Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
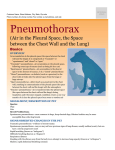
suppression of ovulation with oral contraceptives initially is recommended; however, recurrence of pneumothorax has been documented frequently.'6"7 Danazol, a weak androgen, has been used in the management of recurrent catamenial pneumothorax;'8 however, recurrence of pneumothorax, as occurred in our patient, has been documented.'9 Pleural abrasion and pleurectomy can prevent recurrent pneumothorax and hemothorax in these patients but cannot affect catamenial chest pain and hemoptysis. Hormonal suppression has been successful in only 40 percent of patients. Hysterectomy with bilateral salpingooophorectomy, the definitive treatment for thoracic endometriosis, may not be effective if estrogen replacement is commenced soon after surgery as occurred in our patient; delaying hormonal replacement therapy by several months should provide adequate time for the regression of ectopic endometrial tissue. Chemical pleurodesis with talc insufflation at thoracoscopy or minocycline, doxycycline, or talc slurry instillation via a chest tube should be considered as the initial treatment for catamenial pneumothorax and hemothorax even with intact ovarian function or hormonal replacement therapy. REFERENCES 1 Maurer RR, Schall JA, Mendez FL Jr. Chronic recurring spontaneous pneumothorax due to endometriosis of the diaphragm. JAMA 1972; 168:2012-14 2 Wilkins SB, Bell-Thompson J, Tyras DH. Hemothorax associated with endometriosis. J Thorac Cardiovasc Surg 1985; 89:636-38 3 Elliot DL, Barker AF, Dixon LM. Catamenial hemoptysis: new methods of diagnosis and therapy. Chest 1985; 87:687-88 4 Horsfield K. Catamenial pleural pain. Eur Respir J 1989; 2:1013-14 5 Mobbs GA, Sydney MB, Pfanner DW. Endometriosis of the lung. Lancet 1963; 1:472-74 6 Carter EJ, Ettensohn DB. Catamenial pneumothorax. Chest 1990; 98:713-16 7 Laws HL, Fox LS, Younger B. Bilateral catamenial pneumothorax. Arch Surg 1977; 112:627-28 8 Wilhelm JL, Scommegna A. Catamenial pneumothorax: bilateral occurrence while on suppressive therapy. Obstet Gynecol 1977; 50:227-31 9 Rossi NP, Goplerud CP. Recurrent catamenial pneumothorax. Arch Surg 1974; 109:173-76 10 Lee CY, DiLoreto PC, Beaudoin J. Catamenial pneumothorax. Obstet Gynecol 1974; 44:407-11 11 Hobbs JE, Bortnick R. Endometriosis of the lung: an experimental and clinical study. Am J Obstet Gynecol 1940; 40:832-43 12 Park W. The occurrence of decidual tissue within the lung: report of a case. J Pathol Bacteriol 1954; 67:563-70 13 Sahn SA. Catamenial pneumothorax and hemoptysis: current therapy of respiratory disease-3. Philadelphia: BC Decker, 1989;295-98 14 Zaatri GS, Gupta PK, Bhagavan BS, Jarboe BR. Cytopathology of pleural endometriosis. Acta Cytol 1982; 26:227-32 15 Grangberg I, Willems JA. Endometriosis of lung and pleura diagnosed by aspiration biopsy. Acta Cytol 1977; 21:295-97 16 Schoenfeld A, Ziv E, Zeelel Y, ans Ovadia J. Catamenial pneumothorax: a literature review and report of an unusual case. Obstet Gynecol Surv 1986; 41:20-24 17 Muller NL, Neelms B. Post-coital catamenial pneumothorax: report of a case not associated with endometriosis and success- 1896 fully treated with tubal ligation. Am Rev Respir Dis 1986;134:803-04 18 Hinson JM, Brigham KL, Daniell J. Catamenial pneumothorax in sisters. Chest 1981; 80:634-35 19 Furman WR, Wang KP, Summer WR, Terry PB. Catamenial pneumothorax: evaluation by fiberoptic pleuroscopy. Am Rev Respir Dis 1980; 121:137-40 Sudden Enlargement of a Deep Cervical Lymph Node During and After Treatment for Pulmonary Tuberculosis* E. Jane Carter, M.D., F.C.C.P.; and Susan Mates, M.D. A 25-year-old Filipino woman presented with sudden massive enlargement of a deep cervical lymph node on two occasions: during adequate treatment of pulmonary tuberculosis and again 2 years after completion of therapy. Although this immunologic phenomenon is well known in childhood tuberculosis, occurrence in adults should also be recognized. (Chest 1994; 106:1896-98) AFB=acid-fast bacilli Pathophysiologically, intrathoracic lymph nodes are probably infected in every