Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
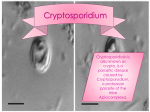
Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ Waterborne transmission of Cryptosporidium and Giardia: detection, surveillance and implications for public health D. Carmena MRC Clinical Sciences Centre, Faculty of Medicine, Imperial College, Hammersmith Hospital Campus, Du Cane Road, London W12 0NN, UK Protozoan enteroparasites of the genera Cryptosporidium and Giardia have emerged over the past decades as major waterborne pathogens. Both parasites are among the major causative agents of gastroenteritis and nutritional disorders in humans, with tens of millions of new cases occurring every year. Although cryptosporidiosis and giardiasis are normally self-limiting in immune-competent individuals, both are potential severe, life-threatening diseases in immunecompromised patients. Both pathogens are transmitted via the faecal-oral route, with the consumption of contaminated drinking water and use of recreational waterways being significant avenues for acquisition of infection. Because infected humans and animals can seed enormous amounts of the transmission stages of these parasites (Cryptosporidium oocysts and Giardia cysts), both micro-organisms are ubiquitous in the aquatic environment. In addition, (oo)cysts may remain viable for several months under a range of environmental conditions, their small size allow them to pass through conventional water plant filters, both are resistant to disinfectants at the concentrations and exposure times commonly used, and have low infectious doses in humans. Taken together, these data indicate that Cryptosporidium and Giardia represent a significant threat to public health. Indeed an increasing number of waterborne outbreaks of cryptosporidiosis and giardiasis have been reported worldwide, with most cases occurring in the USA and UK. This situation has become a major concern for water utilities and sanitary authorities that are responsible for providing safe drinking water supplies for human consumption. In this chapter relevant aspects of the biology and epidemiology of Cryptosporidium and Giardia from the aquatic environmental perspective are discussed, including pathology, treatment, transmission dynamics, detection, prevention and control measures. Keywords Cryptosporidium, Giardia, drinking water, recreational water, surveillance, public health, diarrhoea, zoonoses 1. Introduction Organisms of the genera Cryptosporidium and Giardia are protozoan parasites that infect the gastrointestinal tract of vertebrate animals, including mammals, birds, reptiles, amphibians and in the case of Cryptosporidium, fish. Species within these genera cause human cryptosporidiosis and giardiasis, which constitute the most common causes of protozoan diarrhoea and lead to considerable morbidity and mortality. About 200 million people have symptomatic giardiasis worldwide [1], with prevalences of 2–5% in industrialized countries and 20–30% in developing regions of Asia, Africa and Latin America. Transmission of cryptosporidiosis and giardiasis is typically associated with poor faecal-oral hygiene, being completed by any mechanism by which material contaminated with faeces containing infectious (oo)cysts can be swallowed by a susceptible host. Water and food are the most common transmission vehicles, although person-to-person or animal-to-person direct contacts are also important routes of infection. Immunecompromised individuals (i.e. AIDS and cancer patients, the very young or the elderly) are most at risk from the clinical consequences of these diseases. Because Cryptosporidium and Giardia infections cause considerable socio-economic burden in developing countries, both pathogens were included in the World Health Organization’s Neglected Disease Initiative in 2004 [2]. Cryptosporidium is currently classified within the phylum Apicomplexa, class Sporozoae, subclass Coccidia, order Eucoccidiida, suborder Eimeriina and family Cryptosporidiidae. To date at least 20 Cryptosporidium species have been recognized (see Table 1), among which eight (C. hominis, C. parvum, C. meleagridis, C. andersoni, C. suis, C. muris, C. canis and C. felis) have a zoonotic potential. Furthermore, nearly 61 Cryptosporidium genotypes with uncertain species status have also been reported [3,4]. Cryptosporidium was initially described as an intracellular parasite infecting the gastric glands of experimentally infected mice at the beginning of the last century. The first cases of human cryptosporidiosis were not reported until 1976, and soon afterwards the AIDS pandemic brought Cryptosporidium to the forefront as an opportunistic parasite infecting immune-compromised patients. However, its relevance in public health acquired a new dimension twenty years later, when Cryptosporidium began to be recognized as an important waterborne pathogen. The genus Giardia falls within the phylum Sarcomastigophora, class Zoomastigophora, order Diplomonadida and family Hexamitidae. It includes six valid species that inhabit the intestinal tracts of virtually all classes of vertebrates, with G. duodenalis (syn. G. intestinales, G. lamblia) being the only species found in humans (Table 2). Members of the G. duodenalis group should actually be regarded as a species complex with little morphological variation among them, yet can be assigned to at least seven genotypes or ‘assemblages’ (A-G) [5,6]. Giardia has been known since the seventeenth century work by Antony van Leeuwenhoek, although for most of this time this protozoa has been considered a harmless intestinal commensal, primarily because the parasite was identified in asymptomatic individuals. ©FORMATEX 2010 3 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ It was not until 1987 that the pathogenic nature of Giardia was definitively confirmed in a study of infection in human volunteers [7]. As in the case of Cryptosporidium, Giardia is also an important cause of waterborne illness. Table 1 Cryptosporidium species (adapted from references [4], [8] and [9]). Species Main host C. andersoni C. baileyi C. bovis C. canis C. fayeri C. felis C. fragile C. galli C. hominis C. macropodum C. meleagridis C. molnari C. muris C. parvum C. ryanae C. scophthalmi C. serpentis C. suis C. varanii C. wrairi Cattle Chicken Cattle Dog Kangaroo Cat Toad Chicken Humans Kangaroo Turkey Marine fish Mouse Mouse Cattle Cultured fish Snake Pig Lizard Guinea pig Reported infections Yes No No Yes No Yes No No Yes No Yes No Yes Yes No No No Yes No No in human Reported in waterborne outbreaks No No No No No No No No Yes No Yes No No Yes No No No No No No Reported in water (nonoutbreak conditions) Yes Yes No Yes No Yes No No Yes No Yes No Yes Yes No No No Yes No No 2. Life cycle of Cryptosporidium and Giardia Members of the genus Cryptosporidium are able to infect and multiply in a wide range of vertebrate hosts, including humans, mice, rats, cats, dogs, sheep, cattle, horses, pigs, poultry, birds, reptiles, and fish. Cryptosporidium is an obligate intracellular parasite that requires a single host (monoxenous) to complete its life cycle. Infected hosts shed oocysts, the infective stage of the parasite, contaminating pastures, soil and water. Once the oocyst is accidentally ingested by a new host, exposure to stomach acid, bile salts and host metabolic temperature promotes thinning of the oocyst wall (excystation), resulting in release of four motile sporozoites into the small intestine (Fig 1A). This requires different factors derived from both the parasite and the host cell, including expression of receptors on the surface of oocysts, trypsin and other enzymes for sporozoite excystation [10]. Released sporozoites contain secretary apical organelles required for adhesion, penetration and