Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
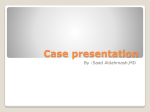
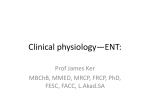
992 INVESTIGATIVE OPHTHALMOLOGY b VISUAL SCIENCE / August 1984 VI, Duke-Elder S, editor. St. Louis, CV Mosby Co., 1973, p. 176. 3. Kaufman PL and Davis GE: "Minified" Goldmann applanating prism for tonometry in monkeys and humans. Arch Ophthalmol 98:542, 1980. 4. Moses RA: Repeated applanation tonometry. Ophthalmologica 142:663, 1961. 5. Moses RA, Lurie P, and Grodzi WJ Jr: Antero-posterior forces Vol. 25 on the human eyeball. In Basic Aspects of Glaucoma Research, Liitjen-Drecoll E, editor. International Symposium, Department of Anatomy, University Erlangen-Niirnberg, September 17-18, 1981. Stuttgart-NY, FK Schattauer, Verlag, 1982, pp. 199-208. 6. Kraukau CET and Wilke K: On repeated tonometry. Acta Ophthalmologica 49:611, 1971. 7. Kraukau CET: A vibration tonometer. Ophthalmic Res 1:129, 1970. Decrease of Anterior Ciliary Arterial Pressure with Increased Ocular Pressure Go Sakimoro ond Bernard Schwartz The relationship of the ocular pressure to the anterior ciliary arterial pressure was studied by measuring the pressure of the anterior ciliary artery using a modified pressure chamber. Of the 40 subjects, 9 were normal, 16 were ocular hypertensive patients, and 15 were primary, open-angle, glaucoma patients. A significant negative correlation was found between the anterior ciliary arterial pressure and the ocular pressure such that the former decreases as the latter increases. These results support the concept that the blood flow in the anterior ciliary artery is from the inside of the eye to the outside. Invest Ophthalmol Vis Sci 25:992-995, 1984 In order to further investigate our previous finding that blood flowed from the inside of the eye to the outside in the anterior ciliary arteries,1 we examined the circulatory dynamics by measuring the pressure of the anterior ciliary artery in normal, ocular hypertensive, and glaucomatous subjects and determined the correlations between pressures in this vessel and ocular pressures. Materials and Methods. Subjects: As defined previously,2 the study was comprised of normal subjects, ocular hypertensive and open-angle glaucoma patients attending the Outpatient Ophthalmology Service of the Tufts-New England Medical Center (Boston, Massachusetts). Informed consent was obtained from all subjects. None of the normal subjects or ocular hypertensive patients were taking ocular medications. All of the glaucoma patients were receiving antiglaucoma medication. The pressure chamber method was used for the measurement of the anterior ciliary arterial pressure.2 A transparent plastic film (Saran Wrap) was used on the tip of the pressure chamber for measurement of the anterior ciliary arterial pressure, and a transparent latex membrane (Tonofilm) was used for the measurement of the episcleral venous pressure. First, ocular pressure and brachial blood pressure were measured with the patient seated. The Goldmann applanation tonometer was used for ocular pressure, and brachial blood pressure was measured in the standard fashion by sphygmomanometer. For the subsequent measurement of episcleral vein and anterior ciliary arterial pressures, the subject's eye was anesthetized topically with 0.5% proparacaine and the subject was seated before the slit lamp. The anterior ciliary arteries were distinguished from the episcleral veins by wider caliber, more tortuous course, and slightly brighter color.2 The episcleral venous pressure was measured before the anterior ciliary arterial pressure, using the total collapse of the veins as the end point. The measurement was made on an episcleral vein at a point approximately 5 mM from the limbus in the temporal quadrant; the right eyes of 35 patients and the left eyes of four patients were measured. The diastolic arterial pressure was recorded as the first point at which some portion of the anterior ciliary artery showed pulsation. The pressure then was increased and the systolic arterial pressure was recorded as the point at which the artery collapsed totally. Pressure measurements were made on the anterior ciliary artery in the temporal and nasal quadrants approximately 5 mM from the limbus, in the right eye of 36 subjects and in the left eyes of four subjects. Only one eye was measured