases and oxygenation of Hb reduces its ability to bind carbon dioxide Pulmonary Functions Factors Affecting Performance on Pulmonary Tests • Motivation given to subject • Position – standing optimal • Illness – cold, allergy, etc. Tests • Static lung functions – volumes • Dynamic lung functions – volume and velocity 13 Determinants of Lung Functions (prediction) • • • • Race Age Gender Height Dynamic Functions • Maximal Voluntary Ventilation (MVV) – Volume of air that could be moved during vigorous, deep breathing (extrapolated to a minute) – Test of ventilatory capacity – 140-180 L/min (men) – 80 – 120 L/min (women) – Training of ventilatory muscles increases MVV Dynamic Tests • Velocity dependent on – Airway resistance – Resistance of lung tissue to change in shape Dynamic Functions • Single forced expiration – FVC – total volume exhaled – FEV1.0 – volume exhaled in first second – FEV1.0/FVC – Forced expiratory ratio (FER) • % – Peak expiratory flow rate (PEFR) – highest forced expiratory flow • L/min – FEF25-75% - Forced expiratory flow rate • Average flow rate measured over the middle half of the expiration (related to FEV1.0 ) Types of Pulmonary Disorders • Restrictive – low lung volumes • • • • • Pulmonary fibrosis Kyphoscoliosis FVC < 80% of predicted FEV1.0/FVC > 70% (normal for lower lung volume) Inspiration limited by reduced compliance or weak inspiratory muscles Types of Pulmonary Disorders • Obstructive - low flow rates – – – – Asthma Bronchitis Emphysema FEV1.0/FVC < 70% 14 Pulmonary Screening • • • • Check for signs of restrictive disease: Msd FVC/Pred FVC < 80% Predict FVC – equation – Chp 4 Example – 30 yr old, female, 64 inches, FVC = 3.20, FEV1.0 = 2.5 L Pulmonary Screening • Check for signs of obstructive disease: – msd FEV1.0/ msd FVC < 70% – 2.5/3.2 = .78 X 100 = 78% – Normal • Ok, so recheck in ……. years FVC = (0.0414 X ht (cm) – (0.0232 X 30) – 2.2 FVC = (0.0414 X 162.6) – (0.0232 X 30) – 2.2 Predicted FVC = 3.83 L 3.2/3.83 = .84 X 100 = 84% - normal Example • • • • Asian male, age 35 years, 63 in. tall FVC = 2.1 L FEV1.0 = 1.33 L Restrictive disease: – Predicted = 3.89 X 0.85 = 3.31 L – 2.14/3.31 = 64% (refer < 80%) • Obstructive disease: – 1.33/2.1 = 62% (refer < 70%) Flow Volume Loops • Subject inspires to total lung capacity and then exhales as hard as he can to residual volume • Flow rate is independent of effort over most of the lung volume – High volumes – expiratory flow rate increases with effort but at med and low volumes, flow rate plateaus – WHY?????? • Compression of airways by intrathoracic pressure 15 Asthma • Reversible, bronchospasm triggered by allergy, exercise, infections or environmental irritants – EIA (Exercise Induced Asthma) – epithelial water loss and cooling of airways – S/S - Increased secretion of nasal mucous, dry, nonproductive cough, wheezing, SOB Bronchitis • Inflammatory disorder of small airways in lung • Common in smokers • Productive cough, wheezing, reduced arterial O2 saturation and increased CO2 due to hypoventilation EIA • Most problematic – cold, dry environments • 1984 Olympics Games in LA – 11% US team – chronic EIA – Won 41 medals Emphysema • Gradual destruction of lung alveolar cell units and connective tissue and airway inflammation • Enlargement of alveoli • Loss of supporting tissue • Airway collapse during expiration • Total lung volume increases • Dyspnea on exertion • Limited functional capacity • Arterial Desaturation 16 Static Lung Volumes Respiratory Center • Brainstem (medulla and pons) • Establishes rate and depth of breathing • Input from chemoreceptors, receptor stretching in lungs Oxygen Cost Ventilation during Exercise • Rest – 1-2% of total body oxygen consumption • Heavy exercise - > 15% of total body oxygen consumption • Pulmonary ventilation not a limiting factor in maximal performance unless restrictive or obstructive lung disease • Respiratory muscles better designed for avoiding fatigue during long-term activity than muscles of extremities 17 Ventilation During Exercise • Ventilation - two-phase increase • Immediate increase followed by a continued gradual rise – Initial – produced by mechanics of the body’s movements Entrainment • A synchronization of limb movement and breathing frequency • Those who exhibit his have a lower energy cost during exercise automatically • Motor cortex transmitting impulses to respiratory center • Proprioceptive feedback from muscles to respiratory center Ventilation During Exercise – More gradual increase in second phase • Produced by changes in the temperature and chemical status of the arterial blood – H+, carbon dioxide, heat enhance unloading in muscles – Increases arterial-venous dif – More carbon dioxide enters blood • Stimulates chemoreceptors which stimulate the inspiratory center increasing rate and depth of breathing Ventilation Post Exercise • Energy demand drop immediately • Pulmonary ventilation returns to normal at a slow rate – Due to acid-base balance – Carbon dioxide – Temperature 18