inclusion in host epithelial cells lining the luminal surfaces of the digestive and respiratory tracts. After this process the parasite nestles itself within a parasitophorous vacuole (intracellular but extracytoplasmatic) where it is protected from the hostile gut environment and is supplied by the host cell with energy and nutrients. The sporozoites undergo then asexual reproduction cycle (merogony), involving differentiation and, sequentially, trophozoite, Type I meront and merozoite production. Some of these merozoites can cause autoinfection by attaching and invading neighbouring epithelial cells (perpetuating the asexual cycle) whereas others become Type II meronts, which contain 4 Type II merozoites. Released Type II merozoites infect adjacent host epithelial cells and differentiate into either macrogamonts or microgamonts, initiating the parasite’s sexual phase (gametogony). Microgamonts differentiate into microgametes, which after being released can penetrate and fertilise the macrogamonts, producing a zygote. Following meiosis, the zygote differentiates into four naked sporozoites that then develop into cysts of two types: 20% of oocysts have thin walls, enabling autoinfection of the host by rupturing and releasing new sporozoites. The remaining thick-walled oocysts (environmentally-resistant and immediately infective) are shed in the faeces, usually in large numbers (Fig 1B-D). A new generation of parasites can develop and mature in as little as 12–14 hours. Giardia has a simple, non-invasive life cycle that involves two well-differentiated forms: the trophozoite (proliferative stage) and the cyst (resilient to environmental stressors and infective stage). Cysts are passed in the faeces of infected hosts, contaminating food, soil and water. Fortuitous ingestion of cysts by a new susceptible host leads to the release of the trophozoites after exposure to stomach acid and bile salts. Trophozoites are teardrop shaped, binucleate, with four pairs of flagella and have a ventral sucking disc that allow them to adhere and colonise the brush border of the intestinal epithelium (Fig 2A). The trophozoites absorb their nutrients by pinocytosis from the lumen of the small intestine and undergo asexual replication through longitudinal binary fission. As faeces enter the colon and begin to 4 ©FORMATEX 2010 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ dehydrate, the trophozoite-to-cyst transformation (encystation) occurs, being the newly formed and readily infective cysts (Fig 2B-D) excreted with the faeces to re-initiate the cycle. Although Giardia is considered to be strictly asexual, recent evidence suggests that exchange of genetic material may take place during the excystation and encystation processes in G. duodenalis [11]. Table 2 Giardia species and assemblages (adapted from references [5] and [9]). Species Main host G. duodenalis G. agilis G. muris G. ardeae G. psittaci G. microti Mammals Amphibians Rodents Birds Birds Rodents Reported infections Yes No No No No No Assemblages A (= G. duodenalis) B (= G. enterica) C/D (= G. canis) E (= G. bovis) F (= G. cati) G (= G. simondi) Mammals Mammals Dog Cattle Cat Rat Yes Yes No No No No in human Reported in waterborne outbreaks Yes No No No No No Reported in water (nonoutbreak conditions) Yes No No No No No Yes No No No No No Yes Yes No No No No 3. Cryptosporidium and Giardia infections in humans 3.1 Pathology and clinical manifestations At least eight Cryptosporidium species (see Table 1) and two Cryptosporidium genotypes (cervine and monkey) have been found to infect humans, with C. hominis and C. parvum accounting for more than 90% of the cases [12]. The main site of the infection is the small intestine (jejunum and ileum), although the parasite may also spread throughout the gastrointestinal and respiratory tracts. Invasion of host cells is restricted to the luminal border and leads to loss of the surface epithelium, causing villous disruption and atrophy, blunting and crypt cell hyperplasia, mononuclear cell infiltration in the lamina propia and eventually enterocyte death [13]. Tissue damage triggers the immunological and inflammatory responses of the host, inducing the recruitment of prostaglandin-secreting inflammatory cells. Crypt cells and prostaglandin in turn stimulate chloride ion secretion and inhibits NaCl absorption. As a consequence of the impaired intestinal absorption of fluids and nutrients and the disruption in the normal ion flux, secretory diarrhoea occurs. Extra-gastrointestinal cryptosporidiosis has been reported in both immune-competent individuals and immunecompromised patients, affecting pancreas, liver and bile ducts. Tracheo-bronchial involvement and even sinusitis have been described in severe cases. The precise pathogenic mechanisms of cryptosporidiosis have not yet been fully elucidated, although in vitro experiments using Caco-2 cells suggest that enterotoxins may be involved in the process [14]. The duration and severity of cryptosporidiosis in humans is directly related to the immunological status of the host, with CD4+ T lymphocyte counts and gamma interferon levels playing an important role in fighting the infection [15]. In immune-competent individuals the infection and colonization of the pathogen within the intestinal tract can be asymptomatic or develop illness causing an acute self-limiting gastroenteritis with a median duration of 9–15 days. Children (particularly those under two years old) are most frequently affected, the disease being associated with impaired growth, malnutrition and significant morbidity and mortality in developing countries. The major symptom is watery diarrhoea associated with abdominal pain, anorexia, weight loss, nausea, fatigue and low-grade fever [16]. In immune-compromised people including those with haematological malignancies, AIDS patients with CD4+ lymphocyte counts of <50/mm3 and patients undergoing cancer chemotherapy or chemo-suppressive treatment associated with organ transplantation, the intestinal infection is chronic or intractable and can affect atypical and extra-intestinal sites. G. duodenalis is the only specie within the genus Giardia able to infect humans. Giardia infection is not invasive and often asymptomatic: as many as 50% to 75% of infected persons may not develop any symptoms of the disease [17]. The main site of the infection is the small intestine (jejunum and duodenum), being extra-intestinal invasion infrequent. The pathogenesis of giardiasis is not completely understood but recent evidence suggests that the parasite’s trophozoites trigger a multifactorial pathophysiological process involving damage to the intestinal brush border and mucosa, induction of the host immune and inflammatory responses, impairment in pancreatic function and alteration of duodenal flora [18]. Cases of urticaria and reactive arthritis have also been associated to Giardia infections. In addition, altered epithelial permeability caused by cytopathic molecules of parasitic origin, disruption of tight junction-associated protein ©FORMATEX 2010 5 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ zonula occludin-1 (ZO-1) and apoptosis leads to both digestive and absorptive changes that induce acute or chronic diarrhoea [19]. Other common symptoms include abdominal pain, steatorrhea, bloating, flatulence and weight loss, with nausea, vomiting and fever being less frequent. Similarly to Cryptosporidium infection, the duration and severity of giardiasis may vary depending upon the immunological, developmental and nutritional status of the host and the parasite strain infectivity and virulence. In immune-competent individuals giardiasis is short-lasting and resolves spontaneously in 1–4 weeks with symptoms lasting for only 3–4 days. Immune-compromised individuals