Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
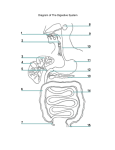
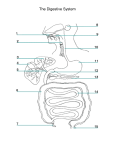
The intestines Small Intestine The small intestine is the longest part of the alimentary canal and extends from the pylorus of the stomach to the ileocecal junction. The greater part of digestion and food absorption takes place in the small intestine. It is divided into three parts: the duodenum, the jejunum, and the ileum. General arrangement of abdominal viscera Duodenum Location and Description The duodenum is a C-shaped tube, about 10 in. (25 cm) long, which joins the stomach to the jejunum. It receives the openings of the bile and pancreatic ducts. The duodenum curves around the head of the pancreas. The first inch (2.5 cm) of the duodenum resembles the stomach in that it is covered on its anterior and posterior surfaces with peritoneum and has the lesser omentum attached to its upper border and the greater omentum attached to its lower border; the lesser sac lies behind this short segment. The remainder of the duodenum is retroperitoneal, being only partially covered by peritoneum. Pancreas and anterior relations of the kidneys Parts of the Duodenum The duodenum is situated in the epigastric and umbilical regions and, for purposes of description, is divided into four parts. First Part of the Duodenum The first part of the duodenum begins at the pylorus and runs upward and backward on the transpyloric plane at the level of the first lumbar vertebra. Posterior relations of the duodenum and the pancreas. The numbers represent the four parts of the duodenum. The relations of this part are as follows: Anteriorly: The quadrate lobe of the liver and the gallbladder Posteriorly: The lesser sac (first inch only), the gastroduodenal artery, the bile duct and portal vein, and the inferior vena cava Attachment of the lesser omentum to the stomach and the posterior surface of the liver Superiorly: The entrance into the lesser sac (the epiploic foramen) Transverse section of the lesser sac showing the arrangement of the peritoneum in the formation of the lesser omentum, the gastrosplenic omentum, and the splenicorenal ligament. Arrow indicates the position of the opening of the lesser sac. Inferiorly: The head of the pancreas Pancreas and anterior relations of the kidneys. Second Part of the Duodenum The second part of the duodenum runs vertically downward in front of the hilum of the right kidney on the right side of the second and third lumbar vertebrae. Posterior relations of the duodenum and the pancreas. The numbers represent the four parts of the duodenum. About halfway down its medial border, the bile duct and the main pancreatic duct pierce the duodenal wall. They unite to form the ampulla that opens on the summit of the major duodenal papilla. The accessory pancreatic duct, if present, opens into the duodenum a little higher up on the minor duodenal papilla. Entrance of the bile duct and the main and accessory pancreatic ducts into the second part of the duodenum. Note the smooth lining of the first part of the duodenum, the plicae circulares of the second part, and the major duodenal papilla. The relations of this part are as follows: Anteriorly: The fundus of the gallbladder and the right lobe of the liver, the transverse colon, and the coils of the small intestine Posteriorly: The hilum of the right kidney and the right ureter Laterally: The ascending colon, the right colic flexure, and the right lobe of the liver Medially: The head of the pancreas, the bile duct, and the main pancreatic duct Note the relation of the gallbladder to the transverse colon and the duodenum. Third Part of the Duodenum The third part of the duodenum runs horizontally to the left on the subcostal plane, passing in front of the vertebral column and following the lower margin of the head of the pancreas. The relations of this part are as follows: Anteriorly: The root of the mesentery of the small intestine, the superior mesenteric vessels contained within it, and coils of jejunum Posteriorly: The right ureter, the right psoas muscle, the inferior vena cava, and the aorta Superiorly: The head of the pancreas Inferiorly: Coils of jejunum Pancreas and anterior relations of the kidneys. Fourth Part of the Duodenum The fourth part of the duodenum runs upward and to the left to the duodenojejunal flexure. Posterior relations of the duodenum and the pancreas. The numbers represent the four parts of the duodenum. The flexure is held in position by a peritoneal fold, the ligament of Treitz, which is attached to the right crus of the diaphragm. Peritoneal recesses, which may be present in the region of the duodenojejunal junction. Note the presence of the inferior mesenteric vein in the peritoneal fold, forming the paraduodenal recess. The relations of this part are as follows: Anteriorly: The beginning of the root of the mesentery and coils of jejunum Posteriorly: The left margin of the aorta and the medial border of the left psoas muscle Attachment of the root of the mesentery of the small intestine to the posterior abdominal wall. Note that it extends from the duodenojejunal flexure on left of the aorta, downward and to the right to the ileocecal junction. The superior mesenteric artery lies in the root of the mesentery. Mucous Membrane and Duodenal Papillae The mucous membrane of the duodenum is thick. In the first part of the duodenum it is smooth. In