Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Bacterial morphological plasticity wikipedia , lookup
Antimicrobial copper-alloy touch surfaces wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Neonatal infection wikipedia , lookup
Staphylococcus aureus wikipedia , lookup
Antimicrobial surface wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
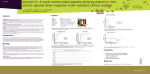
In Vitro Activity of Lefamulin Against Macrolide-Susceptible (MSMP) and Macrolide-Resistant (MRMP) Mycoplasma pneumoniae from the United States, Europe, and China Abstract 3972 1Dept. K. B. Waites1, D. M. Crabb1, L. B. Duffy1, Y. Liu2, and S. Paukner3 of Pathology, University of Alabama at Birmingham, Birmingham, AL, 2Fudan University, Shanghai, China, 3Nabriva Therapeutics AG, Vienna, Austria ABSTRACT (amended) MATERIALS & METHODS Background: Pleuromutilin (PM) antibiotics bind to the peptidyl transferase center of the 50S ribosomal subunit, blocking protein synthesis. Lefamulin (LMU, Nabriva Therapeutics) is a novel semi-synthetic PM with potent activity against gram-positive, gram-negative and atypical bacteria, including multi-drug resistant strains. LMU is formulated for IV and oral use and is in Phase 3 trials for the treatment of community-acquired bacterial pneumonia. Although macrolide-resistance in Mycoplasma pneumoniae (MPN) has become increasingly prevalent globally, in previous in vitro surveillance studies crossresistance between LMU and commonly used respiratory antibiotics has not been observed. We performed an in vitro evaluation of pediatric respiratory isolates of MSMP and MRMP from the US, Europe, and China. Methods: The broth microdilution MIC assay per CLSI guidelines (2011) was used to test strains against LMU and 4 comparators (see Table). Results: LMU was highly active against all strains, with MICs < 0.004 µg/ml. The LMU MIC90 for MRMP (0.002 µg/ml) was the lowest among all 5 drugs tested. Additionally, LMU minimum bactericidal concentrations (MBCs) were determined for 2 macrolide-susceptible and 6 macrolide-resistant isolates and all MBCs were 2 to 4 times the MIC values, indicating a bactericidal effect. Conclusions: LMU has potent in vitro activity against MPN, including macrolide resistant strains. LMU may be a promising therapeutic option for MPN infections. Lefamulin (LMU) Azithromycin (AZI) Erythromycin (ERY) Tetracycline (TET) Moxifloxacin (MOX) <0.00025-0.001 <0.00025-0.001 0.004-0.008 0.25-1 0.063-0.25 MIC50 <0.00025 0.0005 0.008 0.5 0.125 MIC90 0.001 0.001 0.008 1 0.25 0.0005-0.004 16 - >32 >32 0.25-1 0.125-0.25 MIC50 0.002 32 >32 0.5 0.125 MIC90 0.002 >32 >32 1 0.25 MSMP (n = 14) Range [µg/ml] MRMP (n = 36) Range [µg/ml] BACKGROUND & OBJECTIVES • • • • • Mycoplasma pneumoniae is an important cause of community-acquired respiratory infections in persons of all ages. Historically, macrolides have been the treatments of choice for these infections, especially in children for whom other drug classes such as tetracyclines and fluoroquinolones are less desirable because of potential adverse effects. Acquired macrolide resistance occurs in M. pneumoniae as a result of target modification caused by mutations in 23S rRNA. High level, clinically significant resistance began in Asia in 2000 and has spread globally. Recent surveillance from several states in the USA has indicated 13.2% of clinical isolates are macrolide-resistant. Pleuromutilins inhibit bacterial growth by binding to a highly conserved region of the peptidyl transferase center of the 50S ribosomal subunit via multiple non-covalent bonds and central positioning of their tricyclic core, as well as steric interference with nucleotides created by side chain that hinder tRNA rotary motion. Lefamulin (LMU) is a semi-synthetic pleuromutilin with potent activity against gram-positive, gram-negative and atypical bacteria, including multi-drug resistant strains, in Phase 3 clinical trials for treatment of community-acquired bacterial pneumonia. The objective of this study was to assess the in vitro activity of lefamulin against 14 MSMP and 36 MRMP pediatric clinical isolates and reference strains obtained from several countries to determine the potential utility of lefamulin in the treatment