are more susceptible to symptomatic infection and have more severe and prolonged disease, lasting even for months if treatment is not provided. A B C D Fig. 1 Cryptosporidium parvum oocysts are spheroidal objects, 4 to 6 microns in diameter, and may contain as many as 4 banana shaped sporozoites. A) Scanning electron micrograph of a human intestinal biopsy infected with C. parvum. B) Nomarski differential interference contrast microscopy image. C) Immunofluorescence microscopy image. D) Immunofluorescence microscopy image with DAPI staining, specific for nucleic acids. DAPI stained sporozoites appear as intense bright blue spots. Figures B, C and D correspond to the same field of view. Image credits: M.V. McCrossan EM Unit, London School of Hygiene & Tropical Medicine, UK (image A) and H.D.A Lindquist, U.S. EPA (images B, C and D) 3.2 Treatment Despite recognition of Cryptosporidium and Giardia as important human pathogens, there are a relatively limited number of agents available for chemotherapeutical purposes, and more research is required in order to identify existing or new compounds that may be effective against cryptosporidiosis and giardiasis. To date nitazoxanide is the only drug licensed in the United States for treating cryptosporidiosis in immune-competent individuals, being able to reduce the duration of diarrhoea and oocyst shedding in several clinical trials (revised in reference [20]). Nitazoxanide has also been demonstrated effective in well controlled clinical trials with AIDS patients, achieving eradication of the parasite in up to 62% of the treated people. A dose of 2-g per day during 12 weeks is recommended for treating this type of patient. A wider spectrum of compounds is currently available for the treatment of giardiasis. The drugs of choice are the derivatives of nitroimidazol, including metronidazole, tinidazole and ornidazole, all well known inhibitors of nucleic acid synthesis. Metronidazole at doses of 250 mg two to three times a day for 7–10 consecutive days has a median efficacy over 90%, but some severe side effects such as pancreatitis, central nervous system toxicity and potential carcinogenesis have been reported. Tinidazole at a 2-g single dose in adults achieves levels of efficacy ranging from 80% to 100% and reduce greatly the adverse side effects of metronidazole. Benzimidazole carbamates including mebendazole and albendazole have also been successfully used for the treatment of giardiasis with rates of efficacy from 62% to 95%, and also other drugs such as quinacrine, furazolidone and paromomycin [21]. 6 ©FORMATEX 2010 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ 4. Cryptosporidium and Giardia transmission Cryptosporidium and Giardia can be transmitted to humans through any mechanism by which material contaminated with infectious (oo)cysts is swallowed by a susceptible host. Both parasites are maintained in a variety of transmission cycles, including human-to-human, animal-to-human, and environmental transmission involving appropriate vehicles, mainly water and food. Whatever the case, it is of capital importance to understand the host range of different species and strains/genotypes, how they are maintained in nature and their zoonotic potential in domestic and wildlife animals. Experimental cross-transmission studies have been carried out in order to investigate the host specificity of a given strain/genotype, but very often the relevance of the obtained results is limited by incomplete molecular characterization of the source (oo)cysts, uncertainty about their viability or the parasite-free status of the challenged hosts and the use of high doses of (oo)cysts that are unlikely to represent a natural infection [19]. A B C D Fig. 2 Giardia duodenalis cysts are ovoid or ellipsoidal objects, 8 to 14 microns in length, and may contain as many as 4 nuclei and structures from their trophozoites. A) Transmission electron micrograph of trophozoites infecting the epithelial surface of the intestine. B) Nomarski differential interference contrast microscopy image. C) Immunofluorescence microscopy image. D) Immunofluorescence microscopy image with DAPI staining, specific for nucleic acids. DAPI stained nuclei appear as intense bright blue spots. Figures B, C and D correspond to the same field of view. Image credits: Reference [22], with kind permission of Springer Science and Business Media (image A) and H.D.A. Lindquist, U.S. EPA (images B, C and D). 4.1 Direct transmission between humans Person-to-person transmission is an important route of spread of Cryptosporidium and Giardia, being usually associated with poor hygiene and sanitation. Thus, cryptosporidiosis and giardiasis are common in day-care centres, with diaperchanging and mouthing behaviour being important causes of infection. Transmission of these diseases are also frequent in nosocomial settings including hospitals, nursing homes and other institutions, where both transmission from patients to health care staff and patient-to-patient transmission have been reported. Cryptosporidium has also been discovered in both sputum and vomits, and these body fluids may prove to be additional vehicles of transmission [23]. Transmission can also occur through certain types of sexual contact. 4.2 Transmission between animals and humans Cryptosporidium and Giardia have been identified in numerous mammalian (including livestock and house pets), avian, reptilian, and piscine hosts worldwide [24,25]. Because the extent of cross-transmission to humans appears to be genotype-dependent, molecular characterization of animal isolates is crucial to evaluate their epidemiological relevance. Both the bovine genotype of C. parvum, and to a much lesser extent C. andersoni have been demonstrated to be zoonotic (see Table 1). Because newborn calves are predominantly infected with C. parvum whereas older animals are infected primarily with C. andersoni, young animals are the principal source of zoonotic C. parvum. Transmission may ©FORMATEX 2010 7 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ happen either by direct contact with infected young cattle or by consumption of livestock-contaminated drinking water [26]. Indeed cattle have been clearly implicated as the source of at least one waterborne outbreak [27]. C. parvum infection is less common in sheep and goats, although direct transmission of C. parvum from lambs to children and handlers have been reported [28]. Although evidence of contamination of water supplies by Cryptosporidium from infections in sheep and goats is limited, this possibility should not be ruled out completely. Regarding companion animals, dogs and cats do not seem to be important zoonotic reservoirs of Cryptosporidium, as they are most commonly infected with their host-adapted species C. canis and C. felis, respectively [29]. These species, together with C. suis and C muris may cause sporadic infections in humans, most likely through direct contact. Genotypes of Giardia of assemblage A and to a lesser extent of assemblage B pose the greatest zoonotic risk (see Table 2). In cattle the livestock genotype (assemblage E) occurs most frequently, although a small proportion of animals may harbour genotypes of assemblage A [30]. In any case the potential risk of zoonotic transmission of Giardia infections between cattle and humans is probably minimal. In sheep and goats Giardia isolates of assemblage E are also predominant, with zoonotic assemblages A and B being detected in 30% of infected animals [31]. Transmission to humans can occur either directly or by environmental contamination, with few reports proposing sheep and goats as sources of Giardia contamination of water supplies. Similarly, dogs and cats are both susceptible to infection with zoonotic genotypes of Giardia [32], but the chances of a contamination event from a dog or cat leading to a waterborne outbreak seem unlikely [30]. Wildlife in water catchments have often been identified as potential sources of Cryptosporidium and Giardia infections in humans. Beavers have being involved in a number of Giardia waterborne outbreaks, although recent research has evidenced that beavers can actually become infected with Giardia of human origin from contaminated municipal water supplies. Besides, C. parvum can be mechanically passed to water by birds in faeces, suggesting that birds, particularly waterfowl, can serve both as reservoir host and vectors [33]. Evidence from the limited number of molecular studies conducted to date support the idea that wildlife genotypes are host-specific, non-human adapted and do not seem to represent a major public health concern. 