Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Polysubstance dependence wikipedia , lookup
Neuropharmacology wikipedia , lookup
Prescription costs wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
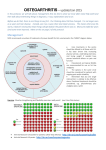
Effect of Diclofenac Sodium 1.5% Topical Solution on Coagulation Parameters in Patients With Knee Osteoarthritis Taking Anticoagulant and Antithrombotic Medications Theresa M. Gillis, PA-C, CRC; Nathan Wei, MD, FACP, FACR ▪ Arthritis Treatment Center, Frederick, MD, USA Introduction • Although nonsteroidal anti-inflammatory drugs (NSAIDs) are effective for managing mild to moderately severe pain, they are also associated with adverse events (AEs) involving the cardiovascular (CV) and gastrointestinal (GI) systems1 – These effects are related to the primary mechanism of action of NSAIDs (ie, cyclooxygenase [COX] enzyme inhibition)1 • Additionally, NSAIDs have been shown to significantly decrease platelet aggregation and to increase coagulation time2,3 – This effect has been observed with both nonselective and COX-2 selective NSAIDs – Using NSAIDs in patients who are also being treated with anticoagulants may further increase the risk for bleeding – An almost 13-fold increase in the risk of GI hemorrhage has been observed in patients taking anticoagulants and NSAIDs compared with those who use neither drug4 • NSAIDs are not recommended for patients taking anticoagulants (eg, warfarin);5 however, it is still unclear whether this interaction is related to higher plasma concentrations – Topical NSAIDs have been shown to produce lower plasma concentrations and to have better tolerability profiles than orally administered NSAIDs, particularly for AEs involving the GI system6 – Use of topical NSAIDs reduces systemic exposure, which may result in less risk for GI bleeding when taken with anticoagulant and antiplatelet medications Objective • To determine whether diclofenac sodium 1.5% topical solution increases the anticoagulant and antithrombotic effects of warfarin, dabigatran, or aspirin and/or clopidogrel in patients with osteoarthritis (OA) of the knee Methods Study Design • Single-center, phase-3, open-label, 4-week study Study Drugs • Diclofenac sodium 1.5% topical solution was applied to the knee 4 times daily as 40 drops during the 4-week treatment period7 • Patients were permitted to use acetaminophen (maximum dose, 1500 mg/day) as a supplemental analgesic Patients Inclusion Criteria • Patients aged ≥55 years who had moderate to severe OA of the knee and had been taking stable doses of warfarin, dabigatran, or aspirin and/or clopidogrel – OA symptoms needed to be present for ≥3 months, ≥40 mm on a 0 to 100 mm visual analog scale at baseline, and grade 2-4 on the Kellgren-Lawrence scale within the previous 2 years • For patients with bilateral knee pain, the more symptomatic knee was the index knee • Control group consisted of patients treated with a different concurrent anticoagulant or antithrombotic treatment than the analysis population (eg, the control group for warfarin-treated patients were receiving dabigatran, aspirin, or clopidogrel) Exclusion Criteria • Patients were required to abstain from using oral analgesics except for acetaminophen, which was permitted for use as a supplemental analgesic – However, patients taking low-dose aspirin for CV health could continue to receive stable doses throughout the study • Other exclusion criteria included: – Abnormal coagulation test results that would require an alteration in anticoagulant dose – Skin breakdown or rash at the application site POSTER # 166 American Academy of Pain Medicine ▪ Phoenix, AZ ▪ March 6-9, 2014 Figure 2: Median Prothrombin Time in Patients Receiving Diclofenac Sodium 1.5% Topical Solution and Warfarin (n=9) and Controls (n=12) Figure 4: Median Platelet Aggregation Time in Patients Receiving Diclofenac Sodium 1.5% Topical Solution and Aspirin and/or Clopidogrel (n=10) and Controls (n=11) • In this study, diclofenac sodium 1.5% topical solution did not interfere with coagulation parameters to a clinically significant degree in patients with moderate to severe OA of the knee receiving concomitant anticoagulant therapy Outcome Measures • The primary outcomes were international normalized ratio (INR), prothrombin time (PT), partial thromboplastin time, activated partial thromboplastin time (aPTT), and platelet aggregation time measured weekly during the 4-week study period • Tolerability was assessed by measuring the occurrence of AEs, defined as any untoward medical occurrence temporally associated with the use of study drug – Intensity (ie, mild, moderate, or severe) and relationship to study drug (ie, not related, possibly related, probably related, or definitely related) were also assessed References 1. Barkin RL, Beckerman M, Blum SL, Clark FM, Koh EK, Wu DS. Should nonsteroidal anti-inflammatory drugs (NSAIDs) be prescribed to the older adult? Drugs Aging. 2010;27(10):775-789. 2. Lattuca B, Khoueiry Z, Malcles G, Davy JM, Leclercq F. Drug interactions between nonsteroidal anti-inflammatory drugs and cardiovascular treatments (except anti-agregant therapy). Antiinflamm Antiallergy Agents Med Chem. 2013;12(1):36-46. Statistics 3. Cheetham TC, Levy G, Niu F, Bixler F. Gastrointestinal safety of nonsteroidal antiinflammatory drugs and selective cyclooxygenase-2 inhibitors in patients on warfarin. Ann Pharmacother. 