MSPP and MRMP infections. Bacterial Strains & Inoculum Preparation 50 unique strains of M. pneumoniae tested included 14 macrolide-susceptible clinical isolates obtained between 1980 and 2013 from several states in the USA, Europe, and China, and one reference strain (MAC). An additional 36 clinical isolates were obtained between 2009 and 2013 from several states in the USA and from Shanghai, China that had been shown previously to be macrolide-resistant (MIC > 32 µg/ml). Both P1 subtypes 1 and 2 were represented. Organism sources included nasal swabs, throat swabs, sputum, bronchoalveolar lavage fluids, and 1 cerebrospinal fluid. Most specimens were obtained from children. Organism stock cultures were previously tested to assess purity and to determine numbers present and then stored frozen at 80oC until tested. Organisms were thawed to room temperature and diluted in SP4 broth in 50 ml conical tubes to yield a final inoculum of approximately 104 CFU/ml. Broths were incubated aerobically at 37oC for 2 hours prior to use to allow mycoplasmas to become metabolically active prior to inoculating microtiter plates. Antimicrobial Agents Antimicrobial agents were obtained in powder form of known purity from their respective manufacturers or from commercial sources. Drugs were dissolved according to each manufacturer’s instructions and in accordance with CLSI guidelines. An appropriate amount of each powdered drug was weighed to prepare 10 mls of a stock solution, allowing for the percentage purity of each agent. If not used immediately, stock solutions were frozen at -80oC. Broth Microdilution Assay (CLSI Method) Each drug was tested in duplicate along with solvent, media, drug, and growth controls in accordance with CLSI guidelines. Microdilution trays were incubated aerobically at 37oC and examined after 18-24 hours and then daily for color change in the growth control wells. Endpoint MICs were usually measurable after 4-5 days of incubation. MIC Determination MICs were recorded as the lowest concentration of antimicrobial inhibiting color change in SP4 broth at the time the organism growth control well demonstrated a color change from pink to yellow indicative of glucose metabolism. Table 2. Mycoplasmacidal concentration of lefamulin MBC Determination The mycoplasmacidal concentration for lefamulin was determined for 2 macrolidesusceptible and 6 macrolide-resistant isolates by subculturing 0.30 ml of fluid from all wells of the MIC microtiter plate that did not show color change and from the growth control well at time of the initial color change into 2.97mls of SP4 broth to dilute the antibiotic beyond the MIC (1:100 dilution). A subculture onto SP4 agar was prepared from the lowest concentration showing color change in the MIC microtiter plate to verify organism viability. Subcultures were incubated aerobically at 37oC and agar plates were incubated at 37o C in air plus 5% CO2 until the growth control showed color change and the date was noted. The MBC was recorded as the last tube without color change after twice the length of incubation time for the MIC well to show initial color change. MBC controls included tetracycline (non-cidal) and levofloxacin (cidal) set up and monitored in the same manner as the investigational agent. Drugs were considered bactericidal if the MBC is < 4-fold (2 dilutions) of the MIC. Quality Control (QC) American Type Culture Collection (ATCC) strain 29342 (M129-B7) was included with each assay on every day of performance. MIC reference ranges for several antimicrobial agents have been established for this ATCC QC type strain. This QC strain performed as expected for all MIC assays for which data are presented. Solvent, drug, media, and growth controls also performed as expected. A final determination of the CFU/mL of the working dilution used to inoculate each microtiter plate was made by preparing 6 serial dilutions of the inoculum (0.1 ml inoculum in 0.9 ml of SP4 broth) and pipetting 20 µL of each dilution onto SP4 agar to verify that a proper dilution was made and that the inoculum contained 104-105 CFU/mL. Agar plates were incubated at 37o C in air plus 5% CO2 until colonies were visible and could be counted using a stereomicroscope. Results