case of pulmonary tuberculosis.' In children2 and HIV-infected patients,3 these nodes are usually or often clinically apparent. In HIVnegative adults, however, the nodes usually remain clinically silent. When treating pulmonary tuberculosis, it is important to be aware of the extensive area of lymphatic drainage from the affected lung (hilar, subcarinal, paratracheal, deep cervical, and abdominal nodes) and the potential complications from these nodes. We present a patient with documented pulmonary tuberculosis, whose nodal involvement became dramatically apparent when she suffered a sudden enlargement of a left deep cervical node with symptomatic impingement on her trachea during therapy and enlargement of a contralateral deep cervical node after completion of therapy. CASE REPORT A 25-year-old woman born in the Philippines presented in September 1988 with a 6-month history of an 8.1-kg weight loss and fatigue. She had immigrated to the United States 2 years previously. There was no relevant medical history. She denied all *From the Divisions of Pulmonary Medicine (Dr. Carter) and Infectious Diseases (Dr. Mates), Brown University School of Medicine and the Rhode Island Tuberculosis Clinic, Providence. Reprint requests: Dr. Carter, 877 Chalkstone Avenue, Providence, RI 02908 Lymph Node Enlargement Durng and After TB Treatment (Carter, Mates) Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21704/ on 04/29/2017 of treatment with medications; complianc&was deemed excellent. At the end of treatment, she had no palpable adenopathy. Chest radiograph continued to demonstrate bilateral upper lobe nodules that had remained stable for greater than 6 months. Twenty-two months following completion of therapy, she developed a 30X40-mm right deep cervical node. At this time she had no constitutional symptoms. Weight was stable. Chest radiograph was unchanged. The HIV serologic test was negative. Excisional biopsy of the lymph node was performed. Pathologic study revealed granulomatous inflammation and areas of caseous necrosis with acute inflammation. The AFB smear and subsequent culture were negative. It was elected not to retreat the patient, but to follow her clinically for any further signs of reactivation. She is now 19 months since excision without recurrence of nodal disease or constitutional symptoms suggestive of tuberculosis infection. DISCUSSION The sudden noninfectious enlargement of tuberculous lymph nodes during the course of adequate chemotherapy is well described.4-6 This complication occurs in 12 to 13 percent of patients, usually within the first months of therapy, and resolves without alteration of chemotherapy. It is postulated to be due to hypersensitivity to tuberculo- protein.4 FIGURE 1. Top, Chest radiograph demonstrates bilateral upper lobe reticulonodular infiltrates. Bottom, Chest CT scan obtained during therapy reveals an enlarged left deep cervical node with mild tracheal deviation. other symptoms, including cough, sputum production, fever, or chills. A chest radiograph (Fig 1, top) revealed bilateral upper lobe infiltrates without cavitation or intrathoracic adenopathy. The trachea was midline. Expectorated sputa for acid-fast bacilli were negative on two occasions. Fiberoptic bronchoscopy was performed; washings and postbronchoscopy sputum were AFB smear positive. She was started on a regimen of isoniazid, rifampin, and ethambutol. At this time she had no visible or palpable lymphadenopathy. Five weeks into treatment the patient suddenly developed a 20X30-mm left deep cervical node with a new cough described by the patient as due to tracheal impingement. Otherwise, she felt well. A computed tomographic scan of the neck (Fig 1, bottom) confirmed the node and demonstrated minimal tracheal displacement. No change was made in the patient's therapy. Three and a half months into therapy, the deep cervical node began to recede. Constitutional symptoms had disappeared; the patient regained her weight. Cultures of the bronchoscopy specimens eventually grew two organisms: a fully sensitive Mycobacterium tuberculosis and a fully resistant M avium. The second was