Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiac surgery wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Myocardial infarction wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
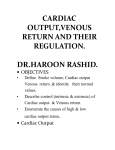
1210 Dobutamine Increases Cardiac Output of the Total Artificial Heart Implications for Vascular Contribution of Inotropic Agents to Augmented Ventricular Function Philip F. Binkley, MD; Kevin D. Murray, MD; Kim M. Watson, BS; P. David Myerowitz, MD; and Carl V. Leier, MD Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 Background. The synthetic catecholamine dobutamine increases stroke volume in normal subjects and in patients with congestive heart failure. In addition to its direct influence on myocardial contractility, dobutamine may significantly modulate vascular tone because of its a' and ,B-adrenergic agonist activity. Methods and Results. To test the hypothesis that such vasoactive properties significantly contribute to the improved ventricular performance noted with this agent, hemodynamic parameters were measured during stepped ascension infusion of dobutamine in a model that is insensitive to positive inotropic stimulation. Administration of dobutamine in nine calves that underwent replacement of the native right and left ventricles with pneumatically driven total artificial hearts resulted in a significant (p=0.0001) increase in cardiac output from 7.0±+1.8 to 8.2±1.8 1/min and a significant (p=0.0001) decrease in total peripheral vascular resistance from 1,224± 559 to 745 ±317 dyne-sec/cm5. A less marked influence was noted on the pulmonary vasculature, with pulmonary vascular resistance exhibiting a significant (p<O.OS) decrease from its baseline value only at the peak infusion. Consistent with an increase in venous return, both left and right atrial pressures increased significantly (p<0.005) with dobutamine administration. Conclusions. These data demonstrate that the vasoactive properties of dobutamine significantly contribute to improved ventricular performance independent of direct myocardial stimulation. This effect appears to result in part from a direct modulation of arterial and venous tones rather than from a reflex response to primary changes in contractility. (Circulation 1991;84:1210-1215) obutamine is a synthetic catecholamine that is known to increase cardiac output in normal subjects and in patients with congestive heart failure.'-3 Although this effect is attributed in large part to direct stimulation of the myocardium and consequent increases in ventricular contractility, dobutamine may influence the arterial and venous vasculature because of a- and ,B-adrenergic agonist activity.3-10 Dobutamine exists as a racemic mixture of two stereoisomers in which the D From the Divisions of Cardiology and Thoracic Surgery, The Ohio State University Hospital, Columbus, Ohio. Supported by a Grant-in-Aid from the American Heart Association, Central Ohio Affiliate, and Eli Lilly and Co., Indianapolis, Ind. P.F.B. is the recipient of a Clinical Associate Physician Award from the National Institutes of Health. Address for reprints: Philip F. Binkley, MD, The Ohio State University Hospital, Division of Cardiology, 1654 Upham Drive, 627 Means Hall, Columbus, OH 43210. Received December 12, 1989; revision accepted April 9, 1991. a-adrenergic activity is found to reside in the levo isomer and 13-adrenergic activity is expressed by the dextro isomer.'0 Varying degrees of peripheral vasodilation have been reported that have been ascribed to either direct or reflex effects on the vasculature, but the mechanism of this vascular response remains incompletely described.6-9 The present investigation used a model that is insensitive to the positive inotropic influence of dobutamine to test the hypothesis that the vasoactive properties of this agent significantly contribute to improved ventricular performance. The results indicate that dobutamine is associated with a significant reduction of systemic vascular resistance coincident with a significant increase in cardiac output that appears to be independent of its effects on myocardial contractility and may be ascribed to its direct effects on the vasculature. Methods All investigations and procedures were reviewed and approved by the animal use committee of the Binkley et al Augmented Function of Artificial Heart Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 Ohio State University. The model consisted of nine calves that underwent replacement of the native right and left ventricles with pneumatically driven total artificial right and left ventricles (Jarvik 7, Symbion, Inc., Salt Lake City, or Utah 100, University of Utah, Salt Lake City). The procedure