Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
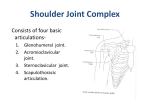
The Shoulder Joint (Glenohumeral Articulation) By Prof. Dr. Muhammad Imran Qureshi Type Of the Joint: Simple Synovial Variety Of the Joint: Multiaxial Ball and Socket Variety Articular Surfaces: Head Of the Humerus Glenoid Fossa of The Scapula Disproportion between the large rounded head of Humerus and small shallow Glenoid cavity Fibrous Capsule: On the Scapula, it is attached beyond the supraglenoid tubercle and margins of the Labrum. On the Humerus, it is attached around the articular margins of the Head (anatomical Neck) except inferiorly, where it is attached to the surgical neck (which lies about 1.5 cm below the articular margin). The capsule bridges the gap between the greater and lesser tuberosities i.e. the intertubercular groove, forming the Transverse ligament. A gap is always present in the anterior part of the capsule, through which, the cavity of the joint communicates with the subscapularis bursa.A similar gap may sometimes be present posteriorly, communicating the joint cavity with the Infraspinatus bursa. The fibers of the capsule run HORIZONTALLY between the scapula and the humerus.It is THICK and STRONG but very LAX.Near the humerus, it is greatly thickened by fusion of the tendons of short scapular muscles (Rotator Cuff).The tendon of the long head of biceps is Intracapsular. Synovial Capsule / Membrane: On the Scapula, It is attached around the glenoid labrum and lines the capsule. On the Humerus, it is attached to the articular margins of the head, and covers the bare area of the surgical neck that lies within the capsule on the upper end of the shaft medially. It herniates through the gap in the anterior part of the capsule, to communicate with the subscapularis bursa. It invests the tendon of long head of biceps in a tubular sleeve that is reflected back on the tendon to the transverse ligament and adjoining floor of the intertubercular sulcus. This sleeve of synovial membrane glides to and fro with the tendon of the long head of biceps during the movements of abduction and adduction. 1 Ligaments of the joint: Extracapsular Ligaments: Coracohumeral Ligament: Passes laterally across the capsule, from the under surface of the coracoid process to the margins of the greater tuberosity and along the transverse ligament. Coracoacromial Ligament: Passes from the medial border of acromion, in front of the acromioclavicular joint and fans out in the form of a strong flat triangular band, to the coracoid Process. It lies above the head of the humerus and serves to increase the surface upon which, the head of the humerus is supported. It is separated from the ‘rotator cuff’ by the sub acromial bursa. Transverse Humeral Ligament Intracapsular Ligaments: Glenohumeral Ligaments: These are thickenings above and below the opening into the subscapular bursa in the anterior part of the capsule. They are three in number. Superior glenohumeral ligament: Is a thickened transverse part that spans between the upper ends of the glenoid rim and anatomical neck of the humerus. Inferior glenohumeral ligament: Is a thickened transverse part that spans between the lower parts of the glenoid rim to the lower part of the anatomical neck of the humerus. Middle glenohumeral ligament: Is a thickened oblique part that spans between the upper part of the glenoid rim to the lower part of the anatomical neck of the humerus. Blood Supply of the joint: Branches from the following arteries supply the joint: Anterior Circumflex Humeral Artery Posterior Circumflex Humeral Artery Suprascapular Artery Circumflex Scapular artery. Nerve Supply of the joint: It follows the Hilton’s Law. It is innervated predominantly from the posterior cord of the brachial plexus via the Axillary and Radial nerves.The capsule is also supplied by the Suprascapular Nerve, the Lateral Pectoral nerve and the Musculocutaneous nerve. Movements of the joint: Due to 1:4 disproportion between the head of Humeral and the Glenoid fossa, there is a substantial freedom for a variety of 2 movements at this joint. Three basic movements take place at this joint: Flexion and Extension, Abduction and Adduction, and Rotation. Circumduction is merely a combination of the first two movements in a specific sequence. Movements at the shoulder joint are accompanied by movements of the scapula on the thoracic wall and by subsequent movements of the Clavicle. (Thoracohumeral articulation) Analysis of the movements: Abduction: It takes place in the coronal plane along an anteroposterior axis, and is produced by the Supraspinatus and the Deltoid (but only for the initial 