in each subject. Ocular pressure was measured by one observer and anterior ciliary arterial and episcleral venous pressure by a second; each was masked to the measurements made by the other. Pressures for the episcleral veins and the anterior ciliary arteries were recorded as the average of three consecutive measurements. The median coefficients of variation (SD/mean X percent) and, in parentheses, the 30th and 70th percentiles for the reproducibility of each of the sets of pressure measurements were: nasal systolic 5.4 (3.6, 6.6); nasal diastolic 7.5 (5.8, 11.7); temporal systolic 6.6 (5.6, 8.4); temporal diastolic 7.9 (5.1, 11.3); and episcleral venous pressure 7.6 (6.0, 11.1). Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933348/ on 05/11/2017 993 Reports No. 8 Table 1. Systemic and ocular characteristics Percentiles Median (30th, 70th) Age Ocular pressure (mmHg) Episcleral venous pressure (mmHg) Brachial blood pressure (mmHg) Systolic Diastolic 66 (58, 73) 17.8 (15.9,23.8) 9 .5* (8.3,* 10.6*) (126, 145) (67, 77) 133 72 Ocular hypertensives (n = 16) Normals (n = 9) All subjects (n = 40) 75 (70, 79) 61 15.8: (14.5, 17.0) 23.8(18.2, 25.4) 17.0(16.2, 24.5) 9.4 (8.0, 10.3) 9.0(8.2, 10.4) 10.5,f(9.3,t 11.2f) 140 73 129 71 (127, 150) (67, 78) * Based on 39 eyes. (55,68) Open-angle glaucomas (n = 15) (122, 140) (70,76) 65 140 76 (60, 75) (128, 151) (70, 83) t Based on 8 eyes. Nonparametric statistical tests were used for analysis. A stepwise regression analysis3 was used to determine whether multivariable relationships exist between the episcleral arterial pressures and various systemic and ocular characteristics. The levels of significance were 0.05 for the two-tailed t-tests and 0.01 for the correlation and regression analyses. Results. The systemic and ocular characteristics of all subjects are described in Table 1. The percentiles of the anterior ciliary arterial pressure in all subjects and for each diagnostic group are shown in Table 2. Within the total population, no significant correlation coefficients were found between the anterior ciliary arterial pressures, episcleral venous pressures, and systolic and diastolic blood pressures and age. Also, no significant correlations were observed between systolic and diastolic blood pressures and systolic and diastolic anterior ciliary arterial pressures. No significant differences were found between men and women for temporal or nasal diastolic and systolic pressures. Comparison of the nasal with the temporal arteries in the same eye using the Wilcoxin Signed Rank test revealed that the pressures in the nasal vessels were significantly higher than in the temporal vessels for both systolic (P = 0.001) and diastolic (P = 0.034) pressures. Thus, for further analyses the nasal and temporal arteries were considered separately. Using the Mann-Whitney U-test, significant differences between the diagnostic groups were discovered for the frequency distributions of the anterior ciliary arterial pressures between the normal and the ocular hypertensive groups (nasal systolic P = 0.016; temporal systolic P = 0.009; nasal diastolic P = 0.025; temporal diastolic P = 0.041). However, no significant differences were found between normals and glaucomas nor between glaucomas and ocular hypertensives. Statistically significant negative Spearman correlations (rs) were found between the anterior ciliary arterial pressures and the ocular pressures (nasal systolic rs = -0.6102, P< 0.0001; temporal systolic r s = -0.6595, P < 0.0001; nasal diastolic rs = -0.5454, P = 0.0003; temporal diastolic rs = 0.45 \l,P = 0.0035), indicating that the higher the ocular pressure, the lower the anterior ciliary arterial pressure (Figs. 1, 2). Both linear and nonlinear regression models were generated to describe the relationship between the anterior ciliary arterial pressures and ocular pressure. The nonlinear models were found to provide a better fit of the data (Figs. 1, 2). Significant positive Spearman correlations (rs) were found for the anterior ciliary arterial pressures with the episcleral venous pressures, indicating the higher the anterior ciliary arterial pressure, the higher the episcleral venous pressure (nasal systolic rs = 0.4568, Table 2. Anterior ciliary arterial pressures (mmHg) Percentiles Median (30th, 70th) All subjects (n = 40) Nasal systolic Temporal systolic Nasal diastolic Temporal diastolic * Based on 39 eyes. 51* 51 36* 33 (45,* 63*) (44,57) (29,* 41*) (29, 40) Normals (n = 9) 62 57 41 37 (59, 67) (56, 59) (39, 47) (31,43) Ocular hypertensives (n = 16) 48 45 30 30 (43, (38, (27, (26, 58) 49) 37) 35) t Based on 14 eyes. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933348/ on 05/11/2017 Open-angle glaucomas (n = 15) 51f(44,t 66f) 50 (43, 56) 34f (28,t 42f) 32 (28, 40) 994 INVESTIGATIVE OPHTHALMOLOGY 6 VISUAL SCIENCE / Augusr 1984 I00 < ACAP=84.8le- a 0 2 6 I 0 P < rs = -0.6595 p = < 0.0001 n =40 so 0) "</> 60 II j 40h 10 20 30 40 Ocular Pressure (IOP, mm Hg) Fig. 1. Relationship between ocular pressure and temporal systolic anterior ciliary arterial pressure with nonlinear model. ACAP (anterior ciliary arterial pressure) = 84.81e" 0026IOP (intraocular pressure). P = 0.0039; temporal systolic rs = 0.5798, P < 0.0001; nasal diastolic rs = 0.3806, P = 0.0184; temporal diastolic rs = 0.4718, P = 0.0024). The ocular pressure was also significantly negatively correlated with the episcleral venous pressure (rs = -0.5573, P = 0.0002). A stepwise regression analysis was done with the temporal systolic, temporal diastolic, nasal systolic, and nasal diastolic pressures of the episcleral arteries considered separately as dependent variables and the potential independent variables of age, ocular pressure, 80 ACAP=53.82e-°- 023l0P a. o si rs =-0.4511 p = 0.0035 n = 40 60 a> t .2 o 40 o f— 10 20 30 40 Ocular Pressure (IOP, mm Hg) Fig. 2. Relationship between ocular pressure and temporal diastolic anterior ciliary arterial pressure with nonlinear model. ACAP (anterior ciliary arterial pressure) = 53.82e"002:ilOP (intraocular pressure). Vol. 25 episcleral venous pressure, and systolic and diastolic blood pressures. The logarithms of the temporal systolic and diastolic pressures were used for this analysis since the distributions of these variables showed marked skewness and kurtosis. The only independent variable that showed a significant relationship with each of the dependent variables was ocular pressure (P< 0.001). Discussion. A highly significant negative correlation was found between the anterior ciliary arterial pressures and the ocular pressures, indicating the higher the ocular pressure, the lower the anterior ciliary arterial pressure. To our knowledge, this negative correlation has not been described previously; however, Weigelin and Lohlein4 reported no correlation between both pressures. In their study, the range of ocular pressure was probably not large enough to determine a relationship (7-24 mmHg). Using model equations (Figs. 1, 2) the degree of change of anterior ciliary arterial pressures with ocular pressure can be calculated. An increase in ocular pressure from 10 mmHg to 40 mmHg results in about a 50% decrease in diastolic and systolic arterial pressures. There were significant differences in anterior ciliary arterial pressures between normals and ocular hypertensives but not between normals and open-angle glaucomas. Since the glaucomas were being treated, this finding probably resulted from the closer similarity of the ocular pressures of normal and glaucomatous individuals (Table 1). We found no significant relationship between anterior ciliary arterial pressures and brachial blood pressures with either Spearman correlation or multiple regression analysis. However, Weigelin and Lohlein4 and Sayegh et al5 observed what they considered to be a significant correlation between episcleral arterial pressure and brachial blood pressure. The differences between our results and theirs may be explained by the larger range of ocular pressures among our subjects. Since we have shown a highly significant decrease in anterior ciliary arterial pressures with increasing ocular pressures, this factor would tend to lower anterior ciliary arterial pressures and, therefore, negate any correlation with brachial blood pressures. The lack of correlation of anterior ciliary arterial pressures with brachial blood pressure may be the result of the dominant influence of the ocular pressure, not blood pressure, in controlling the correlation. Within limits, the eye can be viewed as a closed system with local pressure determinants overriding systemic ones. The absence of a significant correlation between episcleral venous pressure