Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Approach to Dyspnea
Mani S. Kavuru, MD
Professor & Division Chief
Pulmonary & Critical Care Medicine
Thomas Jefferson University / Hospital
Key learning Objectives
• Familiarize with eliciting history relevant to
dyspnea & scales utilized;
• Be able to define a diagnostic approach to
dyspnea, with emphasis in the outpatient area;
• Develop facility with common pulmonary
diagnostic modalities from PFTs, exercise
studies, imaging, and biopsy
• Apply these concepts in case-based scenarios
ATS Definition of Dyspnea
• Patient self-reported, subjective
• “Breathing discomfort, qualitatively distinct
sensations varying in intensity”
• Arises from “interactions among multiple
physiological, psychological, social, and
environmental factors and may induce
secondary psychological and behavioral
responses”
• Prefer “breathlessness” as patient-centric
Dyspnea
• Subjective
• Discomfort associated with the act of breathing
in circumstances it is unexpected;
• Further characterize by:
◊nature of onset (acute, chronic), duration
◊evolution over time
◊associated symptoms (cough, CP, wheeze,
orthopnea)
◊physiologic vs. pathologic
◊quantify (“no SOB” is inadequate)
Caveats re. Dyspnea Evaluation
• Note discrepancy between patient’s perception (under-reported) and
physician’s clinical evaluation (under-recognized);
• Be able to recognize fatigue vs. activity intolerance vs. dyspnea;
• Be aware of natural history of dyspnea in various clinical settings
and disease entities;
• Co-existence of multiple causes of dyspnea is common; so need to
be able to define relative contribution of lung disease (as opposed to
obesity, anemia, LBP);
• Be adept at distiguishing cardiac vs. pulmonary causes of SOB;
• FEV1 as a surrogate marker can be misleading;
• PFTs and exercise studies do not assess severity of feeling of
breathlessness (a sensation); but rather impact on functional
capacity or physiological consequences;
• Don’t be fooled by “normal O2 sat’n”;
Pathogenesis of Dyspnea
• Dynamic hyperinflation
• Increased ventilatory demand relative to
capacity
• Abnormalities in gas exchange
• Inspiratory muscle weakness
• Cognitive & psychological influences (i.e.
fear, anxiety)
• Other
The “Oxygen Cost” Diagram
“What can you do before you become short of breath?”
Patient makes a mark on a 10cm line at the point beyond which they become
breathless
The oxygen cost diagram is more sensitive to change than the MRC scale - it
consists of a 10cm line with everyday activities placed proportionately according to
their oxygen cost. Patients place a mark on a 10cm line, beyond which they become
Reference
breathless. The ability score is the distance in centimetres from the zero point.
McGavin CR, Artvinli M, Naoe H, McHardy GJR. Dyspnoea, disability and distance walked:
comparison of estimates of exercise performance in respiratory disease. Br Med J 1978; 2:
241–243
Bausewein. Respiratory Med 2007
1. A 62 y/o WM smoker (200+ pk-yr) with progressive dyspnea and activity
intolerance over past 6 mos; Exam: markedly reduced BSs with prolonged
expiration, distant heart tones, 1+ edema; CXR is clear; spiro shows FEV1 to
be 30%, FVC 50%, ratio 0.32; RA PaO2 is 78;
2. A 45 y/o with hx of pred-dependent asthma since childhood; is a smoker; has
gained 100+ lbs; several prior admits for resp failure; now presents to clinic
with worsened SOB, wheezing; Exam: verbal, no distress, audible wheezing,
morbidly obese; RA O2 sat = 98%;
3. A 75 y/o non-smoker presents with
Clinical Evaluation for Lung
Disease
• PFTs: spirometry (screening/simple), lung volumes,
DLCO, O2 assessment; [assess for copd, asthma, UAO, ILD]
• Exercise assessment (6MWT, GXT) [assess functional
status of any cardiopulm disease]
• Bronchoprovocation challenge
[assess for asthma]
• Serial chest radiographs, CTA / HRCT chest [assess for
ILD, cancer, CHF, HP, other]
• Targeted Labs: cbc, chems, HPP, CVD, other [assess
for anemia, CVD, HP, sarcoid, vasculitis]
• Bronchoscopy (BAL, TBBx, EBUS) [assess for any
parenchymal lung disease that produces infiltrates on CXR/CT]
• Surgical lung biopsy (VATS, mede) [assess for any
parenchymal lung disease that produces infiltrates on CXR/CT]
Spectrum of Dyspnea &
Respiratory Syndromes
“Normal” CXR/CT
• Asthma
• COPD & emphysema
• Occupational “asthma-like”
syndromes
• Cardiac causes
• Upper airway disease
• Pulmonary vascular
disease
• Neuromuscular disease
• Other (anemia, obesity,
deconditioning)
Abnormal CXR/CT
• Acute pneumonia
syndromes, alveolitis
• Chronic fibrotic diseases
(IPF, CVD, sarcoid)
• Pneumoconioses
• Malignancy
• Cardiac disease
• PE
• Other
Clinical vignette #2 (Q4)
A 45 y/o non-smoker presents with episodic
dyspnea and cough of 4 months’ duration. She
denies nasal drainage, wheezing or heartburn.
