Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Reduced Toxicity of Liposome-Associafed
Amphotericin B Injected Intravifreally in Rabbits
Claude Tremblay,*t Michael Barza,*^: Francis Szoka,§:j: Moshe Lahav,||H and Jules
The ocular toxicity of liposome-intercalated amphotericin B and commerical amphotericin B were
compared after intravitreal injection in healthy pigmented rabbits. Ophthalmoscopic observations
over 5 weeks following a single intravitreal injection showed vitreal band formation and focal retinal
damage after doses of .commercial amphotericin B as low as 5 Mg- Such lesions were not seen in
animals given liposomal amphotericin B in doses up to 20 ng. Histopathologic examination showed
areas of retinal atrophy or necrosis in five of 16 rabbits given commercial amphotericin B in doses of
5-20 Mg but in none of 16 rabbits given the same doses of liposomal amphotericin B (P = 0.02).
Small white vitreal bodies were seen clinically in virtually all animals given liposomal amphotericin
B or "empty" (drug-free) liposomes but in only a few animals given commercial amphotericin B;
these deposits may represent residual lipid. Concentrations of amphotericin B ranged from 0.4 to 1.0
jug per ml of vitreous humor 5 weeks after injection of 5-20 Mg of either formulation. These studies
indicate that liposome association markedly reduces the ocular toxicity of amphotericin B. Invest
Ophthalmol Vis Sci 26:711-718, 1985
Amphotericin B is a drug of choice for a number
of serious fungal infections of the eye including
Candida endophthalmitis, postsurgical fungal endophthalmitis, and mucormycosis, and is an alternative
to natamycin in the treatment of fungal keratitis.1"3
Unfortunately, intraocular penetration of amphotericin B is poor following systemic administration in
rabbits,4 although modest levels were found in the
aqueous and vitreous humor of two patients whose
eyes were enucleated because of severe fungal infection. 5 Subconjunctival injection of amphotericin B
penetrates the ocular humors of rabbits very poorly4
and is prone to produce severe local tissue reactions.6
Direct intravitreal injection of amphotericin B is
attractive because it produces high concentrations at
the site of infection in fungal endophthalmitis. Axelrod
et al7 found that normal rabbits tolerated intravitreal
injections of 10 /u.g of amphotericin B without toxicity
if the drug was administered slowly into the center
of the vitreous humor. In contrast, Souri and Green1
reported marked retinal damage in this same species
with intravitreal doses as low as 1 jig. In one patient
with Candida albicans endophthalmitis, intravitreal
injection of 5 /xg of amphotericin B appeared to
produce no residual ocular toxicity.8
Recent studies have indicated that incorporation
of amphotericin B into liposomes markedly reduces
the acute toxicity of the drug while retaining efficacy
in animal models of fungal infection.9"" We have
developed a liposomal formulation of amphotericin
B, which is approximately one-fifth as toxic as the
commercial drug in terms of acute lethality after
intravenous injection in mice but is fully active in
vitro and in the treatment of systemic candidiasis in
mice." a In the present study we have compared the
ocular toxicity of commercial amphotericin B with
that of our liposomal formulation after intravitreal
injection in rabbits.
Materials and Methods
Drug Preparations
From the Infectious Disease Division, Department of Medicine,*
and the Department of Ophthalmology, || Tufts-New England
Medical Center, Boston, Massachusetts, and the School of Pharmacy^ University of California, California.
Supported in part by research grant EY-01517 from the National
Eye Institute,:): the Massachusetts Lions Eye Research Fund, Inc.,H
and Fonds F.C.A.C. pour l'Aide et le Soutien de la Recherche,f
Province of Quebec, Canada.
Submitted for publication: September 30, 1983.
Reprint requests: Michael Barza, MD, New England Medical
Center, 171 Harrison Avenue, Boston, MA 02111.
Amphotericin B was obtained from the Squibb
Institute (Princeton, NJ) as the commercial preparation for intravenous use. This formulation contains
sodium desoxycholate as a solubilizing agent.