and blood pressure as well as the negative correlation between ocular pressure and episcleral venous pressure confirm our finding in an independent sample of subjects.2 Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933348/ on 05/11/2017 No. 8 995 Reporrs The decrease of episcleral arterial pressure with increased ocular pressure may be the result of decreased flow of blood in the episcleral arteries. On the basis of our previous fluorescein angiographic studies of the anterior ciliary arteries,1 we postulated that the blood flow is from the inside of the eye to the outside. Thus, with increased ocular pressure there may be a decrease in the flow in the iris and choroid,6 with a resultant decrease in flow of blood into the episcleral arterial system. However, other explanations are possible. With an increase in ocular pressure, the episcleral arteries could dilate with a resultant decrease in pressure; or a shunting of blood away from the episcleral arterial system could occur with a resulting decrease in episcleral arterial pressure. Finally, it has been known for some time that the anterior ciliary arteries provide the blood supply to the drainage area of the anterior chamber, including the canal of Schlemm.7"9 As far as we are aware, there is only one published study of changes in the blood supply to this area in glaucomatous eyes.10 Our observations suggest that increased ocular pressure decreases anterior ciliary arterial pressure and thus may decrease blood flow in these arteries, which supply blood to the drainage area of the anterior chamber, including Schlemm's canal. Therefore, a decrease in nutrition of this area may be a pathogenic factor, impeding aqueous humor drainage in glaucoma. Key words: anterior ciliary arterial pressure, episcleral venous pressure, ocular hypertension, open-angle glaucoma From the Department of Ophthalmology, New England Medical Center, and Tufts University School of Medicine, Boston, Massachusetts. The work for this study was done while Dr. Sakimoto was a Glaucoma Fellow at New England Medical Center. He is now at the Department of Ophthalmology, Kagoshima University Faculty of Medicine, Usukicho, 1208-1, Kagoshima-shi 890, Japan. Supported by grants from the Massachusetts Lions Eye Research Fund, Inc., and from Research to Prevent Blindness, Inc., New York, New York, and by grant RO1-EY04905 from the National Institutes of Health, Bethesda, Maryland. Read in part before the annual meeting of the Association for Research in Vision and Ophthalmology, Sarasota, Florida, April 27, 1981. Submitted for publication: March 7, 1983. Reprint requests: Bernard Schwartz, MD, PhD, Department of Ophthalmology, New England Medical Center, 171 Harrison Avenue, Boston, Massachusetts 02111. References 1. Talusan ED and Schwartz B: Fluorescein angiography: Demonstration of the flow pattern of anterior ciliary arteries. Arch Ophthalmol 99:1074, 1981. 2. Talusan ED and Schwartz B: Episcleral venous pressure: Differences between normals, ocular hypertensives and primary open angle glaucomas. Arch Ophthalmol 99:824, 1981. 3. KJeinbaum DG and Kupper TT: Applied Regression Analysis and Other Multivariable Methods. North Scituate, MA, Duxbury Press, 1978, pp. 37-59; 131; 231-232. 4. Weigelin E and Lohlein H: Blutdruckmessungen an den episkleralen Gefassendes des Auges bei Kreislaufgesunden Personen. Albrecht von Graefes Arch fur Ophthalmol 153:202, 1952. 5. Sayegh F, Azmoun A, and Weigelin E: Critical comparison of vasotonometric (Rethy) and ophthalmodynamometric measurements. Ophthalmic Res 5:300, 1973. 6. Bill A: Capillary permeability to and extravascular dynamics of myoglobin, albumin and gamma globulin in the uvea. Acta Physiol Scand 73:204, 1968. 7. Ashton N and Smith R: Anatomical study of Schlemm's canal and aqueous veins by means of neoprene casts. III. Arterial relations of Schlemm's canal. Br J Ophthalmol 37:577, 1953. 8. Dvorak-Theobald G: Further studies on the canal of Schlemm. Its anastomoses and anatomic relations. Am J Ophthalmol 39:65, 1955. 9. Jocson VL and Grant WM: Interconnections of blood vessels and aqueous vessels in human eyes. Arch Ophthalmol 73:707, 1965. 10. Friedenwald JS: Circulation of the aqueous. V. Mechanism of Schlemm's canal. Arch Ophthalmol 16:65, 1936. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933348/ on 05/11/2017