A chest x-ray is normal. Which of the following
is the next best step?
a. Empiric therapy with antibiotics
b. 24 hour pH monitoring
c. Exercise and/or cold air challenge
d. Spirometry, if airway obstruction is
present, proceed with methacholine
challenge test
e. Spirometry, if normal, proceed with
methacholine provocation test
Clinical vignette #3 (Q8)
60 y/o non-smoker with progressive dyspnea over 8
mos; hx is remarkable for prior thyroid cancer, s/p 2
surgeries, XRT to neck. W/up shows normal ABGs,
spirometry, lung volumes/DLCO, HRCT chest, V/Q
scan. Which is next best test to establish a diagnosis?
a.
b.
c.
d.
e.
Open lung biopsy
Flow volume loop
100% shunt study
2D echocardiogram with bubbles
Methacholine provocation study
Clinical Vignette #4 (Q9)
50 y/o male ex-smoker (20 pk-yrs) with DOE, daily cough +/sputum, activity intolerance, wheezing; Exam: reduced breath
sounds; CXR: hyperinflated, clear; spiro: severe reduction in
FEV1 with no BD response and reduced DLCO; several family
members died prematurely. Which of the following is the best
approach?
a.
b.
c.
d.
e.
Blood test to prove diagnosis, then optimize inhalers, home O2,
and start intermittent monthly infusions
Proceed to lung transplantation
Bronchoscopy with BAL, biopsy
Liver biopsy
Serum cotinine levels
Clinical vignette #5 (Q11)
•
66 y/o WF smoker with 6-12 mos hx of progressive
dyspnea, cough, activity intolerance. Exam shows
clubbing of fingers, bibasilar crackles, trace edema.
PFTs show reduction in DLCO and volumes with
normal ratio and flows; RA PaO2 55; CXR is diffusely
abnormal. What is the most likely abnormal
compartment?
a.
b.
c.
d.
e.
Upper airways
Pulmonary vasculature
Small airways, tethering structures
Interstitium
“Bellows” or resp muscles/nerves
Vignettes, Questions
•
•
•
•
•
•
Clinical vig #1 (Q 1-3)
Clinical vig #2 (Q4-7)
Clinical vig #3 (Q8)
Clinical vig #4 (Q9-10)
Clinical vig #5 (Q11)
Clinical vignette #6 (Q12)
Initial Approach to Respiratory
Disease
• Typical Symptoms
–
–
–
–
–
–
–
Dyspnea
Cough +/- sputum
Activity intolerance
Fatigue
Chest pain
Wheezing
Note: pattern of sx
• History
– Temporal aspects
• acute or chronic
– Assoc systemic sx
– Response to therapies
– Family history
• IPF, CTD
• Exposures
–
–
–
–
–
–
–
Sick contacts
Tobacco
Occupational
Hobbies
Pets
Drugs
Radiation
Classification of Lung
Diseases
• Obstructive Disease: asthma;
chronic bronchitis; emphysema; CF;
• Restriction--Intra-parenchymal
disease (lung tissue is abnormal, e.g.