4.3 Transmission through water Because infected animals (and humans) can shed massive amount of infective (oo)cysts to the environment (see subsection 5.1) Cryptosporidium and Giardia are ubiquitous. In aquatic environments both pathogens have been isolated worldwide from rivers, lakes or reservoirs used as source waters for human consumption or recreation, and also from treated drinking water supplies and recreational waters facilities, including swimming pools and water parks. In addition, (oo)cysts may reach groundwater supplies through infiltration of contaminated surfaces waters. Commonly reported (oo)cyst concentrations are in the range of 0.01–150 per litre, but higher concentrations have been found in agricultural run-off and urban wastewater effluents. Not surprisingly, Cryptosporidium and Giardia have been frequently associated with waterborne illness in the last 30 years. The most remarkable episode happened in 1993, when a massive Cryptosporidium waterborne outbreak was registered in Milwaukee, Wisconsin (USA), affecting an estimated 403,000 people including 4,400 people hospitalized and more than 100 deaths [34]. The total cost of outbreak-associated illness was estimated at $96.2 million, including $31.7 million in medical costs and $64.6 million in productivity losses [35]. Since then at least 165 Cryptosporidium waterborne outbreaks have been recorded in developed countries, with North American and European outbreaks accounting for the vast majority [36,37,38]. To date only three Cryptosporidium species (C. hominis, C. parvum and C. meleagridis) have been isolated from water-related outbreaks, although several others have been reported in surface waters under non-outbreak conditions (see Table 1). Giardia is more frequently found in surface waters than Cryptosporidium, and it has been associated with at least 132 waterborne outbreaks worldwide [36]; the most important ocurred in Norway in 2004 and affected more than 1,500 persons [39]. Generally most human infections are due to the consumption of water from unfiltered surface water sources, shallow wells and during water recreational activities. Giardia has been the most commonly identified pathogen in waterborne outbreaks reported in the United States since 1971, with almost 28,000 cases during the period 1965 to 1996 [21]. Despite this little is known about the Giardia assemblages present in the aquatic environment, due to the scarcity of genotyping surveys conducted. Although most of the waterborne outbreaks of cryptosporidiosis and giardiasis have been associated with contamination of municipal drinking water systems, exposure to contaminated recreational waters (i.e. swimming and wading pools) were also significant sources of infection in humans. Contamination of the source water may be caused by a wide range of events including the dispersion and transportation of (oo)cysts after heavy rainfall or melting snow, sewage contamination of surface water and wells, inadequate treatment practices and deficiencies in water treatment systems or combination of these factors [40]. The relative significance of these contamination sources may differ depending on the particular characteristics of each water catchment and supply network. 4.4 Transmission through food Foodborne outbreaks of cryptosporidiosis and giardiasis are less frequently reported in the literature than waterborne outbreaks, probably due the lower evidence of parasitic infection and the lack of standardized detection methods [41]. 8 ©FORMATEX 2010 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ Raw milk and meat, farm-made apple cider, fermented milk, salads and raw vegetables are among the food products where the presence of (oo)cysts has been documented. Food can be contaminated by infected food handlers, irrigation with contaminated water or manure. Although there is evidence of zoonotic transmission in certain cases, more research (particularly genotyping studies) is needed to correctly assess the public health relevance of these findings. In USA approximately 10% of all cryptosporidiosis and giardiasis cases are thought to be foodborne. 5. Cryptosporidium and Giardia are particularly suited for waterborne transmission (Oo)cysts of Cryptosporidium and Giardia share a number of biochemical and physical features that make them especially robust to a wide range of ecological stressors and favour their successful dispersal in the aquatic environment. 5.1 (Oo)cysts are shedding in high numbers Both Cryptosporidium and Giardia have adopted high fecundity rates as adaptative strategy to enhance their probabilities of survival and transmission. Cattle and humans per se are regarded as the most important reservoirs of Cryptosporidium and Giardia infection in humans, respectively. Mean intensity of infection by Cryptosporidium in cattle has been estimated to be in the range between 2–1,000 oocysts/g of faeces [42], with maximum shedding of 106-8 oocysts/g of faeces at the peak of the infection. Considering that cattle may shed up to 40 kg of faeces a day and that oocyst excretion last 3–12 days in infected animals, these data clearly illustrate the huge impact of cattle on the load of infective Cryptosporidium to the environment, including watersheds. Humans are also major contributors to the environmental (oo)cyst pool that causes contamination of surface waters. Therefore, infected persons can shed up to 105-7 Cryptosporidium oocysts/g of faeces during infection and up to 109 Giardia cysts in a single day. 5.2 Persistence in the aquatic environment Cryptosporidium oocysts and Giardia cysts can survive for six months and 2–3 months, respectively, suspended in natural surface waters [9]. The survival of both pathogens in the aquatic environment is significantly affected by temperature, with (oo)cysts infectivity decreasing as temperature increases. In reservoir waters at 22 °C and 30 °C, 45 and 11 days, respectively, were estimated for a 2 log reduction of C. parvum infectious oocysts assessed by cell culture [43]. Similarly, survival of Giardia cysts declines to less than a month at 21°C. (Oo)cysts are extremely susceptible to temperatures above 37 °C and heat-shocks, with complete loss of infectivity after incubation at 64 °C for 5 min in the case of Cryptosporidium and 54 °C for 10 min in the case of Giardia. In addition, Cryptosporidium oocysts are able to retain infectivity after freezing at –10 °C for up to 168 h, but not after 24 h at –20 °C. Giardia cysts are more sensitive to extreme low temperatures and can not survive freezing conditions. Desiccation, freeze-thaw cycles and solar radiation are other environmental stresses that can threat the viability and infectivity of (oo)cysts [44]. 