believed to be a contaminant. When sensitivities were received 3 months into treatment, ethambutol therapy was discontinued. She completed 10½/2 months When an enlarged mediastinal node occurs during the course of therapy in a child and causes either respiratory difficulty or a collapse-consolidation lesion, the use of steroids, under the cover of effective antituberculous drugs, has been suggested.7 In our case, steroids were deferred as the patient's tracheal compression was mildly symptomatic, it did not threaten the airway, and sensitivities of the organism were not yet available. The probable immune mechanism of this phenomenon is underscored in that both episodes of enlargement resolved without specific therapy: the first occurred with characteristic timing in the treatment of a sensitive organism with adequate chemotherapy, and the biopsy specimen of the second was smear- and culture-negative. Our case is of particular interest because it demonstrates treatment-related node enlargement occurring not only during, but also after, effective chemotherapy. Most physicians caring for children with pulmonary tuberculosis have experienced the occurrence of sudden mediastinal node enlargement during treatment, usually presenting as a new infiltrate with an obstructive cause. It is important that those caring for adult patients also be aware of this possibility, the range of nodes that may be involved, and the potential complications. In most cases, no change in tuberculosis therapy is necessary. In some cases, steroids may be considered. ACKNOWLEDGMENTS: Special thanks to Margaret Smith, M.D., of Tulane University, New Orleans, and Marian Goble, M.D., of National Jewish Hospital for Immunologic and Respi- ratory Disease, Denver, for clinical assistance during care of this patient. REFERENCES 1 DesPrez RM, Hein CR. Mycobacterium tuberculosis. In: Mandell GL, Douglas GR Jr, Bennett JE, eds. Principles and practice of infectious diseases. 3rd ed. New York: Churchill Livingstone, 1985 2 Starke JR, Jacobs RF, Jereb J. Resurgence of tuberculosis in CHEST / 106 / 6 / DECEMBER, 1994 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21704/ on 04/29/2017 1897 children. J Pediatr 1992; 120:839-55 3 Hill AR, Premkumar S, Brustein S, Vaidya K, Powell S, Li P-W, et al. Disseminated tuberculosis in the acquired immunodeficiency syndrome era. Am Rev Respir Dis 1991; 144:1164-70 4 Campbell IA, Dyson AJ. Lymph node tuberculosis: a comparison of various methods of treatment. Tubercle 1977; 58:171-79 5 British Thoracic Society Research Committee. Short course chemotherapy for tuberculosis of lymph nodes: a controlled trial. BMJ 1985; 290:1106-08 6 Deitel M, Saldanha CF, Borowy ZJ, Ronald AG, Krajden S. Treatment of tuberculous masses in the neck. Can J Surg 1984; 27:90-3 7 Smith MHD, Marquis JR. Tuberculosis and other mycobacterial infections. In: Feigin RD, Cherry JD, eds. Textbook of pediatric of infectious diseases. Philadelphia: WB Saunders Co, 1981 Acquired Laryngomalacia as a Cause of Obstructive Sleep Apnea* Kota G. Chetty, M.B., F.C.C.P.; Fady Kadifa, Richard B. Berry, M.D., F.C.C.P.; and C. Kees Mahutte, M.D., Ph.D., F.C.C.P. M.D.; We describe a patient who, 4 years after a radical neck dissection and radiotherapy, presented with obstructive sleep apnea; upon bronchoscopy, he was found to have acquired laryngomalacia. Inspiration induced upper airway obstruction due to a large flaccid epiglottis, large aryepiglottic folds, and edema of the supraglottic area. We suggest that acquired laryngomalacia can lead to obstructive sleep apnea. Patients with obstructive sleep apnea after radical neck dissection need to be evaluated for laryngomalacia with fiberoptic laryngobronchos- copy. Examination of the upper airway is useful to determine the nature and extent of any upper airway col- lapse. (Chest 1994; 106:1898-1899) OSA=obstructive sleep apnea Key words: laryngomalacia; obstructive sleep apnea; up- per airway The mechanism of obstructive sleep apnea (OSA) appears to be multifactorial. Anatomic narrowing, increased compliance, altered reflexes, and inspiratory pharyngeal muscle dysfunction