Small unilamellar vesicles were prepared by sonication in a bath type sonicator 12 from a lipid composition of egg phosphatidylcholine (Avanti Polar
Lipids; Birmingham, AL) cholesterol, and tocopherol
succinate (Sigma Chemical; St. Louis, MO) in a
711
Downloaded From: http://arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933354/ on 05/12/2017
712
INVESTIGATIVE OPHTHALMOLOGY & VISUAL SCIENCE / Moy 1985
molar ratio of 5:3:1. The lipids were deposited on the
sides of a round bottom flask by evaporation from a
chloroform solution. Amphotericin B in dimethylsulfoxide was added to the dried lipids at a 10 mole
percent ratio. Phosphate-buffered saline (PBS; composition 137 mM NaCl, 2.6 mM KC1, 6.4 mM
Na 2 HPO 4 , pH 7.4) was added to the flask to rehydrate
the lipids and to give a final lipid concentration of
50 jumol/ml.
The dispersion was hydrated under nitrogen for 10
min and then sonicated under nitrogen for 60 min
at room temperature. The slightly opalescent yellow
preparation was dialyzed at 4°C against 200 volumes
of PBS, changed two times over a 24-hr period to
remove nonintercalated amphotericin B and dimethylsulfoxide. A typical preparation retained 70% of the
initial amphotericin B (3525 ng amphotericin B per
50 /xmoles total lipid per ml). The liposomes were
sterilized by filtration through a sterile 0.22 jum filter
(Millipore; Bedford, MA) into a sterile container.
Drug concentration in the liposome dispersion was
determined by diluting an aliquot of the final preparation 1/1000 in methanol, measuring the absorbance
at 388 nm and 406 nm, and comparing it with a
standard curve prepared from solid amphotericin
diluted in methanol. The standard curve was linear
up to 6 Mg/ml of amphotericin B.
The liposome weight average diameter was estimated by dynamic light scattering using a Malvern
light scattering monochromator (Cherry Hill, NJ)
coupled to a Spectraphysics 15 mW helium (633 nm)
fixed wavelength laser.
Injections
Twenty healthy pigmented (Dutch-belted) rabbits,
weighing 1.5-2.5 kg, were used. All studies were
carried out in accordance with the ARVO Resolution
on the Use of Animals in Research. Amphotericin B
and liposomal amphotericin B were diluted in sterile
distilled water to an appropriate concentration such
that the intravitreal dose would be contained in 0.1
ml. The concentration of drug in the liposomal
suspension was verified by spectrophotometric absorbance at 388 nm and 406 nm.
Each of the forty eyes was randomly assigned to
receive one of 10 intravitreal regimens: amphotericin
B or liposomal amphotericin B in a dosage of 1, 5,
10, or 20 ng, or a control preparation consisting of
PBS or drug-free ("empty") liposomes. The latter
were prepared in the same way as drug-containing
liposomes. The controls given empty liposomes received the same amount of lipid as was present in
the 20 fig injection of liposomal amphotericin B.
Each preparation was administered to four eyes in
Vol. 26
four animals. The volume injected was 0.1 ml in
each instance.
In preparation for the intravitreal injections, the
rabbits were tranquilized with an intramuscular injection of ketamine 90 mg and acepromazine maleate
1 mg. Proparacaine hydrochloride 0.5% was then
applied topically. The intraocular volume was decreased by aspiration of 0.1-0.2 ml of aqueous humor
through a 25-gauge needle. The superior rectus muscle
was gently grasped with a forceps to stabilize and
proptose.the globe. A 27-gauge needle attached to a
tuberculin syringe was introduced about 5 mm posterior to the limbus and was inserted to the approximate center of the vitreous humor. The solution (0.1
ml) was injected slowly.
Ophthalmoscopic and Histologic Studies
The rabbits' eyes were examined once a week with
a direct ophthalmoscope and a slit lamp after dilatation with atropine sulfate 1%. All examinations were
made by one observer who did not know which
preparation had been administered.
After 5 weeks, the animals were killed with an
intravenous injection of pentobarbital, and the eyes
were promptly enucleated. The vitreal lesions appeared
stable by this time. About 0.4 ml of vitreous humor
was aspirated through a 25-gauge needle for assay of
the amount of amphotericin B remaining (see below);
this volume was promptly replaced by an equal
volume of phosphate-buffered saline to maintain the
volume of the globe.