5.3 Small size Because of their small size (see Figs 1B and 2B), Cryptosporidium oocysts and Giardia cysts have very low specific gravities, with settling velocities in water ranging from 0.03 to 5-10 m/day [45]. Some authors have proposed that sedimentation rates are significantly increased when (oo)cysts attach to other suspended particles, whereas others found that this is not the case and (oo)cysts remain free for considerable periods of time, a fact that facilitates their transport and diffusion in a water body [44]. While sedimentation of (oo)cysts may remove them temporarily from host ingestion, turbulence generated by underflow events can result in sediment re-suspension, with deposited (oo)cysts re-joining the pool of suspended particles. These characteristics have important implications for the water industry, as (oo)cysts removal by sedimentation would be insignificant even after long periods of reservoir storage, and (oo)cysts can pass through most conventional filters used in water treatment facilities. Even well-designed and operated water treatment systems allow the passage of infectious (oo)cysts, which might expose the community to outbreaks of giardiasis and cryptosporidiosis [2]. 5.4 Resistance to chemical disinfection Both Cryptosporidium and Giardia (particularly the former) are resistant to chlorine-based disinfectants at the concentrations and exposure times commonly used in the water industry [46], and using increased chlorine concentrations may lead to generation of toxic disinfection by-products such as trihalomethanes or nitrite. In practice this means that water treatments based only on chlorination are not sufficient to inactivate potential infective (oo)cysts. Effective physical removal or inactivation of Cryptosporidium and Giardia requires the right combination of water filtration and disinfection (including ozonation and ultraviolet irradiation) procedures operated under optimum conditions [21,40]. ©FORMATEX 2010 9 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ 5.5 High infectivity Exposure to Cryptosporidium and Giardia will result in infection or illness depending on a number of pathogen-, hostand environment-derived factors, including the strain genotype of the parasite involved and the susceptibility and immune status of the host. Whatever the case the infectivity of (oo)cysts is considered high: as little as 10–30 Cryptosporidium oocysts have been proven to induce infection in 20–40% of human volunteers, with ID50 in the range of 9–1,042 oocysts [47–49]. Similarly, only 10 Giardia cysts were sufficient to produce infection in another two human volunteers. The median infectious dose for Giardia has been estimated to be in the range of 25–100 cysts [9]. Although it is unclear if the number of (oo)cysts generally present in drinking water constitute a sufficient dose to cause illness in humans, research using mathematical models (see also section 7) has demonstrated that some fraction of the population could become infected with a single Cryptosporidium oocyst [40]. 6. Detection of Cryptosporidium and Giardia in water Due to their small size and frequently low number in water samples, detection of Cryptosporidium oocysts and Giardia cysts is difficult and requires time consuming and labour intensive work and also well trained and experienced personnel. Under these circumstances, optimized and standardized techniques for (oo)cysts monitoring in surface and drinking waters are essential. Current recommended and most common used methods are based on four sequential steps: i) mechanical filtration of small-large volumes (1–1,000 L) of water to maximize (oo)cysts recovery and ensure a representative sample; ii) purification and concentration of (oo)cysts by immunomagnetic separation (IMS); iii) staining with specific fluorescent antibodies (FA); and iv) enumeration using fluorescence (see Figs 1C and 2C) and differential interference contrast microscopy [50]. Other techniques that can be also used for (oo)cysts purification purposes include density gradient, saturated-salt solution centrifugation, continuous flow centrifugation and flow cytometry with cell sorting [51]. 6.1 Spatial and temporal distribution of (oo)cysts The environmental load of Cryptosporidium oocysts and Giardia cysts in surface water bodies is discontinuous in nature and depends on factors such as livestock contamination (particularly during the periods of calving and lambing), agricultural practices, sewage contamination, heavy rainfall and flooding or snow and ice melting. However, operational deficiencies and sub-optimal processes in water treatment facilities rather than meteorological-related events account for the majority of the waterborne outbreaks reported. Taken together, these data indicate clearly that spatial and temporal variations in the (oo)cysts distribution are expected in both untreated and finished waters, with (oo)cysts contents fluctuating in a spiking pattern. This fact needs to be considered in the sampling design of studies intended to assess the presence of Cryptosporidium and Giardia in water samples. Indeed, extensive monitoring programs have shown that prolonged periods with zero or very low (oo)cysts counts are followed by peaks of high counts but short duration [40]. Thus, spot sampling tends to underestimate the real prevalence of these pathogens in water, and more importantly, tends also to miss those ‘rare but all important’ high count samples. In fact, as many as 10 samples may be required to describe the range of (oo)cysts concentrations that a community is experiencing in its water supply [52]. In a simulated model for a waterborne outbreak of cryptosporidiosis, nine out of every ten 100-L spot samples underestimated the risk to the population to some degree, with 33% containing no oocysts [53]. According to this model, there was a one in three chance of a 100-l spot sample suggesting zero risk when in fact there was an outbreak across the population. 6.2 Recovery efficiency (Oo)cysts recovery levels can be influenced by a large number of factors, including the physicochemical and organic properties or the water matrix (turbidity, pH, inorganic compounds, clays and suspended algae), the age and condition of the (oo)cysts, the type of cartridge/capsule filter and the quality of the reagents employed. As a consequence, every method used for the detection of (oo)cysts in water samples must be appropriately validated and its initial precision and recovery efficiency determined in spiking trials in the laboratory with known amounts of (oo)cysts [54]. To estimate the actual concentration of (oo)cysts in an environmental sample, the (oo)cyst counts need to be corrected for the recovery efficiency of the used method. This is complicated by the fact that the recovery efficiency can vary between samples. Typical (oo)cysts recoveries based on the filtration/IMS/FA system range between 10–70% [54–57], although recent improvements in this methodology have allowed values up to 80% [58]. Reported recovery levels for Giardia cysts usually exceed those for Cryptosporidium oocysts. 