HP, pulmonary fibrosis)
• Restriction--Extra-parenchymal
disease (lung tissue is normal); chest
wall deformities, kyphosis, scoliosis,
obesity, pleural effusions, ascites
– Neuromuscular disorders (“bellows”)
Clinical Vignette #1
• 22 y/o woman non-smoker with episodic
chest tightness, wheezing, SOB, coughing
with exposure to cold air, exercise
• FMHx: allergies, eczema, asthma
• Exam: tachypnea; bilat wheezes
• CXR: clear
• Spirometry: reduced flows (i.e. FEV1)
Question 1
Which of the statements
regarding this disease is
incorrect?
a. There has been a recent upward trend
b. Death occurs frequently
c. Excessive use of -agonists has been
implicated
d. Subgroups of patients are at greatest
risk
e. Inadequate use of certain medications
have been implicated
Question 2
All of the following features are
typical for bronchial asthma except:
a. Airway hyperreactivity
b. Severe hypoxemia
c. Obstructive impairment with reversibility
d. Mild increase in diffusing capacity
(DLCO)
e. Airway inflammation
Spirometry
• Two main measurements:
– total volume exhaled (FVC)
• lung/thorax expansion
– HPP, IPF - restrictive lung diseases
– volume exhaled in 1st second of exhalation
(FEV1)
• airway diameter
– obstructive lung diseases
» asthma, emphysema, chronic bronchitis, etc.
Question 3
•
What is the single best maintenance
therapy for chronic moderate asthma?
a.
b.
c.
d.
e.
Prednisone
Albuterol or epinephrine
Inhaled steroids
Cromoglycates
Leukotriene blockers
Question 5
A 20 y/o with a history of episodic asthma presents to the
emergency department (ED) with dyspnea, wheezing, and
chest tightness of several days duration. A PEFR was 200
1/min. Inhaled -agonists were administered 30 minutes
apart x 3. She became asymptomatic. Which of the following
is the next best step?
a. Send home with -MDI q 4 hours
b. Send home with inhaled steroids and PRN MDI
c. Begin IV aminophylline, admit for observation
d. Administer p.o. steroid in ED, discharge home
with steroid taper over two weeks and PRN
-MDI
e. Assess ABGs and CXR prior to further
treatment
Question 6
Reversible factors that may contribute to
"steroid-dependent" asthma include all of the
following except:
a. Misdiagnosis of asthma
b. Presence of a co-morbid disease
(i.e., sinusitis, GERD, etc.)
c. Steroid receptor polymorphism
d. Patient non-compliance with
medications
e. Poor control of environmental triggers
Question 7
A 30 y/o non-smoker presents to the clinic with a 3 year history of
episodic cough, chest tightness, and wheezing. She meticulously
uses a -MDI at least 2 puffs every 6 hours with good relief of
symptoms. She takes several additional puffs at night to help with
sleep. A month ago, after an acute URI, she required ER care. She
was very aggressively treated and discharged home on nebulized
albuterol, atrovent, humibid, and theo/albuterol tablets. What is the
single most important intervention now?
a. Establish the correct diagnosis (i.e., obtain a
methacholine provocation test)
b. Carefully quiz the patient / family about compliance
issues
c. Instruct regarding proper MDI technique, spacer device,
home PEFR monitoring
d. Add inhaled corticosteroids
e. Check theo level and optimize the dose
Asthma "Mimics": Differential Diagnosis
•
•
•
Overlapping airway disorders
– Chronic bronchitis and emphysema
(COPD)
– Cystic fibrosis
– Bronchiectatic syndromes
Anatomical airway obstruction
– Foreign bodies
– Laryngospasm, edema
– Vocal chord paralysis
– Laryngotracheobronchomalacia
– Benign / malignant endobronchial tumors
Other conditions associated with wheezing
– Congestive heart failure ("cardiac
asthma")
– Pulmonary embolism
– Aspiration (gastroesophageal reflux)
– Loffler's syndrome
– Factitious asthma (vocal chord
dysfunction)
Variable Extrathoracic :
Fixed
Upper Airway Obstruction
Staging of COPD
Criteria
FEV1 % pred
% of all pts
Physician
Mortality
years
I
50%
+++
Generalist
Average
30% 1 yr,
Stage
II
III
35-49%
< 35%
++
+
Gen/Pulm Pulm/Gen
at 10
90% 10 yr
Intermediate
Intermediate
Yes
Occasionally
QOL
Good
Poor
Cost
Low
High
Need for ABGs?
