Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Heart arrhythmia wikipedia , lookup
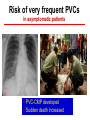
Does asymptomatic patients with very frequent ventricular ectopy need prophylactic catheter ablation to prevent the development of cardiomyopathy Minglong Chen, MD Division of Cardiology The First Affiliated Hospital of Nanjing Medical University Risk of very frequent PVCs in asymptomatic patients PVC-CMP developed Sudden death increased Risk of very frequent PVCs PVC burden ≤20% >20% LVEF 45±1mm 54±1mm CTR 46±1% 52±2% LVEF 73±2% 66±2% MR 0.4±0.1 1.2±0.2 NYHA 1.3±0.1 1.8±0.2 All P < 0.05 Takemoto M, et al. J Am Coll Cardiol, 2005;45:1259–65 Prognostic significance of frequent PVCs with normal LV function • • • • 239 pts with frequent PVCs (>1000 beats/day) Structural heart disease was ruled out, FU period of 5.6 ys no patients exhibited any serious cardiac events. negative correlation between the PVC prevalence and DeltaLVEF (p<0.001) • positive correlation between the PVC prevalence and DeltaLVDd (p<0.001). • PVC prevalence and LVEF at the initial evaluation were independent predicting the development of LV dysfunction (p<0.01) Niwano S, et al. Heart, 2009, 95(15):1230-1237 PVC-CMP more easily attacked in asymptomatic patients The proportion of asymptomatic patients was significantly higher in the presence of cardiomyopathy (36/76, 47%) than in normal LV function (25/165, 15%) Yokokawa M, et al. Heart Rhythm, 2012;9:92–95 Incidence of PVC-CMP • Definition: LVEF of ≤50% in the absence of any detectable underlying heart disease and improvement of LVEF≥15% following effective treatment of index ventricular • Incidence: 6.8% in patients with idiopathic ventricular arrhythmias • Predictors: gender, absence of symptoms, PVC burden, the presence of repetitive monomorphic VT, and so on Hasdemir C, et al. J Cardiovasc Electrophysiol, 2011,22:663-668 Sudden death increased • prospective study,15 637 apparently healthy white men, 35 to 57 ys • prevalence of any VPC was 4.4% (681 of 15,637) • Over FU of 7.5 years, a total of 381 deaths occurred • The presence of any VPC was associated with a significantly higher risk for SCD (adjusted RR=3.0; P < 0.025) • frequent (2 or more uniform VPCs every 2 minutes) or complex (multiforms, pairs, runs, R-on-T) VPCs were at a significantly increased risk of SCD (adjusted RR=4.2; P < 0.005) Abdalla IS, et al. Am J Cardiol, 1987, 60:1036 -1042 Baseline examination from 1987 to 1989, 2-minute rhythm strip of EKG follow-up data collected until December 2002 14,574 subjects,130 incident cases of SCD Participants with VPC were 2 times as likely to have SCD compared to those without VPC (HR2.09, 95% CI1.22 to 3.56) Cheriyath P, et al. Am J Cardiol, 2011, 107:151-155 Cheriyath P, et al. Am J Cardiol, 2011, 107:151-155 Characteristics of PVC-CMP • Enlarged LVDd and CTR, reduced LVEF, increased MR, and deteriorated NYHA functional class • PVC-CMP was resolved within 2 to 4 weeks after discontinuation of PVCs • No inflammation, fibrosis, or changes in apoptosis and mitochondrial oxidative phosphorylation Takemoto M, et al. J Am Coll Cardiol, 2005;45:1259–65 Huizar JF, et al. Circ Arrhythm Electrophysiol, 2011;4:543-549 Huizar JF, et al. Circ Arrhythm Electrophysiol, 2011;4:543-549 Mechanism of PVC-CMP • a short PVC coupling • LV dyssynchrony during PVCs • postextrasystolic