6.3 Viability and infectivity From a public health perspective, the relevance of the detection of (oo)cysts in a water sample will depend on their viability and infectivity, as an (oo)cyst that is apparently intact and metabolically sound but incapable of excystation is of no more importance that a dead (oo)cyst . The term ‘viable’ has been defined as ‘capable of reproducing under 10 ©FORMATEX 2010 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ appropriate conditions’ [59], although other authors have suggested that viability should be better used to reflect the (oo)cyst metabolic activity and integrity [60]. Thus, a viable (oo)cyst can be infective or non-infective, and if noninfective is of no public health concern. Viability has been widely assessed by microscopy-based methods reliant on vital dye uptake such as propidium iodine, 4’6-diamidino-2-phenyl indole (DAPI, see Figs 1D and 2D), and SYTO-59, but they have proven to be relatively unreliable, tend to overestimate the infective potential of (oo)cysts and differentiation of (oo)cysts from debris and/or other micro-organisms may be difficult [51]. Similar problems have been found using in vivo excystation assays (as (oo)cysts that are capable of excysting might not be capable of initiating infection) and also with fluorescent in situ hybridization techniques. Therefore, results obtained with these methods must be interpreted with caution, particularly if risk assessment or treatment evaluation is under consideration [60]. To date infectivity studies in animal models or humans volunteers and cell culture assays (including human epithelial and intestinal cell lines) are regarded as the most consistent approaches to assess (oo)cysts viability and/or infectivity. Thus infectivity assays remain the gold standard as they are the only method that provides definitive evidence of the (oo)cyst capability to initiate and cause infection in an specific host. Cell culture assays (often coupled to PCR, reverse transcription PCR or immunofluorescence) offer equivalent results to those from infectivity studies when (oo)cysts not exposed to disinfectants or environmental stressors are used. However both methods are costly, labour-intensive, timeconsuming and require large numbers of (oo)cysts for analyses (particularly the infectivity assays), features that make them unsuitable for routine testing of environmental samples [40,51,60]. 6.4 Molecular characterization The most commonly found Cryptosporidium species and genotypes in surface and waste waters include the two major Cryptosporidium pathogens of humans (C. parvum and C. hominis) in addition to the cattle species C. andersoni, whereas only zoonotic Giardia assemblages A and B have been reported to date [9]. However, infected livestock, wildlife and migratory animals are also important contributors to the (oo)cysts pool found in surface waters, although many of them are not pathogenic to humans (see sub-sections 4.2 and 4.3) and consequently do not represent a public health threat. Thus, molecular characterization of Cryptosporidium and Giardia isolates from water samples at the species/assemblage level is essential to understand not only their potential infectivity to humans, but also their environmental transmission. Additional typing to the subspecies level to describe variation between Cryptosporidium species and Giardia assemblages can provide further information to address contamination source and disease tracking during outbreaks [26,41]. A wide range of Cryptosporidium target genes are available for amplification-based techniques, including nuclear small subunit ribosomal DNA (18S rDNA), heat shock protein 70 (Hsp70), Cryptosporidium oocyst wall protein (COWP), internal transcribed spacer 1 and 2 (ITS1-2), actin, β-tubulin, glycoprotein 60 (Gp60), and micro- and mini-satellite multilocus repeats, with a sensitivity as low as a single oocyst [26,61]. For instance, PCR-restriction fragment length polymorphism (PCR-RFLP) of the COWP gene allows differentiation among C. parvum, C. hominis and C. wrairi, whereas PCR-RFLP of the 18S rDNA discriminates among C. parvum, C. muris and C baileyi [61]. On the other hand, Gp60 sequence and micro- and mini-satellite repeats are used to cluster Cryptosporidium strains into subtypes [41,51]. For Giardia, PCR amplification of gene markers such as 18S rDNA, glutamate dehydrogenase (GDH), triose phosphate isomerase (TPI), β-giardin and elongation factor 1α (EF1α) has been used for speciation and assemblage/sub-assembalge determination [26,61]. 7. Surveillance and control measures Waterborne cryptosporidiosis and giardiasis have become a major concern for the sanitary authorities and the water industry responsible for providing safe drinking water supplies for human consumption. Different strategies are available for the surveillance of Cryptosporidium oocysts and Giardia cysts in raw and finished waters. Thus, current regulations of countries such as USA [62], Canada [63], Australia and New Zealand [64] establish that water treatment facilities must comply with specific goals for treatment performance, including (oo)cysts removal for filter systems, turbidity monitoring and estimation of pathogen inactivation. None of the regulatory agencies of these countries recommend (oo)cysts monitoring on the basis that current methods for the detection of (oo)cysts suffer from low recovery rates, do not provide any information on their viability or human infectivity and there is a lag time between sample collection and test result. On the contrary, continuous Cryptosporidium oocysts monitoring is compulsory in England and Wales [65] and Northern Ireland [66]. Regulations in these countries set a treatment standard of an average of less than one oocyst in 10 L of water supplied from a water treatment facility. The standard does not take into account different species of Cryptosporidium, nor whether any oocysts detected are viable or infective to humans. In addition, detection of Cryptosporidium oocysts at any level above one per 10 L would constitute a criminal offence. Because this approach was not set on human health criteria, its usefulness and cost-effectiveness have been questioned by some authors [67]. Based on (oo)cysts measurements made before and after detected waterborne outbreaks of cryptosporidiosis and giardiasis, some researchers have estimated (oo)cysts levels that, if exceeded, may lead the possibility of an outbreak. Therefore, concentrations of 10–30 oocysts and 3–5 cysts per 100 L of treated water have been proposed as ‘action ©FORMATEX 2010 11 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ levels’ for Cryptosporidium and Giardia, respectively [68,69]. Authors recommended that a single sample containing (oo)cysts at concentrations above the action threshold should be evaluated immediately in order to initiate appropriate action without delay. However, as discussed before, action levels are hampered by the highly variable sensitivities of the methods available for (oo)cysts detection, so obtaining reliable counts may be a difficult task. Integrated risk models based on mathematical and statistical methods have been proven to be useful tools to assess the probability of waterborne cryptosporidiosis and giardiasis outbreaks. These models take into account environmental (source, concentration, distribution and viability/infectivity of pathogens in water), technical (water treatment efficiency, performance of detection methods), medical (virulence, dose-response relationship, immune status of the population), and exposure factors, considering also the natural variation and uncertainties associated to some of those variables [70–72]. Prevention measures are by far the most practical approach to reduce the risk of cryptosporidiosis and giardiasis, as demonstrated during an epidemic of foot and mouth disease in livestock in England and Wales in 2001: limiting visitors to the countryside to reduce direct and indirect exposure to livestock resulted in a marked attenuation (81.8%) of Cryptosporidium reports as compared to the previous year [73]. Because contamination of water supplies is a major source of human infection, implementation of measures to decrease the spread of (oo)cysts in the environment and to improve the performance of the water treatment processes are critical. To achieve this goal the following aspects need consideration: a) Good farming and agricultural practices. Management strategies should be designed to minimize direct livestock contamination of surface waters. This include adequate housing, thorough cleaning, disinfection and drying of animal pens, appropriate removal or inactivation (i.e. composting) of fresh manure, prevention of runoff