The eyes were placed in 10% phosphate-buffered
formalin. After fixation, they were properly oriented
and a pupil-optic nerve section was cut along the
vertical axis. A central segment was processed for
paraffin embedding, sectioned at 6 /xm, and stained
with hematoxylin and eosin. Selected sections were
stained with periodic acid-Schiff reagent. Sequential
sections were observed for inflammatory changes in
the vitreous humor and for retinal abnormalities. All
interpretations were made by one observer who was
not aware of which preparation had been administered. The changes were graded as follows:
Vitreal inflammation: Vitreal inflammation was
graded as follows: ± = few monocular cells along
vitreous base per high power field (40X on AO
Ultrastar microscope, American Optical USA; Buffalo,
NY); 1+ = 10-20 cells along the vitreous base per
high power field; 2+ = 20-40 cells per high power
field at the vitreous base and elsewhere; 3+ = >40
cells per high power field at the vitreous base and
elsewhere.
Retinal atrophy or necrosis: These changes were
designated as focal or diffuse as estimated by the
Downloaded From: http://arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933354/ on 05/12/2017
713
TOXICITY OF INTRAVITREAL LIPOSOAAAL AMPHOTERICIN D / Trembloy er ol.
No. 5
anteroposterior involvement in sections from the
central segment of the globe.
VITREAL BODIES
Assay of Amphotericin B in Vitreous Humor
Residual amphotericin B was assayed by an HPLC
method followed methanol extraction, with o-nitrophenol serving as internal standard.13 Activity was
read spectrophotometrically at 388 nm.
0
1+
None
5-10 per eye
None
Minimal
2+
10-25 per eye
Moderate
3+
>25 per eye
Severe
l ""
0
Retinal damage
None
Silvery sheen or
atrophy of
retina
occupying
0.5-1 whole
field visible at
one time
Retinal sheen or
atrophy
occupying > 1
field visible at
one time
More extensive
than above
(no such
lesions
actually
found)
LESION
Lip-AMB Sug
AMB S ug
2+
1+
During the first week after injection, all but four
eyes showed a moderate diffuse inflammatory cellular
reaction in the vitreous humor, particularly in the
anterior part, and all but six eyes showed scattered
small white vitreal bodies. By the second and third
weeks, the diffuse inflammatory reaction decreased
or disappeared although the vitreal bodies remained.
These opacities were sparkling white, were less than
1 mm in diameter, were mostly located in the lower
part of the eye, and did not move when the animal's
head was moved. In some eyes, bands of "veil-like"
vitreal condensations began to appear, sometimes
seeming to exert traction on the retina.
During the fourth and fifth weeks, the vitreal
bodies and vitreal bands remained unchanged. Retinal
damage was noted in a few eyes, being manifested by
a silvery sheen of the retina, generally in areas adjacent
to the fibrotic vitreal bands. In a few animals, slitlamp examination revealed cataract formation.
A grading system, summarized in Table 1, was
used to quantify the extent of these gross changes 5
weeks after injection when vitreal lesions appeared to
be stable. Intermediate values were scored with halfTable 1. Scoring system for vitreal and retinal
abnormalities observed on direct ophthalmoscopy
Vitreal
bands
3+
OF
Ophthalmoscopic Examination
Vitreal
opacities
J
J«»-r
GRADE
Results
Grade
AMB 1ug
1
11
44
3+
Lip-AMB 10 ug
11
Lip-AMB 20 ug
J
LULI
Empty liposomes
1
2
3
EYE NUMBER
4
1
2
3
4
EYE NUMBER
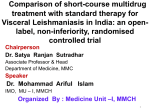
Fig. 1. Gross toxicity of intravitreal amphotericin B. Extent of
vitreal opacities observed ophthalmoscopically 5 weeks after intravitreal injection of commercial amphotericin B (AMB) or liposomal
amphotericin B (lip-AMB) in the indicated dosages in pigmented
rabbits. Each bar is the result in one eye using the scoring system
shown in Table 1. Control eyes received phosphate-buffered saline
(PBS) or empty (drug-free) liposomes.
increments (eg, between 1+ and 2+ = 1.5). Figure 1
shows the density of vitreal bodies for each of the
four eyes in the eight treatment groups and two
control groups (PBS and drug-free or "empty" liposomes). As can be seen, vitreal bodies were evident
in most animals given liposomal amphotericin B or
empty liposomes. It is not clear that these opacities
signify a toxic reaction; they may, instead, represent
residual liposomes. However, some were seen in eyes
that received no liposomes.
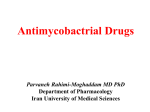
Figure 2 shows the extent of vitreal band formation
and of retinal damage seen clinically in these same
animals. These reactions, which were clearly due to
adverse drug effects, were evident in most eyes given
amphotericin B in doses of 5 /xg or more, but were
absent from all but one of the eyes treated with
liposomal amphotericin B.