for implantation of the artificial ventricles has been previously described.11-'3 Briefly, general anesthesia was maintained with halothane after pentobarbital induction and endotracheal intubation. A right lateral thoracotomy was performed, and the animal was placed on cardiopulmonary bypass. The native right and left ventricles were excised along the atrioventricular valve rings and above the semilunar valves. Atrial quick-connect cuffs were sewn into the right and left atria, and vascular grafts were anastomosed to the pulmonary artery and aorta. The artificial right and left ventricles were then positioned and secured using the respective atrial quick-connect cuffs and vascular grafts. The right and left ventricles were connected via drive line tubing to the respective pneumatic chambers of the heart driver. Control parameters for each ventricle consisted of heart rate, drive pressure, and percent time in systole. With activation of the artificial ventricles, the animal was weaned from total cardiopulmonary bypass. Device parameters were adjusted to maintain physiological pressures and ensure adequate cardiac output. The wound was closed with running sutures, and drainage tubes were inserted in the pleural space. The animal was transported to a specially constructed cage that optimized animal mobility while ensuring the integrity of the drive line connection to the heart driver. All animals were extubated and pleural drainage tubes were removed within 24 to 48 hours. A 4-day recovery period preceded the study protocol. All drug infusions were performed with the animal in the sternal recumbent posture. Aortic, pulmonary arterial, and left and right atrial pressures and cardiac outputs were monitored for a total of 20 minutes to ensure hemodynamic equilibration, which was defined as less than 10% variation in any of these parameters. Device parameters were adjusted so that the artificial ventricles were not completely filling at baseline. Specifically, heart rate for the nine animals ranged from 100 to 120 beats/min (mean+SD, 109 +7 beats/min), and percent time in systole ranged from 44% to 50% (mean+SD, 47+3%). Right ventricular drive pressures ranged from 75 to 120 mm Hg (mean±SD, 103 + 17 mm Hg), and left ventricular drive pressures ranged from 235 to 285 mm Hg (mean+SD, 262+16 mm Hg). These initial device parameters were maintained constant throughout the subsequent dobutamine infusions. Cardiac outputs were measured using the cardiac output monitoring and diagnostic unit (COMDU, Symbion) of the heart driver. This device integrates diastolic exhaust air flow and applies a volume conversion factor to calculate stroke volume on a beat-by-beat basis. Validation of this technique has been performed by com- 1211 parison with simultaneously measured cardiac outputs using turbine flowmeters.14 After establishing hemodynamic equilibration, dobutamine was administered for three consecutive 10-minute infusions at rates of 6,12, and 24 jig/kg/ min using a percutaneously inserted external jugular line. Minute averages of cardiac output were printed continuously by the COMDU, and atrial, pulmonary arterial, and aortic pressures were recorded at the peak of each infusion. After measurements were acquired at peak dosing, the infusion was discontinued, and the animal was allowed to return to baseline hemodynamic status. Derived Hemodynamic Parameters and Statistical Analysis Cardiac output was averaged during the last 5 minutes of the baseline period and of each infusion period and was used for assessment of dobutamine effects on stroke volume. Total peripheral vascular resistance (dyne.sec/cm5) was calculated as mean systemic pressure (mm Hg) multiplied by 80 and then divided by cardiac output (1/min). Similarly, total pulmonary vascular resistance was calculated according to the same formula using mean pulmonary artery pressure and cardiac output. Analysis of variance for repeated measures was used to test for significant changes in hemodynamic parameters associated with dobutamine administration. Posttest comparisons were performed to identify specific points that differed significantly from baseline. Statistical significance was defined as a probability of less than 0.05. Results Systemic Vascular Response Cardiac output was noted to increase in each of the nine calves beginning with the first infusion rate. For the group as a whole, the mean cardiac output of 7.0±1.8 1/min significantly (p = 0.0001) increased over the range of dosages tested, attaining a peak value of 8.2±1.8 1/min at the 24-,mg/kg/min infusion rate (Figure 1A). Posttest comparison of values indicated that all infusion rates were associated with cardiac outputs significantly greater