Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
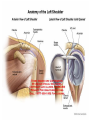
Joints intro A joint is the point where two or more bones meet. There are three main types: Fibrous (immoveable), Cartilagenous (partially moveable) and Synovial (freely moveable) joint. THE JOINTS SYNOVIAL JOINT Cavities between bones in synovial joints are filled with synovial fluid. This fluid helps lubricate and protect the bones. Bursa sacks contain the synovial fluid. The bursitis is the inflammation of the bursa. Characteristics of synovial joints 1. Articular cartilage: This is a smooth, white, shiny mass that covers the articular surfaces of bone. It protects bone tissue and reduces friction (rubbing) between bones when they move. 2. Articular capsule: The articular capsule attaches to the bones near the edge of their articulating surfaces. The capsule is made of strong fibrous tissue and surrounds the joint, adding stability and stopping unwanted material from entering and irritating the joint. The capsule also provides a cavity for synovial fluid to work within. 3. Synovial fluid: yellowish oily fluid that lubricates the articulating surfaces, forms a fluid cushion between surfaces, provides nutrient for cartilage and absorbs debris that is produced by friction between articulating surfaces. 4. Ligaments: These are strong fibrous bands that join articular surfaces, controlling movement and providing stability. 5. Articular discs (meniscus): Some synovial joints such as the knee have menisci. These are made of tough fibrous tissue and their function is to absorb shock and maintain joint stability. They lie between the articulating surfaces and as such protect the surfaces of articulating bone, as seen in the previous image. 6. Bursae: These are found in some synovial joints. They are closed sacs filled with synovial fluid. Their role is to reduce friction that can occur with movement, such as when tendons rub over bones. Types of SYNOVIAL JOINT pivot joint Enables rotation around a lengthwise axis: the cylindrical terminal part of a bone is encased in a hollow cylinder. Examples include the tibia and the fibula. ball-and-socket joint Allows movement along three axes, such as in the shoulder: flexion and extension, rotation, and adduction (arm drawing near the trunk) and abduction (arm drawing away from the trunk). hinge joint Enables flexion and extension along a single axis. The elbow is a particularly good example: the round terminal part of the humerus turns in the hollow of the ulna. condyloid joint An example is the wrist, which the hand can move on two axes: flexion and extension; it can also be tilted sideways (toward the radius and ulna). saddle joint Resembles the condyloid joint but allows a wider range of motion; this type of joint is rare. gliding joint Surfaces of these joints are relatively flat and not very mobile; they allow only a narrow gliding range (e.g., vertebrae, certain bones of the carpus). Shoulder Joint Dr. Nabil Khouri 2015 ARTICULATION Articulation is between: • The rounded head of the humerus and • The shallow, pear-shaped glenoid cavity of the scapula. 10 • The articular surfaces are covered by hyaline cartilage. • The glenoid cavity is deepened by the presence of a fibrocartilaginous rim called the glenoid labrum. 11 Joint Type • Synovial • Ball-and-socket joint 12 Synovial Membrane • It lines the fibrous capsule. • It is attached to the margins of the cartilage covering the articular surfaces. • It forms a tubular sheath around the tendon of the long head of the biceps brachii. • It extends through the anterior wall of the capsule to form the subscapularis bursa beneath the subscapularis muscle. SYNOVIAL MEMBRANE 16 FIBROUS CAPSULE • The fibrous capsule surrounds the joint and is attached: Medially to the margin of the glenoid cavity outside the labrum; Laterally to the anatomic neck of the humerus. 18 • The capsule is thin and lax, allowing a wide range of movement. Ligaments of the shoulder joint Ligamnets of the shoulder 1. The glino humeral legaments: are three weak bands of fibrous tissue that strengthen the front of the capsule. 2. The transverse humeral ligament strengthens the capsule and bridges the gap between the two humeral tuberosities. 3. Coraco humeral ligament : strengthens the capsule from above and stretches from the root of the coracoid process to the greater tuberosity of the humerus. Accessory ligaments: • The coracoacromial ligament extends between the coracoid process and the acromion. Its function is to protect the superior aspect of the joint. LIGAMENTS 21 Shoulder (Anterior View) • • • • The long head of the biceps brachii originates from the supraglenoid tubercle of the scapula, It is intracapsular but extrasynovial It's tendon passes through the shoulder joint and emerges beneath the transverse humeral ligament. Inside the joint, the tendon is surrounded by a separate tubular sheath of the synovial capsule. Movements • Flexion • Extension • Abduction • Adduction • Lateral rotation • Medial rotation Flexion • Normal flexion is about 90° • It is performed by the: 1. 2. 3. 4. Anterior fibers of the deltoid Pectoralis major Biceps brachii Coracobrachialis Extension: • Normal extension is about 45° • It is performed by the: 1. Posterior fibers of the deltoid, 2. Latissimus dorsi 3. Teres major Abduction: • Abduction of the upper limb occurs both at the shoulder joint and between the scapula and the thoracic wall. • It is initiated by supraspinatus from 0 to 18 • Then from 19 to 120 by the middle fibers of the deltoid. • Then above 90 by rotation of the scapula by 2 muscles the Trapezius & Seratos Ant. Adduction: • Normally the upper limb can be swung 45° across the front of the chest. • This is performed by: 1. 2. 3. 