Cataracts were observed in four eyes, one each
treated with amphotericin B, 5 jug, 10 /zg, or 20 /ug
and one given liposomal amphotericin B, 5 ug. A
faint focal cortical opacity was seen in one eye treated
Downloaded From: http://arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933354/ on 05/12/2017
714
INVESTIGATIVE OPHTHALMOLOGY G VISUAL SCIENCE / May 1985
|_| VITREAL BAND FORMATION
|
RETINAL DAMAGE
4+
3+
2+
14-
AMB 1 ug
•
I H
0
44
-
24
• i
1+
OF
0
LESION
Lip-AMB Sug
AMB 5ug
3+
GRADE
Lip-AMB 1ug
r-m
P
|
4+
3+
Lip-AMB 10 ug
AMB 10 ug
2+
1+
o
• IIIL B• H• 1
4+
3+
2+
AMB 20 ug
Lip-AMB 20 ug
1+
0
_
'Ill |
44
34
24
Empty liposomet
PBS
14
o
1
2
3
4
EYE NUMBER
EYE NUMBER
Fig. 2. Gross toxicity of intravitreal amphotencin B. Extent of
vitreal band formation and retinal damage observed ophthalmoscopically 5 weeks after intravitreal injection of commercial amphotericin B (AMB) or Hposomal amphotericin B (lip-AMB) in the
indicated dosage in pigmented rabbits. Each bar is the result in one
eye using the scoring system shown in Table I. Control eyes
received phosphate-buffered saline (PBS) or empty (drug-free) liposomes.
with liposomal amphotericin B, 10 ug. The lenticular
opacities were located in the posterior cortex.
Histologic Studies
The results of histologic examination are summarized in Table 2. Vitreal inflammation, manifested
primarily by round cells along the vitreous base, was
Vol. 26
generally slight. Although some inflammation was
noted in all groups, there was a suggestion of a
somewhat more marked reaction in animals receiving
higher doses of liposomal amphotericin B. We did
not analyze vitreal band formation histologically because of the possibility that some of the effects
observed may have been caused by aspiration of the
vitreous humor for assay of amphotericin B.
Microscopic examination of the retina revealed
damage in five eyes, all of which had been treated
with amphotericin B. In one eye injected with amphotericin B, 5 ug, there was atrophy and necrosis
over 80% of the inferior retina. Another eye treated
in the same manner exhibited focal (2 X 1 mm)
retinal atrophy (Figs. 3A and B). One eye injected
with amphotericin B, 10 ug, displayed retinal necrosis
in one area inferiorly ( 4 X 4 mm) and hypertrophy
of the retinal pigment epithelium. A fourth eye,
which had been treated with amphotericin B, 20 ug,
showed retinal atrophy and focal atrophy of the
retinal pigment epithelium (3 X 1 mm). In the fifth
eye, injected with amphotericin B, 20 ixg, diffuse
necrosis was seen over the lower half of the retina
(Figs. 4A and B). The first three eyes described above
had been noted to have retinal damage on ophthalmoscopic examination. Overall, five of 16 eyes treated
with amphotericin B, but none of 16 treated with
liposomal amphotericin B, exhibited histologic retinal
abnormalities (P = 0.0217 by Fisher exact test, twotailed). All of the microscopic abnormalities were
observed with doses of amphotericin B of 5 fig or
more. None of the eyes injected with "empty" liposomes showed retinal damage histologically.
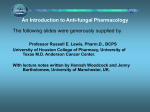
Vitreal Concentrations of Amphotericin B
Figure 5 shows the concentrations of amphotericin
B measured in the vitreous humor 5 weeks after
injection. Several specimens were lost for technical
reasons. No drug was detectable in eyes given 1 ug
of amphotericin B and an unexpectedly high concen-
Table 2. Histologic abnormalities in rabbits given intravitreal amphotericin B (AMB) or liposomal
amphotericin B (lip-AMB) (each group included four eyes)
Vitreal inflammation
Lip-AMB
AMB
Dose of AMB
±
+
0 (empty liposomes)
I
5
10
20
1
3
2
1
Total
++
±
1
1
1
2
2
1
2
8
4
0
5
+
Retinal abnormalities
++
AMB
Lip-AMB
1
2
1
3
1
0
0
2 (1 focal, 1 diffuse)
1 (focal)
2 (1 focal, 1 diffuse)
0
0
0
0
0
7
1
Downloaded From: http://arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933354/ on 05/12/2017
No. 5
TOXICITY OF INTRAVITREAL UPOSOMAL AMPHOTEPJCIN D / Trembloy er ol.
