Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
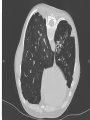
The primary care management of Bronchiectasis Andrew White Consultant Respiratory Physician Gloucestershire Royal Hospital Respiratory Lead GHNHSFT COPD Lead GHNHSFT Sally King Respiratory Specialist Physiotherapist Gloucestershire Care Services When to consider the diagnosis How to make the diagnosis What is the role of secondary care How to manage patients in the community What is Bronchiectasis? Bronchiectasis is a condition in which symptoms of persistent or recurrent bronchial sepsis related to irreversibly damaged and dilated bronchi Usually separated into cystic fibrosis (CF) associated bronchiectasis and Non-CF bronchiectasis Epidemiology True prevalence is unknown Symptoms often overlap with other respiratory diagnoses Increasing use of CT can show evidence of bronchiectasis when no symptoms are present Often a secondary phenomenon to more serious pulmonary pathology Prevalence increases with age In USA 4.2 per 100,000 18-34 increasing to 271.8 per 100,000 in >75 Little reliable epidemiological data in UK How many patients in Gloucestershire? Causes of bronchiectasis? Structural lung syndromes Toxic injury (inhalation, chronic aspiration, Reflux) Obstruction to a single bronchus (tumour/foreign body) Airways disease (Asthma/COPD/AATD) Mucociliary dysfunction (ciliary dyskinesia, Channelopathies) Allergic Bronchopulmonary Aspergillosis Immunodeficiencies Post infectious Non-tuberculous mycobacterial infection Associated with systemic disease Inflammatory bowel disease Connective tissue disease Idiopathic COPD and Bronchiectasis In 2 studies 29% and 50% of patients diagnosed with chronic bronchitis and COPD had evidence of Bronchiectasis Patients with COPD and bronchiectasis had more severe exacerbations and increased sputum inflammation than those with COPD alone, matched for severity Does COPD cause bronchiectasis or does bronchiectasis cause fixed airflow obstruction? Probably both Is it COPD or is it bronchiectasis? Is it Asthma? Symptoms of bronchiectasis Chronic cough with sputum Recurrent “chest infections” Recurrent “pleurisy” Breathlessness and wheeze Green or yellow sputum in stable clinical state Fatigue When to consider bronchiectasis in adults Productive cough with: Young age at presentation Symptoms over many years Especially if never smoker Daily sputum production Haemoptysis Sputum positive for pseudomonas Unexplained haemoptysis or cough without sputum Patients with particularly troublesome COPD or asthma with frequent exacerbations How to diagnose bronchiectasis Computed Tomography (CT scan) Must be with a high resolution protocol (HRCT) Contrast not necessary Bronchi > accompanying bronchial artery Bronchial wall thickening (harder to define) May help to define aetiology ABPA (proximal), CF, Tracheobronchomegaly Initial assessment to establish cause and severity Routine tests Serum immunoglobulins and protein electrophoresis Sputum examination (state bronchiectasis on form) Spirometry Other tests to consider Total IgE and RAST to Aspergillus If joint problems or systemic symptoms consider Rheumatoid Factor/ANA Sputum for AFB Who should be referred to secondary care Patients with chronic Pseudomonas or Staphylococcus in sputum Deteriorating patients with declining lung function Recurrent exacerbations >3yr Patients requiring prophylactic antibiotics (oral or nebulised) Patients with ABPA, rheumatoid associated bronchiectasis, immunodeficiency, inflammatory bowel disease and primary ciliary dyskinesia Patients with severe advanced disease and those considering lung transplantation Management principles Indentify and treat underlying causes to prevent progression Maintain or improve lung function Improve quality of life by reducing daily symptoms and exacerbations Airway clearance Patients should see a specialist respiratory physiotherapist to be taught airway clearance techniques Active cycle of breathing technique Postural drainage Oscillating positive expiratory devices Forces expiration technique Autogenic drainage Manual techniques during exacerbations Other aids for airway clearance Nebulised normal saline Nebulised hypertonic saline Nebulised bronchodilators Exercise and pulmonary rehabilitation ?mucolytics/inhaled manitol Other drugs Bronchodilators if airflow obstruction present No evidence to support inhaled corticosteroids unless there is concomitant asthma Use lowest dose that controls symptoms Possible link between high dose steroids and nontuberculous mycobacteria No evidence for leukotreine receptor antagonists Antibiotics Sputum samples should always be sent before commencing antibiotics Empirical antibiotics should be started while waiting for results of sputum culture Amoxycillin 500mg tds Clarithromycin 500mg bd Amoxycillin 1g tds or 3g bd if severe bronchiectasis associated with Haemophilus influenzae (Doxycycline 100mg bd for pen allergic) Ciprofloxacin 750mg bd for Pseudomonas Failure to respond should prompt repeat sputum tests IVs should be considered when patients particularly unwell, have resistant organisms or fail to respond to oral therapy Duration of antibiotics 14 days Antibiotics in special situations Combinations of IV antibiotics in those with pseudomonas not responding to oral Ciprofloxacin MRSA treat with 2 oral antibiotics or 1 IV agent If >= 3 exacerbations/yr consider long term antibiotics Macrolides in low dose probably best if tolerated Nebulised antibiotics in pseudomonas and can be used in selected cases due to other pathogens Simple steps in primary care Suspect Bronchiectasis and consider CT scan If positive Check sputum Refer for chest physiotherapy for sputum clearance Review patient with patient management plan Give 14 day course of rescue antibiotics based on last sputum result Consider secondary care referral if Complicated comorbidities or severe disease If pseudomonas or Staphylococcus in sputum Very frequent exacerbations despite adequate antibiotic shoices and duration based on microbiology Organisation of care – the vision Developing a Non CF specialist bronchiectasis service Cross county multidisciplinary service Supported by integrated respiratory nursing team to reinforce self management and rapid access to specialists Easy access to pulmonary rehabilitation and physiotherapy Links to community IV service and ambulatory day unit Supported by regular MDT meetings Pathways developed with clinical immunology and microbiology Supporting a more responsive patient centred approach Case Study Mrs B is a 56 year old with a new diagnosis of bronchiectasis. Diagnosis made by GP following GP organised HRCT Referred to the Bronchiectasis MDT Mrs B was seen by a respiratory specialist physiotherapist who taught airway clearance techniques, gave Mrs B disease education and gave a self management plan Exacerbations managed effectively with patient instigating antibiotic therapy 1 year after diagnosis; exacerbation not responding to treatment Self referral to the Bronchiectasis MDT Sputum specimen sent Antibiotic therapy rationalised accordingly Admission required for IV therapy; arranged as a planned admission through the MDT Completion of IV therapy in the community Ongoing support in the community by MDT nurses and physiotherapists