4. pectoralis major latissimus dorsi teres major teres minor Lateral rotation: • Normal lateral rotation is about 40 to 45°. • This is performed by the: 1. infraspinatus 2. teres minor 3. the posterior fibers of the deltoid muscle Medial rotation: • Normal medial rotation is about 55°. • This is performed by the: 1. subscapularis 2. latissimus dorsi 3. teres major 4. anterior fibers of the deltoid. Stability of Joint • This joint is unstable because of the: – shallowness of the glenoid fossa – weak ligaments • Its strength almost entirely depends on the tone of the rotator cuff muscles. • The tendons of these muscles are fused to the underlying capsule of the shoulder joint. • The least supported part of the joint lies in the inferior location, where it is 28 unprotected by muscles. Wrist drop • • • A subglenoid displacement of the head of the humerus into the quadrangular space can cause damage to the axillary nerve. This is indicated by paralysis of the deltoid muscle and loss of skin sensation over the lower half of the deltoid. Downward displacement of the humerus can also stretch and damage the radial nerve. 29 ELBOW Joint Synovial Hinge Joint Articulation Trochlea and capitulum of the humerus above Trochlear notch of ulna and the head of radius below ELBOW Joint The articular surfaces are covered with articular (hyaline) cartilage. Capsule Anteriorly: attached Above To the humerus along the upper margins of the coronoid and radial fossae and to the front of the medial and lateral epicondyles. Below To the margin of the coronoid process of the ulna and to the anular ligament, which surrounds the head of the radius. Capsule Posteriorly: attached Above To the margins of the olecranon fossa of the humerus. Below To the upper margin and sides of the olecranon process of the ulna and to the anular ligament. Ligaments Lateral (Radial Collateral) Ligament Triangular in shape: Apex Attached to the lateral epicondyle of humerus Base Attached to the upper margin of annular ligament. Ligaments Medial (Ulnar Collateral) Ligament Anterior strong cord-like band: Between medial epicondyle and the coronoid process of ulna Posterior weaker fan-like band: Between medial epicondyle and the olecranon process of ulna Transverse band: Passes between the anterior and posterior bands Synovial Membrane This lines the capsule and covers fatty pads in the floors of the coronoid, radial, and olecranon fossae. Is continuous below with synovial membrane of the superior radio-ulnar joint Relations Anterior: Brachialis Tendon of Biceps Median nerve Brachial artery Posterior: Triceps muscle Small bursa intervening Lateral: Common extensor tendon The supinator Medial: Ulnar nerve Bursae around the elbow joint: Subcutaneous olecranon bursa Subtendinous olecranon bursa Movements Flexion Is limited by the anterior surfaces of the forearm and arm coming into contact. Extension Is limited by the tension of the anterior ligament and the brachialis muscle. The joint is supplied by branches from the: Median Ulnar Musculocutaneous Radial nerves Carrying Angle Angle Between the long axis of the extended forearm and the long axis of the arm Opens Laterally About 170 degrees in male and 167 degrees in females Disappears When the elbow joint is flexed 1650-1700 Articulations The elbow joint is stable because of the: Wrench-shaped articular surface of the olecranon and the pulley-shaped trochlea of the humerus Strong medial and lateral ligaments. Elbow dislocations are common & most are posterior. Posterior dislocation usually follows falling on the outstretched hand. Posterior dislocations of the joint are common in children because the parts of the bones that stabilize the joint are incompletely developed. ELBOW Joint Avulsion of the epiphysis of the medial epicondyle is also common in childhood CUBITAL FOSSA Cubital fossa showing boundaries 44 • The roof of the cubital fossa is formed by superficial fascia and skin. • The most important structure within the roof is the median cubital vein, which passes diagonally across the roof and connects the cephalic vein on the lateral side of the upper limb with the basilic vein on the medial side. • The bicipital aponeurosis separates the median cubital vein from the brachial artery and median nerve. • Other structures within the roof are cutaneous nervesthe medial cutaneous and lateral cutaneous nerves of the forearm. 47 4/29/2017 Superficially, in the subcutaneous tissue overlying the fossa median cubital vein, medial and lateral antebrachial cutaneous nerves basilic and cephalic veins. 48 CONTENTS OF CUBITAL FOSSA The major contents of the cubital fossa, from lateral to medial, are: • The tendon of the biceps brachii muscle; • The terminal part of brachial artery; • The median nerve. 50 1) Terminal part of the brachial artery,radial and ulnar arteries 2) Biceps brachii tendon 3) Median nerve 4) Radial nerve 5) (Deep) accompanying veins of the arteries Position of the radial nerve • The median nerve lies immediately medial to the brachial artery and leaves the fossa by passing between the ulnar and humeral heads of the pronator teres muscle. • The brachial artery and the median nerve are covered and protected anteriorly in the distal part of the cubital fossa by the bicipital aponeurosis. • This flat connective tissue membrane passes between the medial side of the tendon of the biceps brachii muscle and deep fascia of the forearm. • The sharp medial margin of the bicipital aponeurosis can often be felt. median nerve lies immediately medial to the brachial artery and leaves the fossa by passing between the ulnar and humeral heads of the pronator teres muscle. radial nerve lies under brachioradialis (lateral margin of the fossa) gives off deep branch of the radial nerve and continues as superficial radial nerve. • The brachial artery normally bifurcates into the radial and ulnar arteries in the apex of the fossa, although this bifurcation may occur much higher in the arm, even in the axilla. • When taking a blood pressure reading from a patient, the clinician places the stethoscope over the brachial artery in the cubital fossa.