than baseline. Coincident with the increase in cardiac output, total peripheral vascular resistance significantly (p=0.0001) decreased from the baseline value of 1,224±559 dyne.sec/cm5 with each of the three infusion rates, with the lowest value of 745 ±317 dyne-sec/cm5 noted at the 24-,g/kg/min infusion (Figure 1B). This response was accompanied by a significant (p=0.001) decrease in mean aortic pressure from 98±32 to 70±14 mm Hg at the peak infusion rate (Figure 1C). Pulmonary Vascular Response In contrast to the effect noted in the systemic vasculature, less marked decreases in pulmonary vascular resistance were observed (Figure 2). The baseline value of 367±313 dyne-sec/cm' significantly (p<0.05) decreased to a value of 280±261 dyne.sec/ 1212 Circulation Vol 84, No 3 September 1991 * 9.5a I- * = ANOVA E 610 560 CD 510- p<.0001 8.5_ CL 460 410360 310 - sr 0 CL U cc cr = ANOVA pc.05 660 us 7.5- 4 cc 4 260, baseline 6.5 6 12 24 1700 ^ E E 1500- cn 1300 c U) 1100- :900z 4c 700- baseline 6 1 2 2 4 Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 INFUSION RATE--MCGIKG/MIN FIGURE 2. Plots of changes in pulmonary vascular hemodynamics with dobutamine administration. Panel A: Significant decrease in pulmonary vascular resistance (PVR) noted with peak dobutamine infusion rate only. Panel B: No change in mean pulmonary artery (PA) pressure observed with dobutamine administration. I E E 125 0) cc 115 60 105 u, r: 85 0 75 W 65 baseline 6 1 2 2 4 INFUSION RATE--MCG/K/GMIN FIGURE 1. Panel A: Plot of mean and standard deviation of cardiac output for nine calves with total artificial hearts at baseline and with dobutamine administered at 6, 12, and 24 pg/kg/min i.v. A significant increase in cardiac output is noted compared with baseline with each dobutamine infusion rate. Panel B: Plot of significant decrease in mean and standard deviation total peripheral vascular resistance (TPR) with dobutamine administration. A significant decrease is noted with low- as well as high-dose infusion. Panel C: Plot of significant decline in mean aortic pressure with dobutamine infusion. exhibited a moderate but statistically significant (p =0.004) increase from 9±4 to 13±3 mm Hg. To test the specific role of the a- and fl-agonist properties of dobutamine in mediating the observed circulatory response, selective pharmacological stimulation of the vasculature was performed in a subset of the experimental animals. The influence of a-adren- pressure * =ANOVA Pc.005 m E E 0 z 0 eh p CL noted at peak infusion. Smaller decreases in pulmonary vascular resistance were noted at intermediate infusion rates, and posttest comparisons demonstrated that only the value at peak infusion differed significantly from baseline. No significant change in the baseline mean pulmonary artery pressure of 24±7 mm Hg was noted with dobutamine administration (Figure 2B). cm5 Right and Left Ventricular Filling Pressures Both left and right atrial pressures increased with dobutamine infusion (Figure 3). A progressive and significant (p=0.0004) increase in left atrial pressure was noted with the baseline value of 13±5 mm Hg increasing to 18+7 mm Hg with peak infusion and with left atrial pressure significantly greater than baseline with each infusion rate. Similarly, right atrial 0 z 41 I E 17 0 13 CLi 13 - 11X m 9 . baseline 6 1 2 24 INFUSION RATE--MCG/KGIMIN FIGURE 3. Plots of changes in left (panel A) and right (panel B) atrial pressures with dobutamine. A significant increase in right atrialpressure is noted with peak infusion and in left atrial pressure at all infusion rates. Binkley et al Augmented Function of Artificial Heart Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 ergic stimulation was established in one cow using a 1-mg i.v. bolus of phenylephrine, which resulted in an increase in cardiac output from 9.6 to 11.1 1/min despite increases in mean systemic pressure from 113 to 149 mm Hg and in total peripheral resistance from 942 to 1,074 dyne.sec/cm5. Having characterized the influence of a-agonist stimulation on circulatory function in this model, the a-adrenergic properties of dobutamine were isolated by ,B-blockade using 20 mg propranolol administered intravenously in the same cow before infusion of dobutamine. Dobutamine infusion after this pretreatment with propranolol resulted in an increase in cardiac output from 8.7 to 10.1 1/min with an increase in mean blood pressure from 112 to 131 mm Hg. The specific influence of the a-adrenergic properties of dobutamine were further examined in two different cows by infusion of the levo isomer of dobutamine (Eli Lilly and Co., Indianapolis, Ind.) in which reside the a-agonist properties of racemic dobutamine.10 In these two cows, infusion