715
Fig. 3. A, top. Equatorial retinal lesion in a rabbit injected intravitreally with 5 /ig of amphotericin B. Note atrophy of all layers, more
marked in the inner layers of the retina. The outer nuclear layer is thinned (hematoxylin and eosin, XI20). B, bottom. Equatorial retina in
a rabbit injected with 5 fig of liposomal amphotericin B. The retinal architecture is normal (hematoxylin and eosin, XI20).
tration of 1.4 ^g/ml was detected in the only eye
studied after 1 jug of liposomal amphotericin B.
Concentrations were in the range of 0.4-1.0 jug/ml
in eyes injected with 5-20 ng of amphotericin B or
liposomal amphotericin B. There was no obvious
difference in concentration between eyes treated with
liposomal or nonliposomal preparations. If one considers that, in these small rabbits, the initial dose of
Downloaded From: http://arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933354/ on 05/12/2017
No. 5
TOXICITY OF INTRAVITREAL LIPOSOMAL AMPHOTERICIN D / Trembloy er ol.
715
'•I
3 ,;
Fig. 3. A, top. Equatorial retinal lesion in a rabbit injected intravitreally with 5 fig of amphotericin B. Note atrophy of all layers, more
marked in the inner layers of the retina. The outer nuclear layer is thinned (hematoxylin and eosin, XI20). B, bottom, Equatorial retina in
a rabbit injected with S jig of liposomal amphotericin B. The retinal architecture is normal (hematoxylin and eosin, XI20).
tration of 1.4 fig/ml was detected in the only eye
studied after 1 fig of liposomal amphotericin B.
Concentrations were in the range of 0.4-1.0 fig/ml
in eyes injected with 5-20 fig of amphotericin B or
liposomal amphotericin B. There was no obvious
difference in concentration between eyes treated with
liposomal or nonliposomal preparations. If one considers that, in these small rabbits, the initial dose of
Downloaded From: http://arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933354/ on 05/12/2017
No. 5
717
TOXICITY OF INTRAVITREAL UPOSOMAL AMPHOTERICIN D / Trembloy er ol.
four half-lives, suggesting a vitreal half-life of amphotericin B of approximately 9-12 days.
Discussion
Amphotericin B has been a mainstay in the treatment of fungal endophthalmitis. 14~16 Jones2 has documented that within the past two decades, candidal
endophthalmitis has emerged as the most common
ocular fungal infection. Several case reports support
the effectiveness of amphotericin B, given by
subconjunctival 1718 or intravitreal8 injection in the
treatment of fungal endophthalmitis. However, the
toxicity of amphotericin B may limit its effectiveness.
Recent experiments in our laboratory have shown
that liposome association of amphotericin B strikingly
reduces the toxicity of the drug after systemic administration in mice. The acute LD 50 of commercial
amphotericin B in this animal is approximately 2.27
mg/kg, whereas the acute LD 50 of the liposomal
preparation is 11.75 mg/kg. lla Similar reductions in
toxicity with liposomal formulations of amphotericin
B have been reported by others. 9 "" We have also
shown that liposomal amphotericin B retains full
antifungal activity in vitro.1 la Finally, we" a and
others 9 "" have demonstrated that liposomal amphotericin B can be given safely in higher doses than
commercial amphotericin B to animals with systemic
fungal infections thereby achieving higher survival
rates. The small unilamellar vesicles that we used
have a diameter of approximately 0.1 ^m so that
they can be sterilized by passage through a 0.22 j^m
filter. The reduced systemic toxicity of liposomal
amphotericin B led us to test the preparation for
ocular toxicity after intravitreal injection in rabbits.
During the first 1 to 2 weeks after intravitreal
injection of amphotericin B or liposomal amphotericin
B, a vitreal haze consistent with leukocytic infiltration
was observed in most eyes. Thereafter, the major
clinical changes consisted of vitreal "bodies", ie, small
white sparkling opacities mainly located in the lower
part of the eye, vitreal condensations, and retinal
abnormalities. Vitreal bodies were noted predominantly in animals given liposomal preparations. They
may represent residual lipid. However, they were also
noted in some eyes treated with nonliposomal formulations. Their histologic counterparts may have
been eluted during tissue processing. Further studies
will be needed to elucidate the nature of these particles
and to determine how long they remain in the eye.