the remainder of the duodenum it is thrown into numerous circular folds called the plicae circulares. At the site where the bile duct and the main pancreatic duct pierce the medial wall of the second part is a small, rounded elevation called the major duodenal papilla. The accessory pancreatic duct, if present, opens into the duodenum on a smaller papilla about 0.75 in. (1.9 cm) above the major duodenal papilla. Entrance of the bile duct and the main and accessory pancreatic ducts into the second part of the duodenum. Note the smooth lining of the first part of the duodenum, the plicae circulares of the second part, and the major duodenal papilla. Blood Supply Arteries The upper half is supplied by the superior pancreaticoduodenal artery, a branch of the gastroduodenal artery. The lower half is supplied by the inferior pancreaticoduodenal artery, a branch of the superior mesenteric artery. Arteries that supply the stomach. Note that all the arteries are derived from branches of the celiac artery. Veins The superior pancreaticoduodenal vein drains into the portal vein; the inferior vein joins the superior mesenteric vein. Lymph Drainage The lymph vessels follow the arteries and drain upward via pancreaticoduodenal nodes to the gastroduodenal nodes and then to the celiac nodes and downward via pancreaticoduodenal nodes to the superior mesenteric nodes around the origin of the superior mesenteric artery. Nerve Supply The nerves are derived from sympathetic and parasympathetic (vagus) nerves from the celiac and superior mesenteric plexuses. Tributaries of the portal vein Clinical Notes Trauma to the Duodenum In severe crush injuries to the anterior abdominal wall, the third part of the duodenum may be severely crushed or torn against the third lumbar vertebra. Duodenal Ulcer As the stomach empties its contents into the duodenum, the acid chyme is squirted against the anterolateral wall of the first part of the duodenum. This is thought to be an important factor in the production of a duodenal ulcer at this site. An ulcer of the anterior wall of the first inch of the duodenum may perforate into the upper part of the greater sac, above the transverse colon. The transverse colon directs the escaping fluid into the right lateral paracolic gutter and thus down to the right iliac fossa. An ulcer of the posterior wall of the first part of the duodenum may penetrate the wall and erode the relatively large gastroduodenal artery, causing a severe hemorrhage. Duodenal Recesses The importance of the duodenal recesses and the occurrence of herniae of the intestine. Important Duodenal Relations The relation to the duodenum of the gallbladder, the transverse colon, and the right kidney should be remembered. Cases have been reported in which a large gallstone ulcerated through the gallbladder wall into the duodenum. Operations on the colon and right kidney have resulted in damage to the duodenum. Jejunum and Ileum Location and Description The jejunum and ileum measure about 20 ft (6 m) long; the upper two fifths of this length make up the jejunum. The jejunum begins at the duodenojejunal flexure, and the ileum ends at the ileocecal junction. The coils of jejunum and ileum are freely mobile and are attached to the posterior abdominal wall by a fanshaped fold of peritoneum known as the mesentery of the small intestine. Attachment of the root of the mesentery of the small intestine to the posterior abdominal wall. Note that it extends from the duodenojejunal flexure on left of the aorta, downward and to the right to the ileocecal junction. The superior mesenteric artery lies in the root of the mesentery. The long free edge of the fold encloses the mobile intestine. The short root of the fold is continuous with the parietal peritoneum on the posterior abdominal wall along a line that extends downward and to the right from the left side of the second lumbar vertebra to the region of the right sacroiliac joint. The root of the mesentery permits the entrance and exit of the branches of the superior mesenteric artery and vein, lymph vessels, and nerves into the space between the two layers of peritoneum forming the mesentery. In the living, The jejunum can be distinguished from the ileum by the following features: The jejunum lies coiled in the upper part of the peritoneal cavity below the left side of the transverse mesocolon; the ileum is in the lower part of the cavity and in the pelvis. Abdominal contents after the greater omentum has been reflected upward. Coils of small intestine occupy the central part of the abdominal cavity, whereas ascending, transverse, and descending parts of the colon are located at the periphery. The jejunum is wider bored, thicker walled, and redder than the ileum. The jejunal wall feels thicker because the permanent infoldings of the mucous membrane, the plicae circulares, are larger, more numerous, and closely set in the jejunum, whereas in the upper part of the ileum they are smaller and more widely separated and in the lower part they are absent. The jejunal mesentery is attached to the posterior abdominal wall above and to the left of the aorta, whereas the ileal mesentery is attached below and to the right of the aorta. Some external and internal differences between the jejunum and the ileum. The jejunal mesenteric vessels form only one or two arcades, with long and infrequent branches passing to the intestinal wall. The ileum receives numerous