of the levo stereoisomer of dobutamine resulted in increases in cardiac output from 7.9±1.0 to 10.0±1.1 1/min, in mean systemic pressure from 77±4 to 148 ±3 mm Hg, in total peripheral resistance from 788±138 to 1,186±122 dyne.sec/cm5, in left atrial pressure from 14±7 to 28±1 mm Hg, and in right atrial pressure from 7±7 to 11±8 mm Hg. The influence of p-adrenergic stimulation in this model was characterized in two cows in which isoproterenol was infused. Isoproterenol infusion resulted in an increase in cardiac output from 7.0±0.1 to 8.3±0.2 1/min, a decrease in systemic vascular resistance from 1.132+6 to 609±23 dyne.sec/cm5, and an increase in right and left atrial pressures of 50%. The influence of the p-adrenergic stimulating properties of dobutamine was then tested in two different cows by infusion of the dextro isomer of dobutamine, which imparts the p-agonist properties of racemic dobutamine.'0 Infusion of the dextro isomer resulted in an increase in cardiac output from 6.7±0.8 to 8.3±1.1 1/min, a decrease in systemic vascular resistance from 845±262 to 611±96 dyne.sec/cm5, and an increase in atrial pressures equal to those seen with isoproterenol. Discussion The present investigation demonstrates that in addition to its positive inotropic properties, the vascular effects of dobutamine significantly contribute to the enhanced cardiac output that results from its administration. Dobutamine infusion resulted in significant increases in cardiac output despite the absence of any change in the drive parameters of the artificial heart, indicating that the changes in cardiac output must be solely ascribed to the influence of dobutamine on the vasculature. This vasoactive augmentation of cardiac output appears to consist of a reduction in ventricular afterload and potentially an increase in venous return mediated by a reduction of venous capacitance. The model used in the present investigation is uniquely suited to the analysis of mechanisms of 1213 vascular control. Because the total artificial heart is devoid of any sensitivity to positive inotropic stimulus, the model may be viewed as one in which the vascular response to a given perturbation may be isolated from any coincident influence on myocardial contractility. Observed vascular responses must therefore be ascribed to the direct influence of an intervention on the vasculature rather than to reflex mechanisms arising from primary changes in myocardial contractility. Although the innate "contractility" of the artificial heart is fixed once the initial functional parameters of the device have been set, the performance of the artificial ventricle is sensitive to preload and afterload, and its function may be modified by alterations in loading conditions. This has been demonstrated in animal models at rest, during exercise, and in response to various pharmacological interventions.15-19 Thus, given the properties of this model, the vascular determinants of ventricular and overall circulatory performance may be segregated and analyzed. Finally, this is an otherwise physiological model in that the animals are not anesthetized and are alert and active in a manner resembling the preoperative state. That dobutamine may directly or indirectly modulate systemic vascular resistance has been noted in prior investigations in human subjects and animal models.4-9 However, none of these has completely eliminated the direct positive inotropic effects of dobutamine on the myocardium and the possible attendant secondary vascular responses. Varying reductions in systemic vascular resistance have been described and attributed to either direct p2-adrenergic stimulation of peripheral resistance vessels or to reflex mechanisms. Using a canine model, Liang and Hood6 reported that lower-dose infusions of dobutamine resulted in reductions in peripheral vascular resistance that could be prevented by ganglionic blockade.6 However, at higher doses, reductions in vascular resistance could be prevented by p-adrenergic but not ganglionic blockade. It was concluded that lower-dose infusions of dobutamine indirectly mediated vasodilation because of baroreceptor activation resulting from enhanced ventricular contractility and consequent increase in pulse pressure. In the present investigation, significant reductions in total peripheral vascular resistance were observed at low as well as high infusion rates. In this model, which is insensitive to positive inotropic stimulation, augmented contractility and subsequent increases in pulse pressure would not be primary events initiating reflex vasodilation. It would appear that in this context, even low-dose infusion of dobutamine would bring about vasodilation via direct