were considered valid if the control agar plate for organism concentration indicated that there were between 104 and 105 CFU/mL. • Lefamulin had potent activity against all M. pneumoniae isolates (n=50) with all MIC values ≤0.004 µg/mL. MIC50/90 of MS and MR subsets were ≤0.00025/0.001 µg/mL and 0.002/0.002 µg/mL (Table 1). • This activity was comparable to the activity of azithromycin when tested against the MS subset of organisms (MIC50/90, 0.0005-0.001 µg/mL). isolates were susceptible to moxifloxacin (MIC50/90, • All 0.125/0.25 µg/mL) and tetracycline (MIC50/90, 0.5/1 µg/mL) when CLSI breakpoints were applied. • Lefamulin MBC values of 0.002-0.008 µg/mL were 2- to 4-fold higher than the corresponding MICs (Table 2). Thus, lefamulin was bactericidal against all 8 M. pneumoniae isolates, including macrolideresistant and macrolide-susceptible isolates. Table 1. In vitro activity of lefamulin and comparators M. pneumoniae, total (n = 50) MSMP (n = 14) MRMP (n = 36) Strain Susceptibility MIC [µg/mL] MBC [µg/ml] 1 Macrolide-susceptible 0.0005 0.002 2 Macrolide-susceptible 0.001 0.002 3 Macrolide-resistant 0.001 0.004 4 Macrolide-resistant 0.002 0.008 5 Macrolide-resistant 0.002 0.008 6 Macrolide-resistant 0.001 0.004 7 Macrolide-resistant 0.002 0.004 8 Macrolide-resistant 0.002 0.008 DISCUSSION & CONCLUSIONS • • • RESULTS • Emergence of clinically significant macrolide resistance and its spread from Asia to Europe and North America has complicated empiric treatment for mycoplasmal infections. As a result, agents with a novel mechanism of action that are unaffected by resistance to commonly utilized respiratory antibacterial agents are needed. Lefamulin demonstrated excellent in vitro activity against M. pneumoniae, regardless of resistance phenotype, inhibiting all 50 strains at concentrations of < 0.004 µg/mL. Lefamulin demonstrated bactericidal activity against all 8 strains tested regardless of resistance phenotype. In conclusion, lefamulin is a promising agent for infections caused by M. pneumoniae in the respiratory tract. REFERENCES Eyal Z, Matzov D, Krupkin M, Wekselman I, Paukner S, Zimmerman E, Rozenberg H, Bashan A, Yonath A. 2015. Structural insights into species-specific features of the ribosome from the pathogen Staphylococcus aureus. Proc Natl Acad Sci USA 112: E5805-5814 Hastings, D.L., Harrington, K.J., Kutty, P.K., Rayman, R.J., et al. Mycoplasma pneumoniae outbreak in a long-Term care facility — Nebraska. MMWR March 27, 2015 / 64(11);296-299. MIC [µg/mL] Lefamulin Azithromycin Erythromycin Tetracycline Moxifloxacin Range ≤0.00025 - 0.004 ≤0.00025 - >32 0.004 - >32 0.25 - 1 0.063 - 0.25 MIC50 0.001 >32 >32 0.5 0.125 MIC90 0.002 >32 >32 1 0.25 Range <0.00025-0.001 <0.00025-0.001 0.004-0.008 0.25-1 0.063-0.25 MIC50 <0.00025 0.0005 0.008 0.5 0.125 MIC90 0.001 0.001 0.008 1 0.25 Range 0.0005-0.004 16 - >32 >32 0.25-1 0.125-0.25 Zheng, X., Lee, S., Selvarangen, R., Qin, X., Tang, Y-W., Stiles, J., Hong, T., Todd, K., Ratliff, A., Crabb, D.M., Xiao, L., Atkinson, T.P., Waites,K.B. Multicenter study of macrolideresistant Mycoplasma pneumoniae in the United States. Emerging Infectious Diseases 21:1470-1472, 2015. MIC50 0.002 32 >32 0.5 0.125 ACKNOWLEDGEMENTS MIC90 0.002 >32 >32 1 0.25 RESEARCH POSTER PRESENTATION DESIGN © 2015 www.PosterPresentations.com Contact: Ken Waites Univ. AL Birmingham Tel: (205) 934-4960 Email: [email protected] ASM Microbe / ICAAC 2016, June 16-20, Boston, MA Sader, H.S., Paukner, S., Ivezic-Schoenfeld,et al. Antimicrobial activity of the novel pleuromutilin antibiotic BC-3781 against organisms responsible for community-acquired respiratory tract infections (CARTIs) J Antimicrob Chemother 67:1170-1175, 2012. Waites, K.B., Duffy, L.B., Bébéar, C.M., et al. Methods for antimicrobial susceptibility testing for human mycoplasmas; approved guideline. Clinical and Laboratory Standards Institute, Wayne, PA. 2011. Waites, K.B., Lysynyansky, Bébéar, C.M. Antibiotic susceptibility testing and resistance in mycoplasmas of humans and animals. In: Browning, G., Citti, C., eds. Mollicutes Molecular Biology and Pathogenesis, Caister Academic Press. pp. 289-322, 2014. This work was supported by Nabriva Pharmaceuticals AG, Vienna, Austria