No
Yes
Need for acute care?
Rarely
Often
Pre-op
risk
Moderate
Modified from: ATS statement. Low
Am J Respir Crit Care
Med 1995;152;S83.
High
Which of the following are the best
long term therapies for COPD to
improve outcomes? (Q10)
a. Inhalers (i.e. BDs)
b. Prednisone
c. Home O2
d. Smoking cessation
e. Pulmonary rehab
Other Imaging Modalities of the
Thorax
•
•
•
•
•
•
•
•
Computed Tomography (CT) chest
Ventilation/Perfusion scan (V/Q scan)
Pulmonary Angiogram (PA gram)
Fluoroscopy; Tomograms
Rib Films
MRI chest (i.e. vessels, heart), spine
Other cardiac studies (echo, thallium)
PET scan
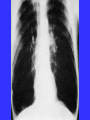
Restrictive Lung Disease:
Definition
• Restrictive lung diseases are a group of
conditions with a decreased ability to expand
lungs to full capacity (can’t get air in)
• Physiologically restrictive lung diseases are
defined by reduced total lung capacity, vital
capacity and functional residual capacity, often
with preserved air flow.
• Diagnostic Hallmark: a reduction in lung
volumes while airflow is preserved
• Oxygenation can be normal to decreased
• Severity of restriction is measured by total lung
capacity (TLC)
Classification of Restrictive Lung
Diseases
• Intra-parenchymal disease (lung tissue
is abnormal, e.g. pulmonary fibrosis)
• Extra-parenchymal disease (lung tissue
is normal) : altered/reduced thoracic
cage compliance
– chest wall deformities, kyphosis, scoliosis,
obesity, pleural effusions, ascites
– Neuromuscular disorders (“bellows”)
Clinical Evaluation for Restrictive
Lung Disease
• History: dyspnea; activity intolerance; cough;
orthopnea; reduced cough strength
• ROS: exposures; associated symptoms; comorbid disease
• Exam: decreased excursion; crackles; shallow
rapid respirations; clubbing
• Spirometry, Volumes, DLCO, O2
• Chest Radiographs
• Targeted Labs
Extra-parenchymal Disorders
The chest wall, pleura and respiratory muscles
are the components of respiratory pump
(“bellows”).
Disorders of these structures will cause lung
restriction and impair ventilatory function.
These are grouped as:
• Non-muscular diseases of the chest wall.
• Neuromuscular disorders.
Extra-parenchymal Disorders
• Diseases of the pleura & thoracic cage
decrease compliance of respiratory
system.
• There is reduction in lung volumes, VA.
• Hypoventilation with increased PaCO2
• Secondarily, atelectasis occurs leading to
V/Q mismatch hypoxemia.