from animal housing, isolation of ill animals (particularly calves), and implementation of measures that reduce transmission between animals (i.e reducing stocking density). b) Water catchment protection. Practices such as restricting access of livestock to water bodies by fencing, access ramps, rotational grazing, or off-site watering, and active control of herds to prevent extensive surface water contact may significantly reduce (oo)cysts contamination. Grass or riparian filter strips acting as buffer zones have also been proven effective in reducing (oo)cysts from overland flow generated during low or moderate precipitation [12]. Intake points from surface water supplies should be kept well away from other contamination sources, such as sewer overflows or discharges of untreated and treated sewage. c) Improved detection methods. New, practical and cost-effective technologies with higher and more consistent sensitivities and with the ability to differentiate species and (oo)cysts viability/infectivity are needed to obtain reliable (oo)cysts concentration measures in water samples and to assess the risk of human infection. d) Optimized water treatment. Water treatment plants should be operated in accordance with good practice at all times, monitoring the performance of the system and introducing corrective measures in those circumstances when the treatment is compromised. Additional second-line treatments including membrane filtration, UV irradiation and ozonization can further improve the efficiency of the system in removing/inactivating (oo)cysts. Acknowledgements This work was partially supported by a grant from the Department of Health, Basque Government, Spain (Exp. No. 2007111002). The author is very grateful to Richard G.E. Chamberlain for his advice with the English language editing. References [1] World Health Organization. Guidelines for drinking-water quality. Vol 1 Recommendations. Geneva, World health Organization; 2006. [2] Savioli L, Smith H, Thompson A. Giardia and Cryptosporidium join the ‘Neglected Disease Initiative’. Trends in Parasitology. 2006;22:203-208. [3] Fayer R. Taxonomy and species delimitation in Cryptosporidium. Experimental Parasitology. 2010;124:90-97. [4] Plutzer J, Karanis P. Genetic polymorphism in Cryptosporidium species: an update. Veterinary Parasitology. 2009;12:187-199. [5] Monis PT, Cacciò SM, Thompson RC. Variation in Giardia: towards a taxonomic revision of the genus. Trends in Parasitology. 2009;25:93-100. [6] Cacciò SM, Ryan U. Molecular epidemiology of giardiasis. Molecular and Biochemical Parasitology. 2008;160:75-80. [7] Nash TE, Herrington DA, Losonsky GA, Levine MM. Experimental human infections with Giardia lamblia. Journal of Infectious Diseases. 1987;156:974-984. [8] Ryan U. Cryptosporidium in birds, fish and amphibians. Experimental Parasitology. 2010;124:113-120. [9] Smith HV, Cacciò SM, Tait A, McLauchlin J, Thompson RCA. Tools for investigating the environmental transmission of Cryptosporidium and Giardia infections in humans. Trends in Parasitology. 2006;22:160-167. [10] Borowski H, Clode PL, Thompson RCA. Active invasion and/or encapsulation? A reappraisal of host-cell parasitism by Cryptosporidium. Trends in Parasitology. 2008;24:509-516. [11] Ortega-Pierres G, Smith HV, Cacciò SM, Thompson RC. New tools provide further insights into Giardia and Cryptosporidium biology. Trends in Parasitology. 2009;25:410-416. [12] Ramirez NE, Ward LA, Sreevatsan S. A review of the biology and epidemiology of cryptosporidiosis in humans and animals. Microbes and Infection. 2004;6:773-785. 12 ©FORMATEX 2010 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ [13] Farthing MJG. Clinical aspects of human cryptosporidiosis. In: Petry F, ed. Cryptosporidiosis and Microsporidiosis. Contributions in Microbiology, vol 6. Basel: Karger; 2000:50-74. [14] Guarino A, Canani RB, Casola A, Pozio E, Russo R, Bruzzese E, Fontana M, Rubino A. Human intestinal cryptosporidiosis: secretory diarrhoea and enterotoxic activity in Caco-2 cells. Journal of Infectious Diseases. 1995;171:976-983. [15] Ungar BLP, Kao T-C, Burris JA, Finkelman FD. Cryptosporidium infection in an adult mouse model: independent roles for IFN-alpha and CD4 T lymphocytes in protective immunity. Journal of Immunology. 1991;147:1014-1022. [16] Chalmers RM, Davies AP. Minireview: Clinical cryptosporidiosis. Experimental Parasitology. 2010;124:138-146. [17] Mintz ED, Hudson-Wragg M, Mshar P, Cartter ML, Hadler JL. Foodborne giardiasis in a corporate office setting. Journal of Infectious Diseases. 1993;167:250-253. [18] Ali SA, Hill DR. Giardia intestinalis. Current Opinion in Infectious Diseases. 2003;16:453-460. [19] Monis PT, Thompson RCA. Cryptosporidium and Giardia-zoonoses: fact or fiction?. Infection, Genetics and Evolution. 2003;2:233-244. [20] Rossignol J-F. Cryptosporidium and Giardia: treatment options and prospects for new drugs. Experimental Parasitology. 2010;124:45-53. [21] United States Environmental Protection Agency. Giardia: human health criteria document. Available at www.epa.gov/waterscience/humanhealth/microbial/giardia.pdf. Accessed March 30, 2010. [22] Erlandsen SL, Feely DE. Trophozoite motility and the mechanism of attachment. In: Erlandsen SL, Meyer EA, eds. Giardia and Giardiasis. New York, NY: Plenum Press; 1984:33-63. [23] Meinhardt PL, Casemore DP, Miller KB. Epidemiologic aspects of human cryptosporidiosis and the role of waterborne transmission. Epidemiologic Reviews. 1996;18:118-136. [24] O’Donoghue P. Cryptosporidium and cryptosporidiosis in man and animals. International Journal for Parasitology. 1995;25:139-195. [25] Adam RD. Biology of Giardia lamblia. Clinical Microbiology Reviews. 2001;14:447-475. [26] Cacciò SM, Thompson RCA, McLauchlin J, Smith HV. Unravelling Cryptosporidium and Giardia epidemiology. Trends in Parasitology. 2005;21:430-437. [27] Fayer R, Morgan U, Upton SJ. Epidemiology of Cryptosporidium: transmission, detection and identification. International Journal for Parasitology. 2000;30:1305-1322. [28] Chalmers RM, Ferguson C, Cacciò S, Gasser RB, Abs EL-Osta YG, Heijnen L, Xiao L, Elwin K, Hadfield S, Sinclair M, Stevens M. Direct comparison of selected methods for genetic categorisation of Cryptosporidium parvum and Cryptosporidium hominis species. International Journal for Parasitology. 2005;35:397-410. [29] Bowman DD, Lucio-Forster A. Cryptosporidiosis and giardiasis in dogs and cats: veterinary and public health importance. Experimental Parasitology. 2010;124:121-127. [30] Thompson RCA. The zoonotic significance and molecular epidemiology of Giardia and giardiasis. Veterinary Parasitology. 2004;126:15-35. [31] Robertson LJ. Giardia and Cryptosporidium infections in sheep and goats: a review of the potential for transmission to humans via environmental contamination. Epidemiology and Infection. 2009;137:913-921. [32] Thompson RC, Palmer CS, O'Handley R. The public health and clinical significance of Giardia and Cryptosporidium in domestic animals. Veterinary Journal. 2008;177:18-25. [33] Graczyk TK, Majewska AC, Schwab KJ. The role of birds in dissemination of human waterborne enteropathogens. Trends in Parasitology. 2008;24:55-59. [34] MacKenzie WR, Hoxie NJ, Proctor ME, Gradus MS, Blair KA, Peterson DE, Kazmierczak JJ, Addiss DG, Fox KR, Rose JB, Davis JP. A massive outbreak in Milwaukee of Cryptosporidium infection transmitted through the public water supply. The New England Journal of Medicine. 1994;331:161-167. [35] Corso P, Kramer M, Blair K, Addiss D, Davis J, Haddix A. Cost of illness in the 1993 waterborne Cryptosporidium outbreak, Milwaukee, Wisconsin. Emerging and Infectious Diseases. 2003;9:426-431. [36] Karanis P, Kourenti C, Smith H. Waterborne transmission of protozoan parasites: a worldwide review of outbreaks and lessons learnt. Journal of Water and Health. 