potentiation (Which could increase in intracellular Ca2+ and myocardial oxygen consumption) Huizar JF, et al. Circ Arrhythm Electrophysiol, 2011;4:543-549 Determinants of PVC-CMP • • • • • • • PVC burden? QRS width? NSVT? Duration? Symptom or absence of symptom? Gender? …......... ≤20% >20% LVEF 45±1mm 54±1mm CTR 46±1% 52±2% LVEF 73±2% 66±2% MR 0.4±0.1 1.2±0.2 NYHA 1.3±0.1 1.8±0.2 All P < 0.05 PVC burden Takemoto M, et al. J Am Coll Cardiol, 2005;45:1259–65 reduced LVEF (n = 17) vs normal LVEF (n = 53) burden of PVCs: (29.3 ± 14.6% vs 16.7 ± 13.7%, P = 0.004) PVC burden Carpio Munoz, FD, et al. J Cardiovasc Electrophysiol, 2011, 22,791-798 • 57Pts with reduced LVEF(0.37 ±0.10) • 117Pts with normal LVEF • PVC burden:33% ± 13% VS 13 ± 12% PVC burden > 24% was independently associated with PVC-CMP sensitivity :79% , specificity :78%, under curve:0.89 PVC burden Baman TS, et al. Heart Rhythm, 2010;7:865–869 • 17Pts with reduced LVEF • 227Pts with normal LVEF • PVC burden:29% ± 9% VS 8 ± 7% PVC burden > 16% was independently associated with PVC-CMP sensitivity :100% , specificity :87% ,under curve:0.96 Hasdemir C, et al. J Cardiovasc Electrophysiol, 2011,22:663-668 PVC burden QRS duration>150 ms predict PVC-CMP: sensitivity 80%; specificity 52% PVC burden for developing PVC-CMP PVC-QRS width of ≥ 150 ms vs narrower PVC-QRS complex (22% ± 13% vs 28% ± 12%; P<0.0001) QRS duration Yokokawa M, et al. Heart Rhythm, 2012, 9:1460-1464 QRS duration Deyell MW, et al. Heart Rhythm, 2012;9:1465–1472 QRS duration and NSVT Carpio Munoz, FD, et al. J Cardiovasc Electrophysiol, 2011, 22,791-798 . .. Others: male, asymtomatic status Yokokawa M, et al. Heart Rhythm, 2012;9:92–95 Does VPCs ablation reverse LV function? implication of medical therapy • 7 pts with more than 20,000 VPCs in holter (EF:40% or less) received additional cardiac medical therapy, including 4 patients with amiodarone therapy • After medical therapeutic intervention , 75% VPCs or more reduction from baseline in 5 pts • 6±3m FU, EF increased from (27±10)% to 49 +/- 17% in the 5 pts suppression of frequent VPCs may be associated with improvement of left ventricular function Duffee DF, et al. Mayo Clin Proc, 1998, 73(5):430-433 8pts,VPCs 17 541±11 479 per day Before abl:LVEF39%±6%,post abl:62%±6%,P=0.017 Yarlagadda RK, et al. Circulation, 2005, 112:1092-1097 47pts PVCs>10000/d, average 24194±12516/d 38pts RF successfully(GROUP 1), 9 pts unsuccessfully(GROUP 2) GROUP1 Sekiguchi Y, et al. J Cardiovasc Electrophysiol, 2005,16:1057-1063 GROUP2 Plots of BNP levels before and after RFCA in the two groups • 22/60 Pts with reduced EF 34% ± 13% • VPCs burden: 37% ± 13% vs. 11% ± 10% • Patients with reduced EF: before abl vs after abl, 34% ± 13% to 59%±7% • EF remained unchanged in control group Bogun F, et al. Heart Rhythm, 2007;4:863– 867 Controll group ablation group • • • • • 69 pts (51 ± 16 ys) LVEF35% ±9%, LVDD5.8 ± 0.7 cm Frequent outflow tract VPCs (29% ± 13%) 11 ± 6 months FU The magnitude of LVEF improvement correlated with the decline in residual VPD burden (r=0.475, P=.007) Mountantonakis SE, et al. Heart Rhythm, 2011;8:1608 –1614 Predictors of recovery of LV function following the elimination of VPCs Mountantonakis SE, et al. Heart Rhythm, 2011;8:1608 –1614 Deyell MW, et al. Heart Rhythm, 2012;9:1465–1472 Do we need catheter ablation to prevent the development of cardiomyopathy