2009;43(11):1765-1773. • Because of the exploratory nature of this study, the sample size was determined based on clinical considerations; therefore, no formal statistical analysis was used • Safety data were summarized descriptively Results Baseline Demographics • Data were available for 21 patients aged 56 to 82 years (mean age, 70 years); female patients (n=14) outnumbered male patients (n=7) • Patients were primarily receiving warfarin 2 mg to 10 mg, clopidogrel 75 mg, aspirin 81 mg, and/or dabigatran 150 mg – However, 2 patients were being treated with higher doses of aspirin (ie, 325 mg) Coagulation Parameters • Increases were observed in median INR (baseline, 1.5; final evaluation,1.9) and PT (baseline, 16.7 seconds; final evaluation, 21.1 seconds) among warfarin users (n=9; Figures 1 and 2) Figure 1: Median International Normalized Ratio Values in Patients Receiving Diclofenac Sodium 1.5% Topical Solution and Warfarin (n=9) and Controls (n=12) Conclusions 4. Shorr RI, Ray WA, Daugherty JR, Griffin MR. Concurrent use of nonsteroidal antiinflammatory drugs and oral anticoagulants places elderly persons at high risk for hemorrhagic peptic ulcer disease. Arch Intern Med. 1993;153(14):1665-1670. • Median aPTT was similar at baseline (53.4 seconds) and final evaluation (53.8 seconds) among dabigatran users (n=4; Figure 3) • Median platelet aggregation time decreased in the aspirin and clopidogrel groups (n=10; baseline, 300 seconds; final evaluation, 232 seconds; Figure 4) • The median final visit INR (1.0), PT (10.8 seconds), aPTT (31.2 seconds), and platelet aggregation time (103 seconds) for the control group were lower than that of the active treatment group Figure 3: Median Activated Partial Thromboplastin Time in Patients Receiving Diclofenac Sodium 1.5% Topical Solution and Dabigatran (n=4) and Controls (n=17) Tolerability • AEs, including nausea, headache, bilateral swelling of the ankles, and rash, were observed in 4 patients and were all classified as being mild or moderate – No AEs related to bleeding were observed Discussion • Orally administered NSAIDs have been shown to produce significant disruptions in platelet function in healthy subjects, leading to increased risk of bleeding, especially of the GI tract8,9 – Increases in hospital-associated GI bleeding have been observed when warfarin is coadministered with nonselective and COX-2 selective NSAIDs3 • The results of this study are consistent with previous analyses evaluating topical NSAIDs, which demonstrated little to no effect on platelet aggregation – A recent study evaluating diclofenac sodium 1% gel demonstrated significantly lower degree of inhibition of platelet aggregation compared with oral diclofenac 50 mg (P≤0.003) in a population of healthy subjects10 ▪ It was concluded by the authors that this effect is possibly caused by the lower diclofenac plasma concentrations of the topical NSAID – In a large-scale analysis of hospital admissions, topical NSAIDs were not associated with a significant risk of upper GI bleeding and perforation, whereas oral NSAIDs were associated with significant risk for developing these events11 – However, there are more studies needed specifically exploring the effect of topical NSAIDs on patients being treated with anticoagulant and antiplatelet medications to confirm the results of this and other previously conducted studies Limitations • This exploratory study has multiple limitations, including an open-label and nonrandomized design and a small study population; therefore, the results should be interpreted with these limitations in mind 5. Holbrook AM, Pereira JA, Labiris R, et al. Systematic overview of warfarin and its drug and food interactions. Arch Intern Med. 2005;165(10):1095-1106. 6. Derry S, Moore RA, Rabbie R. Topical NSAIDs for chronic musculoskeletal pain in adults. Cochrane Database Syst Rev. 2012;9:CD007400. 7.Pennsaid® (diclofenac sodium topical solution) 1.5% w/w [package insert]. Hazelwood, MO: Mallinckrodt Brand Pharmaceuticals, Inc.; 2010. 8. Bauer KA, Gerson W, Wright C, et al. Platelet function following administration of a novel formulation of intravenous diclofenac sodium versus active comparators: a randomized, single dose, crossover study in healthy male volunteers. J Clin Anesth. 2010;22(7):510-518. 9. Schwartz JI, Agrawal NG, Hartford AH, et al. The effect of etoricoxib on the pharmacodynamics and pharmacokinetics of warfarin. J Clin Pharmacol. 2007;47(5):620-627. 10. Kienzler JL, Gold M, Nollevaux F. Systemic bioavailability of topical diclofenac sodium gel 1% versus oral diclofenac sodium in healthy volunteers. J Clin Pharmacol. 2010;50(1):50-61. 11. Evans JM, McMahon AD, McGilchrist MM, et al. Topical non-steroidal anti-inflammatory drugs and admission to hospital for upper gastrointestinal bleeding and perforation: a record linkage case-control study. BMJ. 1995;311(6996):22-26. Acknowledgment Technical editorial and medical writing support for the development of this poster was provided by Dennis Stancavish, MA, Synchrony Medical Communications, LLC, West Chester, PA. Funding for this support was provided by the Arthritis Treatment Center, Frederick, MD, and Mallinckrodt Inc., Hazelwood, MO. Disclosures The authors have no disclosures to report.