2007;5:1-38. [37] Craun GF, Calderon RL, Craun MF. Outbreaks associated with recreational water in the United States. International Journal of Environmental Health Research. 2005;15:243-262. [38] Smith A, Reacher M, Smerdon W, Adak GK, Nichols G, Chalmers RM. Outbreaks of waterborne infectious intestinal disease in England and Wales, 1992-2003. Epidemiology and Infection. 2006;134:1141-1149. [39] Robertson LJ, Forberg T, Hermansen L, Gjerde BK, Alvsvåg JO, Langeland N. Cryptosporidium parvum infections in Bergen, Norway, during an extensive outbreak of waterborne giardiasis in autumn and winter 2004. Applied and Environmental Microbiology. 2006;72:2218-2220. [40] World Health Organization. Risk assessment of Cryptosporidium in drinking water. Available at http://whqlibdoc.who.int/hq/2009/WHO_HSE_WSH_09.04_eng.pdf. Accessed March 30, 2010. [41] Smith HV, Cacciò SM, Cook N, Nichols RA, Tait A. Cryptosporidium and Giardia as foodborne zoonoses. Veterinary Parasitology. 2007;149:29-40. [42] Castro-Hermida JA, García-Presedo I, Almeida A, González-Warleta M, Da Costa JM, Mezo M. Detection of Cryptosporidium spp. and Giardia duodenalis in surface water: a health risk for humans and animals. Water Research. 2009;43:4133-4142. [43] Ives RL, Kamarainen AM, John DE, Rose JB. Use of cell culture to assess Cryptosporidium parvum survival rates in natural groundwaters and surface waters. Applied and Environmental Microbiology. 2007;73:5968-5970. [44] King BJ, Monis PT. Critical processes affecting Cryptosporidium oocyst survival in the environment. Parasitology. 2007;134:309-323. [45] Medema GJ, Schets FM, Teunis PF, Havelaar AH. Sedimentation of free and attached Cryptosporidium oocysts and Giardia cysts in water. Applied and Environmental Microbiology. 1998;64:4460-4466. ©FORMATEX 2010 13 Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology A. Méndez-Vilas (Ed.) _______________________________________________________________________________________ [46] Betancourt WQ, Rose JB. Drinking water treatment processes for removal of Cryptosporidium and Giardia. Veterinary Parasitology. 2004;126:219-234. [47] DuPont HL, Chappell CL, Sterling CR, Okhuysen PC, Rose JB, Jakubowski W. The infectivity of Cryptosporidium parvum in healthy volunteers. New England Journal of Medicine. 1995;332:855-859. [48] Okhuysen PC, Chappell CL, Crabb JH, Sterling CR, DuPont HL. Virulence of three distinct Cryptosporidium parvum isolates for healthy adults. Journal of Infectious Diseases. 1999;180:1275-1281. [49] Chappell CL, Okhuysen PC, Langer-Curry R, Widmer G, Akiyoshi DE, Tanriverdi S, Tzipori S. Cryptosporidium hominis: experimental challenge of healthy adults. American Journal of Tropical Medicine and Hygiene. 2006;75:851-857. [50] US-Environmental Protection Agency. Method 1623: Cryptosporidium and Giardia in water by filtration/IMS/FA. Office of Water. 2005. Availabe at www.epa.gov/microbes/1623de05.pdf. Accessed March 30, 2010. [51] Jex AR, Smith HV, Monis PT, Campbell BE, Gasser RB. Cryptosporidium--biotechnological advances in the detection, diagnosis and analysis of genetic variation. Biotechnology Advances. 2008;26:304-317. [52] Wallis PM, Erlandsen SL, Isaac-Renton JL, Olson ME, Robertson WL, van Keulen H. Prevalence of Giardia cysts and Cryptosporidium oocysts and characterization of Giardia spp. isolated from drinking water in Canada. Applied and Environmental Microbiology. 1996;62:2789-2797. [53] Gale P. Risk assessment model for a waterborne outbreak of cryptosporidiosis. Water Science and Technology. 2000;41:1-7. [54] Carmena D, Aguinagalde X, Fernández-Crespo JC, Zigorraga C, Ocio JA. Presence of Cryptosporidium spp. oocysts and Giardia spp. cysts in drinking water supplies in northern Spain. Journal of Applied Microbiology. 2007;102:619-629. [55] McCuin RM, Clancy JL. Methods for the recovery, isolation and detection of Cryptosporidium oocysts in wastewaters. Journal of Microbiological Methods. 2005;63:73-88. [56] Clancy JL, Bukhari Z, McCuin RM, Matheson Z, Fricker C. USEPA method 1622. Journal of American Water Works Association. 1999;91:60-68. [57] Pezzana A, Vilaginès P, Bordet F, Coquard D, Sarrette B, Vilaginès R. Optimization of the Envirochek capsule method and immunomagnetic separation procedure for the detection of low levels of Cryptosporidium in large drinking water samples. Water Science and Technology. 2000;41:111-117. [58] Zhang T, Xie X, Hu H, Song Y, Wu Q, Zong Z. Improvement of detection method of Cryptosporidium and Giardia in reclaimed water. Frontiers of Environmental Science and Engineering in China. 2008;2:380-384. [59] Jenkins MB, Ghiorse WC, Anguish LJ, Bowman DD, Walker MJ. Author’s Reply to Letter to the Editor, Viability of Cryptosporidium parvum oocysts: Assessment by the dye permeability assay. Applied and Environmental Microbiology. 1998;64:3544-3545. [60] Robertson LJ. Gjerde BK. Cryptosporidium oocysts: challenging adversaries? Trends in Parasitology. 2007;23:344-347. [61] Bouzid M, Steverding D, Tyler KM. Detection and surveillance of waterborne protozoan parasites. Current Opinion in Biotechnology. 2008;19:1-5. [62] United States Environmental Protection Agency. National primary drinking water regulations: long term 1 enhanced surface water treatment rule; Final Rule. Federal Register. 2002;67:1812-1844. Available at http://frwebgate.access.gpo.gov/cgibin/getdoc.cgi?dbname=2002_register&docid=02-409-filed.pdf. Accessed March 30, 2010. [63] Health Canada. Guidelines for Canadian drinking water quality: Supporting documentation – Protozoa: Giardia and Cryptosporidium. Water Quality and Health Bureau, Healthy Environments and Consumer Safety Branch. 2004. http://www.hc-sc.gc.ca/ewh-semt/alt_formats/hecs-sesc/pdf/pubs/water-eau/protozoa/protozoa.pdf. Accessed March 30, 2010. [64] The guidelines for drinking-water quality management for New Zealand. Protozoa Compliance. 2005. Availble at Accessed http://www.moh.govt.nz/moh.nsf/0/5A25BF765B400911CC25708F0002B5A8/$File/08-protozoacompliance.pdf. March 30, 2010. [65] Drinking Water Inspectorate for England and Wales. The water supply (water quality) regulations 2000. Available at http://www.dwi.gov.uk/stakeholders/legislation/ws_wqregs2000.pdf. Accessed March 30, 2010. [66] Drinking Water Inspectorate for Northern Ireland. Guidance for the monitoring of Cryptosporidium in treated water supplies in Northern Ireland. 2003. Available at http://www.ni-environment.gov.uk/crypto_guidance_april05.pdf. Accessed March 30, 2010. [67] Fairley CK, Sinclair MI, Rizak S. Monitoring not the answer to Cryptosporidium in water. Lancet. 1999;354:967-969. [68] Haas CN, Rose JB. Developing an action level for Cryptosporidium. Journal of the American Water Works Association. 1995;87:81-84. [69] Wallis PM, Erlandsen SL, Isaac-Renton JL, Olson ME, Robertson WJ, van Keulen H. Prevalence of Giardia cysts and Cryptosporidium oocysts and characterization of Giardia spp. isolated from drinking water in Canada. Applied and Environmental Microbiology. 1996;62:2789-2797. [70] Rose JB, Haas CN, Regli S. Risk assessment and control of waterborne giardiasis. American Journal of Public Health. 1991 Jun;81(6):709-13. [71] Casman EA, Fischhoff B, Palmgren C, Small MJ, Wu F. An integrated risk model of a drinking-water-borne cryptosporidiosis outbreak. Risk Analysis. 2000;20:495-511. [72] Pouillot R, Beaudeau P, Denis JB, Derouin F; AFSSA Cryptosporidium Study Group. A quantitative risk assessment of waterborne cryptosporidiosis in France using second-order Monte Carlo simulation. Risk Analysis. 2004;24:1-17. [73] Smerdon WJ, Nichols T, Chalmers RM, Heine H, Reacher MH. Foot and mouth disease in livestock and reduced cryptosporidiosis in humans, England and Wales. Emerging Infectious Diseases. 2003;9:22-28. 14 ©FORMATEX 2010