Interstitial Lung Diseases
• Common clinical, physiologic, and
radiographic presentation
– Dyspnea, diffuse interstitial abnormalities
on CXR, and restriction on PFTs
• Heterogeneous group of disorders
• Affect the interstitium more than the
airways and alveoli
• Represent progressive inflammation
and/or scarring processes
Causes of ILD
•
•
•
•
Infectious (acute): viral, pcp
CHF (MS)
Neoplastic (lymphangitic ca)
Occupational/environment
– inorganic-asbestos, silica,
cwp
– organic-HP (allergic
alveolitis)
– Gases (NO), fumes
• Drugs
• Radiation
• Collagen-vascular disease
– RA, Scleroderma, Ank Spon
• Traumatic (fat emboli)
• Acute interstitial
pneumonitis
• Idiopathic pulmonary
fibrosis
• Eosinophilic granuloma (HX)
• Sarcoidosis
• LAM
• Veno-occlusive disease
• Other
Helpful Classification
Interstitial Lung Disease
Occupational
Asbestos
Silica
Coal
Organic
Iatrogenic
Granulomatous
Radiation
Sarcoidosis
Chemotherapy Hypersensitivity
Amiodarone
Methotrexate
CTD
Other
Idiopathic
Scleroderma
PM/DM
RA
SLE
Histiocytosis
LAM
IPF
NSIP
COP
AIP
RB-ILD
DIP
High Resolution Chest CT
• Ground glass
– Represents early
inflammation
– More steroid
responsive in certain
entities
• Fibrosis
– Chronic scarring
– Accompanied by
traction bronchiectasis
– Not steroid responsive
UIP
Slide courtesy of KO Leslie, MD.
HRCT findings: linear and reticular
opacities
• Intralobular interstitial thickening
– “fine reticular pattern” with lines of opacity separated by a few mmm
– Fine lacy or netlike appearance
– When seen in fibrosis, often seen in conjunction with dilated bronchioles
(“bronchiolectasis”)
– DDX:
• IPF
• Chronic hypersensitivity pneumonitis
• Pneumoconioses
• ILD: NSIP, DIP
• Lymphangitis carcinomatosis
• Pulmonary edema
• Pulmonary hemorrhage
• Pneumonia
• Alveolar proteinosis
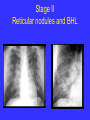
Figure 3-24
Stage II
Reticular nodules and BHL
Clinical vignette #6 (Q12)
50 y/o male sedentary heavy smoker, farmer with
progressive activity intolerance, fatigue; has birds
inside the home; BMI is 34; Exam is notable for
difficulty with speech and lying flat, but clear lungs;
spirometry shows mild restriction, normal ABGs, HRCT
chest & 2D echo. What is the next best step to clarify
the diagnosis?
a. Duplex LEs & V/Q scan
b. Cardiology consult for a heart cath (both R and L)
c. Bronch with BAL, possibly biopsy
d. Serologies for extrinsic allergic alveolitis (farmer’s lung
or psittacosis)
e. Sitting/supine spiro, resp muscle assessment
(MIP/MEP)
Lung Volume Measures
•
•
•
•
Vital capacity (VC)
Residual volume (RV)
Functional residual capacity (FRC)
Thoracic gas volume (TGV)
Lung Volumes in Disease
Neuromuscular Disorders
• Diseases affecting respiratory muscles, nerves,
or NMJ
• Muscular dystrophies, Guillain-Barre syndrome,
ALS / Polio, myasthenia gravis.
• Lead to dyspnea and respiratory failure.
• The progress of disease can be monitored by
FVC and blood gases.
• Treat the underlying cause or assist ventilation.
Pleural Diseases
• Pleural effusion can be acute or chronic.
• Pleural thickening / scarring / plaques– chronic
disease results in reduced compliance of the
lung and prevents expansion.
• If the disease is bilateral – may cause restrictive
lung disease.
• Treatment = underlying disease.
Diseases of the Chest Wall
• Deformity of thoracic cage such as kypho-scoliosis,
thoracoplasty.
• Scoliosis – lateral curvature of spine, kyphosis –
posterior curvature.
• Patients develop exertional dyspnea, rapid shallow
breathing.
• Later complications = Hypoxemia, hypercapnia and
cor-pulmonale.
• Cause of death is respiratory failure or intracurrent
pulmonary infection.
• Treatment is non-invasive or invasive chronic
ventilation.
Causes of Oxygenation Failure
•
•
•
•
Pneumonia syndromes
Acute lung injury / ARDS
Pulmonary edema, alveolar hemorrhage
Shock syndromes
Causes of Ventilatory Failure
•
•
•
•
Depressed MS
COPD; UAO
Weakness, NMS
Obesity / OSAS