p2-adrenergic stimulation of peripheral resistance vessels. In addition to its influence on the systemic arterial vasculature, dobutamine may also modulate venous capacitance and, consequently, venous return. Both aand p-adrenergic stimulations have been shown to reduce venous capacitance in a variety of models.20-23 Because dobutamine possesses a- and p-adrenergic 1214 Circulation Vol 84, No 3 September 1991 Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 agonist activities, it may augment venous return by stimulation of both of these receptor systems. Consistent with this hypothesis, Fuchs et al23 demonstrated a decrease in venous capacitance accompanying dobutamine infusion as measured by splanchnic volume and found that this decrease could be prevented by a-blockade. Thus, both afterload reduction (via /2agonist effects) and augmentation of venous return (resulting from a- and /3-agonist activities) may contribute to the increase in cardiac output mediated by dobutamine's influence on the vasculature. The subset of cows in which the responses to specific a- and ,B-adrenergic stimulations were examined further substantiates these mechanisms. a-Adrenergic stimulation with phenylephrine resulted in an increase in cardiac output similar in magnitude to that observed with dobutamine infusion. This occurred despite marked increases in systemic arterial pressure and systemic vascular resistance. Because the pneumatically driven artificial heart operates at a driving pressure greater than even the peak systemic pressure achieved with phenylephrine, it will continue to eject the volume of blood returned by the venous circulation despite such elevations in afterload. As such, the artificial ventricle resembles the normally functioning human heart in its capacity to maintain stroke volume despite elevations in afterload.24 Therefore, although the artificial ventricle has a demonstrated sensitivity to afterload,16-19 in the setting of augmented venous return, a net increase in stroke volume may result despite an increase in afterload, especially if the magnitude of increased venous return is relatively greater than the increase in afterload. Thus, the only mechanism by which a-adrenergic stimulation could increase cardiac output in this model is through augmentation of venous return. Similarly, this would account for the observed response to dobutamine infusion after /3-blockade with propranolol, in which the a-adrenergic activity of dobutamine would be unmasked, and with infusion of the levo isomer of dobutamine, which possesses only a-agonist activity. As with phenylephrine, an increase in cardiac output was observed with infusion of these agents despite substantial increases in systemic pressure. The increase in atrial pressures with the levo isomer infusion further supports this mechanism. That the ,/-agonist properties of dobutamine contribute to the increase in cardiac output in this model is demonstrated by the responses to the dextro isomer of dobutamine, which possesses only /3-adrenergic stimulating properties, and to the infusion of isoproterenol. Infusion of the dextro isomer in two of the cows resulted in an increase in cardiac output accompanied by a reduction of systemic vascular resistance. Both right and left atrial pressures increased with infusion of this isomer. Similarly, isoproterenol infusion resulted in an increase in cardiac output at all infusion rates and was accompanied by a decrease in systemic vascular resistance and an increase in atrial pressures. Whether the increase in cardiac output associated with these agents derives from the influence of /3-adrenergic stim- ulation on afterload, from /-adrenergic-mediated reduction of venous capacitance and augmented venous return, or from a combination of these mechanisms cannot be completely resolved based on the current data. However, an increase in atrial pressure similar to that seen after the levo isomer suggests that a primary influence on venous return is an important component of this response. The influence of dobutamine on the pulmonary vasculature appears to be less marked than that noted for the systemic vasculature. Although a decrease in pulmonary vascular resistance was noted, this occurred only at the maximal infusion rate. This contrasts with the marked sensitivity of the systemic vasculature in which significant decreases in resistance were noted at even the lowest infusion rate. These differences may arise because of variations in pulmonary and systemic vascular adrenergic receptor populations and affinities for dobutamine. Significant decreases in pulmonary vascular resistance accompanying dobutamine administration have been reported in humans with congestive