Vitreal band formation and retinal damage of
grade 1+ or greater were clinically evident only in
eyes treated with amphotericin B alone. This strongly
suggests that liposome association reduces the acute
inflammatory effect of the drug. Cataract formation
was observed in one of 20 eyes given amphotericin
__ 2 . 0 -
1 1.8m
.E
1.4-
'|
1.2-
o
o
1.60
o
o
f 1.0o
=
0.6-
•
o
o
o
•
°
1
o
.
•
§
Lip-AMB
AMB
0.4-
lo.2«5 o
AMB
Lip-AMB
ug
AMB Lip-AMB
5 ug
AMB
10 ug
Lip-AMB
20 ug
Fig. 5. Concentration of amphotericin B in the vitreous humor
of rabbits 5 weeks after intravitreal injection of commercial amphotericin B or liposomal amphotericin B in the dosage indicated.
Each point is the result for one eye. Assays were done by HPLC.
B and in three of 20 eyes given liposomal amphotericin
B. Although we cannot exclude trauma as a cause of
the cataracts, we were careful to direct the needle
posteriorly. Neither the distribution of cataracts among
the treatment groups nor their morphologic appearance permits us to interpret their cause or significance.
On histologic examination, vitreal inflammation,
chiefly in the form of a round-cell infiltrate along the
vitreous base, was noted in over half of the eyes,
including two eyes treated with PBS. Inflammation
of grade 1+ or 2+ was noted in four of 16 eyes
injected with amphotericin B but eight of 16 injected
with liposomal amphotericin B, suggesting a somewhat
more irritating effect of the liposomal drug. However,
the relation between vitreal inflammation and substance or dose of substance administered was inconclusive.
If we consider retinal necrosis or atrophy as the
most significant histologic lesions, there was a marked
benefit of liposomal amphotericin B. Retinal damage
was detected histopathologically in five of 16 eyes
treated with amphotericin B but none of 16 given
liposomal amphotericin B (P = 0.0217 by Fisher exact
test). This corresponds to the clinical finding that
significant retinal damage was confined to the animals
given amphotericin B alone. Although it is conceivable
that needle trauma caused the atrophic changes noted
in two of the eyes, it is unlikely to have produced the
more extensive changes observed in the other three
eyes. Moreover, only animals given nonliposomal
drug manifested these abnormalities, which should
not be the case if trauma due to the injection were
responsible for the changes. We did not control for
the direction of the needle bevel in making the
injections, but we presume that this varible was
randomly distributed among the eyes. We cannot
rule out the possibility that the desoxycholate solu-
Downloaded From: http://arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933354/ on 05/12/2017
718
INVESTIGATIVE OPHTHALMOLOGY & VISUAL SCIENCE / May 1985
bilizer present in commercial amphotericin B played
some role; however, Axelrod et al7 found that desoxycholate was not toxic in the doses used in this
study.
The mechanism by which liposome-association
reduces the toxicity of amphotericin B without reducing its antifungal activity is not clear. In contrast
to water-soluble molecules, which are trapped in the
interior (aqueous phase) of liposomes, amphotericin
B is presumably intercalated in the wall of the liposome.19 The antibiotic has an affinity for sterols
present in the liposomes and in human and fungal
cellular membranes. Its greatest affinity is for ergosterol, which occurs naturally in fungal cells but not
human cell membranes. It may be that the interaction
between amphotericin B and human cell membranes
is reduced by the competitive effect of the liposomal
cholesterol but that the drug is readily captured by
fungal ergosterol.
Concentrations of amphotericin B of 0.4-1.0 /xg/
ml were found in the vitreous humor 5 weeks after a
single intravitreal injection of 5-20 ng. The apparent
clearance rate of amphotericin B from the vitreous
humor was similar for liposomal and nonliposomal
preparations. However, our data do not permit us to
determine whether amphotericin B administered in
liposomes was cleared as the drug-liposome complex
or after the drug had become separated from the
liposomes. More detailed pharmacokinetic studies
underway in our laboratory suggest that amphotericin
B has a long half-life in the vitreous humor, choroid,
and retina following intravitreal injection. Accordingly, intravitreal injections may not have to be
repeated often to maintain relatively high levels of
drug in pertinent sites.