may all play a role in the pathophysiology of OSA.' Thus, structural alterations as well as the balance *From the Departments of Medicine, Long Beach Veterans Affairs Medical Center, Long Beach, Calif, and the University of California, Irvine, Calif. Re print requests: Dr. Chetty, Long Beach VAMC-IIIP, 5901 E. 7th Street, Long Beach, CA 90822 1898 between pharyngeal dilating and collapsing forces are important in maintaining upper airway patency. The collapsing segment itself may vary in location from the oropharynx to the hypopharynx.' Although the incidence is low, several upper airway abnormalities can produce the OSA syndrome. Examination of the nasal passages and oropharynx is performed routinely to detect nasal obstruction, enlarged tonsils or adenoids, macroglossia, and hypopharyngeal masses. In infants and children, OSA symptoms have been described with congenital laryngomalacia, an entity characterized by inspiratory stridor due to a flaccid epiglottis, redundant aryepiglottic folds, or hypotonia of the larynx. Belmont and Grundfast2 evaluated 30 such infants with congenital laryngeal stridor. Endoscopy characteristically showed flaccid supraglottic structures and medial prolapse of the arytenoid folds or of the epiglottis on inspiration. Seven of these infants had OSA. We describe an adult patient who had had a left radical neck dissection followed by radiotherapy and who years later presented with OSA. Endoscopy revealed flaccid supraglottic tissues. Airflow-induced collapse of the epiglottis into the laryngeal inlet causing intermittent obstruction was also noted. The term acquired laryngomalacia has been used to describe the preceding findings.3 Our patient suggests that acquired laryngomalacia due to neck surgery with radiotherapy may lead to OSA. CASE REPORT A 42-year-old man was admitted to the hospital with complaints of mild swelling of the lips, face, and tongue over 3 days. He had been diagnosed as having carcinoma of the anterior floor of the mouth 4 years before hospital admission. At that time, he underwent a left modified radical neck dissection with removal of the tumor mass and the inner table of the mandible. During the neck dissection, the omohyoid, geniohyoid, myelohyoid, and genioglossus muscles were sacrificed. A temporary tracheostomy was done and this closed with time. The patient also received radiation therapy using a 6-MeV linear accelerator. A total dose of 60 Gy was delivered to the midline of the neck and a dose of 50 Gy was delivered to the lower neck. Several months after radiation therapy, he was started on a regimen of levothyroxine (120 ,ug each day). He quit smoking. The patient consumed a moderate amount of alcohol. Examination at the time of hospital admission showed an oriented afebrile patient with a weight of 105 kg and height of 185 cm. The left side of the neck was deformed and there was mild edema of the lower lip and left side of the face. No lymph nodes were palpable. A mild inspiratory stridor was noted. The chest, cardiovascular, and results of the rest of the examination were normal. Results of routine laboratory tests as well as thyroid function tests were normal. Spirometry showed a FEV, of 3.82 L (83 percent of predicted) and a FVC of 4.29 L (79 percent of predicted). The flow volume curve, including the inspiratory limb, was normal. Chest radiograph was normal. A computed tomographic scan of the neck and chest showed no masses. Angioedema was suspected clinically and the patient was treated with antihistamines and steroids without any benefit. On the ward, the patient was noted to snore and have apneic events. On further questioning, he admitted to mild daytime sleepiness. Consequently, a nocturnal polysomnography study was performed. This study showed a an apnea + hypopnea index of 67 events per hour of sleep. The apneas were associated with oxygen desaturations from a baseline of 95 percent to a minimum level of 60 percent. One hundred fifteen episodes of oxygen de- Laryngomalacia as a Cause of Obstructive Sleep Apnea (Chetty et al) Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21704/ on 04/29/2017