heart failure.23,7 The present data suggest that such a decline in pulmonary vascular resistance may result from indirect influences such as reductions in ventricular filling pressures or reflex responses to increased cardiac output rather than from a direct effect on the pulmonary vasculature. Unlike previous investigations in humans with congestive heart failure, dobutamine administration in this model is associated with significant increases in right and left atrial pressures.2,37 This is consistent with the increase in forward flow and venous return observed in this setting. Unlike the native ventricle, which can shift both to new pressure-volume relations and to different points within a given relation in response to positive inotropic influence, the artificial ventricle will operate along a relatively fixed pressure-volume curve; this will tend to increase filling pressures in the setting of augmented venous return. These changes in atrial pressures and volumes may themselves contribute to the increase in cardiac output through potentiation of atrial contractility by an effect similar to the Starling mechanism of ventricular muscle contraction. Alternatively, dobutamine may directly influence contractility of the atria and in this manner augment ventricular filling. However, the importance of atrial systole is uncertain in this model in which atrioventricular synchrony is not preserved and, consequently, atrial filling occurs at random intervals relative to ventricular filling. The observed increase in cardiac output in this model was noted to occur with the first infusion rate and increase less markedly with subsequent infusions (Figure 1). This phenomenon is most likely a result of the fact that the maximal filling volume of the artificial ventricle was approached with the increase in cardiac output resulting from the first infusion, leaving little margin for further increase with subsequent infusions. It is conceivable that if a greater margin for increased filling were allowed, the cardiac output would continue to increase with further infu- Binkley et al Augmented Function of Artificial Heart Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 sions rather than achieving the observed plateau. However, operating the artificial ventricle at filling volumes below those used in the present study would result in inappropriately low cardiac outputs that would not be tolerated by the animal. The relevance of these observations to the clinically observed hemodynamic response to dobutamine infusion in patients with congestive heart failure provides a focus for future investigation. Although direct comparisons of the afterload sensitivity of the normal or failing ventricle with that of the artificial heart have not been made, extrapolation from prior studies in humans suggests that the artificial heart resembles the normal ventricle in terms of its sensitivity to afterload.24 In a report by Ross and Braunwald,24 decreases in stroke volume were not seen in ventricles with normal contractility until levels of afterload approaching the drive pressure of the artificial ventricle were achieved. The failing ventricle is known to have a much greater sensitivity to afterload; thus, it may be speculated that in the setting of ventricular failure, the vasoactive properties of dobutamine may have an even more profound effect on circulatory performance because of their modulation of loading conditions. This principle must be further tested in humans with congestive heart failure and in animal models of circulatory failure such as those that may be adapted from the present model. Conclusions The present data indicate that the vasoactive properties of dobutamine contribute significantly to the improved ventricular performance and augmentation of cardiac output associated with its administration. The model used in the present study effectively eliminates the inotropic influence of this agent and thus allows an analysis of the direct vascular effects of dobutamine distinct from its influence on myocardial contractility and attendant reflex vascular changes. Further elucidation of the mechanisms of vascular response to dobutamine and related positive inotropic agents may be provided through this model by comparing and contrasting the hemodynamic response to agents that vary in their adrenergic receptor affinity and activity. Acknowledgments The authors wish to thank Anne Brandt and Trichia Zavilla for their invaluable assistance in the preparation of this manuscript. References 1. Tuttle RR, Mills J: Dobutamine: Development of a new catecholamine to selectively increase cardiac contractility. Circ Res 1975;36:185-196 2. Leier CV, Webel J, Bush CA: The