The results of this study offer some hope that
liposome-intercalation may reduce the toxicity of
intravitreal amphotericin B, thereby permitting this
valuable drug to be used more safely in the treatment
of fungal endophthalmitis. Our data suggest that
further study of the safety and efficacy of intraocular
liposomal amphotericin B is warranted.
Key words: amphotericin B, liposomes, intravitreal, toxicity,
rabbit
References
1. Souri EN and Green WR: Intravitreal amphotericin B toxicity.
Am J Ophthalmol 78:77, 1974.
Vol. 26
2. Jones DB: Therapy of postsurgical fungal endophthalmitis.
Trans Am Acad Ophthalmol Otolaryngol 85:357, 1978.
3. Ghosheh R: Polyene antibiotics. In Antimicrobial Agents in
Ophthalmology, Smolin G and Okumoto M, editors. New
York, Masson Publishing USA, 1983, pp. 107-110.
4. Green WR, Bennett JE, and Goos RD: Ocular penetration of
amphotericin B: a report of laboratory studies and a case report of postsurgical cephalosporium endophthalmitis. Arch
Ophthalmol 73:769, 1965.
5. Fisher JF, Taylor AT, Clark J, and Rao R: Penetration of
amphotericin B into the human eye. J Infect Dis 147:164,
1983.
6. Bell RW and Ritchey JP: Subconjunctival nodules after amphotericin B injection. Arch Ophthalmol 90:401, 1973.
7. Axelrod AJ, Peyman GA, and Apple DJ: Toxicity of intravitreal
injection of amphotericin B. Am J Ophthalmol 76:578, 1973.
8. Stern GA, Fetkenhour CL, and O'Grady RB: Intravitreal
amphotericin B treatment of Candida endophthalmitis. Arch
Ophthalmol 95:89, 1977.
9. Taylor RL, Williams DM, Craven PC, Graybill JR, Drutz DJ,
and Magee WE: Amphotericin B in liposomes: a novel therapy
for histoplasmosis. Am Rev Respir Dis 125:610, 1982.
10. Graybill JR, Craven PC, Taylor RL, Williams DM, and Magee
WE: Treatment of murine cryptococcosis with liposome-associated amphotericin B. J Infect Dis 145:748, 1982.
11. Lopez-Berestein G, Mehta R, Hopfer RL, Mills K, Kasis L,
Menta K, Fainstein V, Luna M, Hersh EM, and Juliano R:
Treatment and prophylaxis of disseminated infection due to
Candida albicans in mice with liposome-encapsulated amphotericin B. J Infect Dis 147:939, 1983.
lla.Tremblay C, Barza M, Fiore C, and Szoka F: Efficacy of
liposome-intercalated amphotericin B in the treatment of systemic candidiasis in mice. Antimicrob Agents Chemother 26:
170, 1984.
12. Szoka F and Papahadjopoulos D: Comparative properties and
methods of preparation of lipid vesicles (liposomes). Annu Rev
Biophys Bioeng 9:467, 1980.
13. Mayhew JW, Fiore C, Murray T, and Barza M: An internallystandardized assay for amphotericin B in tissues and plasma.
JChromatogr 274:271, 1983.
14. Michelson PE, Stark W, Reeser F, and Green WR: Endogenous
Candida endophthalmitis. Int Ophthalmol Clin 2:125, 1971.
15. Edwards JE Jr, Foos RY, Montgomerie JZ, and Guz LB:
Ocular manifestation of Candida septicemia: review of 76 cases
of hematogenous Candida endophthalmitis. Medicine 53:47,
1974.
16. Clarkson JG and Green WR: Endogenous fungal endophthalmitis. In Clinical Ophthalmology, Duane TD, editor. Hagerstown, Harper and Row, 1976, pp. 1-44.
17. Allen HF: Amphotericin B and exogenous mycotic endophthalmitis after cataract extraction. Arch Ophthalmol 88:640, 1972.
18. Glassman MI, Henkind P, and Alture-Werber E: Monosporium
apiospermum endophthalmitis. Am J Ophthalmol 76:821,
1973.
19. Andreoli TE: On the anatomy of amphotericin B-cholesterol
pores in lipid bilayer membranes. Kidney Int 4:337, 1973.
Downloaded From: http://arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933354/ on 05/12/2017