90o). The Supraspinatus (attached to the greater tuberosity) tends to pull it upwards. It initiates the movement. This appears to cause the head of the humerus to move down slightly as the greater tuberosity is pulled upwards and medially. At the same time, the subscapularis, teres minor and major and infraspinatus exert a downward pull on the head of the humerus and act as a stabilizing couple against the upward pull of the deltoid. Movement beyond 90o is produced by subsequent scapular rotation, which is achieved by the simultaneous contraction of the upper and lower fibers of the Trapezius and the lowest four digitations of the Serratus anterior. Range is 180o. 120o of this movement takes place at the shoulder joint while the remaining 60o is provided by scapular rotation. In other words, over the whole range, the ratio of shoulder joint to scapular movement is 2:1. For the First 30o, the scapular movement is negligible. Adduction: It is produced by the short scapular muscles (except supraspinatus) when the deltoid relaxes. This movement is aided by the contraction of the great muscles of the axillary fold (Pectoralis Major and Latissimus Dorsi) Flexion: It is produced by the clavicular head of Pectoralis Major and anterior fibers of the deltoid. Extension: It is produced by the Latissimus dorsi, Posterior fibers of deltoid and long head of triceps. Lateral Rotation: It is produced by Infraspinatus and Teres Minor Medial Rotation: It is produced by the Subscapularis and Teres Major. 3 Stability Of the joint: It depends upon THREE factors: Bony Factors Ligamentous Factors, and Muscular Factors Bony Factors: There is 1:4 disproportion between the head of the Humerus and the Glenoid fossa. The Glenoid fossa is very shallow. Some stability is contributed to the joint by the Glenoid Labrum. The Capsule, though strong but is lax. So if the labrum is fractured, the dislocation becomes inevitable. So, the bony factors are the least important as far as the stability of the joint is concerned. Ligamentous Factors: This plays a relatively more important role in the stability of the joint. In this respect, the coracoacromial ligament (along with the under surfaces of the respective bones) plays a vital role. The whole structure is called the coracoacromial arch. The sub acromial bursa located below the arch functions mechanically as an ‘articular surface’ Muscular Factors: These play the MOST IMPORTANT role in the stability of the joint. Of the muscles, the most important role is played by the ROTATOR CUFF, which alone is an indispensable factor regarding the stability of the joint. The pull of the rotator cuff not only holds the head of the humerus against the glenoid fossa, but it also prevents the lax capsule of the joint from being nipped. Since there is no rotator cuff inferiorly, the capsule here is attached well below the articular margins. Muscles attaching Humerus to the Pectoral Girdle: All these muscles assist the joint by maintaining their TONE. The Long heads of Biceps and Triceps play a vital role in this respect. The tendon of the Long head of Biceps is intracapsular and passes above the head of the humerus, preventing upward displacement, while the tendon of long head of Triceps passes below the joint when it is abducted. In fact, during abduction, the tendon of long head of triceps is the only structure that supports the head from below (which is the weakest part of the capsule) 4 Clinical Considerations If the capsule of the joint becomes inflamed, it may thicken and fibrose. This is accompanied by synovitis, which results in contracture and adhesions, giving rise to a condition called the “Adhesive Capsulitis” or “Frozen Shoulder”. The laxity of the capsule, which is an asset for the movement, now becomes a liability by providing a greater surface area for adhesions. Dislocation of the shoulder joint will occur if a strong downward force is applied to the semi abducted shoulder. This may occur in contact sports when a tackle is being discouraged by an outstretched arm. The problem may become recurrent if the capsule and ligaments are weakened, and in this context the strength of the rotator cuff muscles assumes paramount importance. The sub acromial surface forms a tunnel occupied by the tendon of supraspinatus and the overlying sub acromial bursa, which protects the tendon from the coracoacromial arch. If either the tendon or the bursa (or both) get inflamed, abduction becomes painful in an arc of movement classically between about 450 and 1600 as the greater tuberosity compresses the inflamed sub acromial structures. This is known as the “Painful arc”and is a useful sign in clinical diagnosis 5