cardiovascular effects of the continuous infusion of dobutamine in patients with severe cardiac failure. Circulation 1977;56:468-472 3. Leier CV, Unverferth DV: Drugs five years later: Dobutamine. Ann Intem Med 1983;99:490-496 4. Vatner SF, McRitchie RJ, Braunwald E: Effects of dobutamine on left ventricular performance, coronary dynamics, 1215 and distribution of cardiac output in conscious dogs. J Clin Invest 1974;53:1265-1273 5. Robie NW, Glodberg LI: Comparative systemic and regional hemodynamic effects of dopamine and dobutamine. Am Heart J 1975;90:340-345 6. Liang CS, Hood WB Jr: Dobutamine infusion in conscious dogs with and without autonomic nervous system inhibition: Effects on systemic hemodynamics, regional flows and cardiac metabolism. J Pharmacol Exp Ther 1979;211:698-705 7. Leier CV, Heban P, Huss P, Bush CA, Lewis RP: Comparative systemic and regional hemodynamic effects of dopamine and dobutamine in patients with cardiomyopathic heart failure. Circulation 1977;58:466-475 8. Lewis, GRJ, Poole Wison PA, Angerpointer TA, Farnsworth AE, Williams BT, Coltart DJ: Measurement of the circulatory effects of dobutamine, a new inotropic agent, in patients following cardiac surgery. Am Heart J 1978;95:301-307 9. Raifer SI, Borow DM, Lang RM, Neuman A, Carroll JD: Effects of dopamine on left ventricular afterload and contractile state in heart failure: Relation to the activation of beta 1-adrenoceptors and dopamine receptors. J Am Coll Cardiol 1988;12:498-506 10. Ruffolo RR Jr, Spradlin TA, Pollock GD, Waddell JE, Murphy PJ: Alpha and beta adrenergic effects of the stereoisomers of dobutamine. J Pharmacol Exp Ther 1981;219:447-452 11. Olsen DB, Taenaka Y: State of the art and clinically applied pneumatic artificial hearts. Crit Care Clin 1986;2:195-207 12. Frazier OH, Col'n R, Taenaka Y: Surgical technique and hemodynamic characteristics of partial cardiac replacement with an artificial left ventricle. Tex Heart Inst J 1986;13:345-351 13. Anderson FL, DeVries WC, Anderson JL, Joyce LD: Evaluation of total artificial heart performance in man. Am J Cardiol 1984;54:394-398 14. Willshaw P, Nielsen SD, Nanas J, Pichel RH, Olsen DB: A cardiac output monitor and diagnostic unit for pneumatically driven artificial hearts. Artif Organs 1984;8:215-219 15. Olsen DB, Grosse Siestrup CH, Unger R, Kless H, Kolff WJ, Bucherl ES: The non-cardiac intrinsic autoregulation of tissue perfusion in calves with total artificial hearts. Proc Eur Soc Artif Organs 1977;4:263-270 16. Deleuze PH, Riebman JB, Paulis RDE, Olsen DB, Loisance DY: Regulation of pneumatic total artificial heart function: A review. Int JArtif Organs 1988;11:147-152 17. Uchida N, Ishikawa M, Watanabe T, Jacobs G, Oku T, Nasu M, Emoto H, Smith WA, Harasaki H, Kiraly R, Nose Y: Hemodynamic adaptation to exercise after total artificial heart implantation. TransAm SocArtif Intem Organs 1987;33:240-244 18. Hennig E, Grosse Siestrup C, Krautzberger W, Kless H, Bucherl ES: The relationship of cardiac output and venous pressure in long surviving calves with total artificial heart. Trans Am Soc Artif Intem Organs 1978;24:616-624 19. Goldenber I, Walker M, Roeller SK, Gobel FL, Joyce L, Jorgensen R, Madison JD, Pedersen WR: The Jarvik-7 total artificial heart is preload and afterload dependent (abstract). Circulation 1987;6(suppl IV):IV-404 20. Kaiser GA, Ross J, Braunwald E: Alpha and beta adrenergic receptor mechanisms in the systemic venous bed. J Pharmacol Exp Ther 1964;144:156-162 21. Van Maanen EF, Banning JW, Roebel LE, Morgan JP: Dopamine and norepinephrine increase venous return by stimulating alpha and beta adrenoceptors in the dog. J Cardiovasc Pharmacol 1988;11:627-634 22. Lee RW, Raya TE, Gay RG, Marcey 0, Goldman S: Beta-2 adrenoceptor control of the venous circulation in intact dogs. JPharmacol Exp Ther 1987;242:1138-1143 23. Fuchs RM, Rutlen DL, Powell WJ Jr: Effect of dobutamine on systemic capacity in the dog. Circ Res 1980;46:133-138 24. Ross J Jr, Braunwald E: The study of left ventricular function in man by increasing resistance to ventricular ejection with angiotensin. Circulation 1964;29:739-749 KEY WORDS positive inotropic agents * vascular mechanisms * congestive heart failure . Dobutamine increases cardiac output of the total artificial heart. Implications for vascular contribution of inotropic agents to augmented ventricular function. P F Binkley, K D Murray, K M Watson, P D Myerowitz and C V Leier Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 Circulation. 1991;84:1210-1215 doi: 10.1161/01.CIR.84.3.1210 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1991 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/84/3/1210 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/