short terminal vessels that arise from a series of three or four or even more arcades. At the jejunal end of the mesentery, the fat is deposited near the root and is scanty near the intestinal wall. At the ileal end of the mesentery the fat is deposited throughout so that it extends from the root to the intestinal wall. Aggregations of lymphoid tissue (Peyer's patches) are present in the mucous membrane of the lower ileum along the antimesenteric border. In the living these may be visible through the wall of the ileum from the outside. Blood Supply Arteries The arterial supply is from branches of the superior mesenteric artery. The intestinal branches arise from the left side of the artery and run in the mesentery to reach the gut. They anastomose with one another to form a series of arcades. The lowest part of the ileum is also supplied by the ileocolic artery. Superior mesenteric artery and its branches. Note that this artery supplies blood to the gut from halfway down the second part of the duodenum to the distal third of the transverse colon (arrow). Veins The veins correspond to the branches of the superior mesenteric artery and drain into the superior mesenteric vein. Lymph Drainage The lymph vessels pass through many intermediate mesenteric nodes and finally reach the superior mesenteric nodes, which are situated around the origin of the superior mesenteric artery. Nerve Supply The nerves are derived from the sympathetic and parasympathetic (vagus) nerves from the superior mesenteric plexus. Clinical Notes Trauma to the Jejunum and Ileum Because of its extent and position, the small intestine is commonly damaged by trauma. Small, penetrating injuries may self-seal as a result of the mucosa plugging up the hole and the contraction of the smooth muscle wall. The presence of the vertebral column and the prominent anterior margin of the first sacral vertebra may provide a firm background for intestinal crushing in cases of midline crush injuries. Recognition of the Jejunum and Ileum A physician should be able to distinguish between the large and small intestine. He or she may be called on to examine a case of postoperative burst abdomen, where coils of gut are lying free in the bed. Tumors and Cysts of the Mesentery of the Small Intestine A tumor or cyst of the mesentery, when palpated through the anterior abdominal wall, is more mobile in a direction at right angles to the line of attachment than along the line of attachment. Pain Fibers from the Jejunum and Ileum Pain fibers traverse the superior mesenteric sympathetic plexus and pass to the spinal cord via the splanchnic nerves. Referred pain from this segment of the gastrointestinal tract is felt in the dermatomes supplied by the 9th, 10th, and 11th thoracic nerves. Strangulation of a coil of small intestine in an inguinal hernia first gives rise to pain in the region of the umbilicus. Mesenteric Arterial Occlusion The superior mesenteric artery, a branch of the abdominal aorta, supplies an extensive territory of the gut, from halfway down the second part of the duodenum to the left colic flexure. Occlusion of the artery or one of its branches results in death of all or part of this segment of the gut. The occlusion may occur as the result of an embolus, a thrombus, an aortic dissection, or an abdominal aneurysm. Mesenteric Vein Thrombosis The superior mesenteric vein, which drains the same area of the gut supplied by the superior mesenteric artery, may undergo thrombosis after stasis of the venous bed. Cirrhosis of the liver with portal hypertension may predispose to this condition. Meckel's Diverticulum Meckel's diverticulum, a congenital anomaly of the ileum. Large Intestine The large intestine extends from the ileum to the anus. It is divided into the cecum, appendix, ascending colon, transverse colon, descending colon, and sigmoid colon. The primary function of the large intestine is the absorption of water and electrolytes and the storage of undigested material until it can be expelled from the body as feces. Cecum Location and Description The cecum is that part of the large intestine that lies below the level of the junction of the ileum with the large intestine. It is a blind-ended pouch that is situated in the right iliac fossa. It is about 2.5 in. (6 cm) long and is completely covered with peritoneum. It possesses a considerable amount of mobility, although it does not have a mesentery. Attached to its posteromedial surface is the appendix. The presence of peritoneal folds in the vicinity of the cecum creates the superior ileocecal, the inferior ileocecal, and the retrocecal recesses. As in the colon, the longitudinal muscle is restricted to three flat bands, the teniae coli, which converge on the base of the appendix and provide for it a complete longitudinal muscle coat. The cecum is often distended with gas. The terminal part of the ileum enters the large intestine at the junction of the cecum with the ascending colon. The opening is provided with two folds, or lips, which form the so-called ileocecal valve. The appendix communicates with the cavity of the cecum through an opening located below and behind the ileocecal opening. Cecum and appendix. Note that the appendicular artery is a branch of the posterior cecal artery. Relations Anteriorly: Coils of small intestine, sometimes part of the greater omentum, and the anterior abdominal wall in the right iliac region Posteriorly: The psoas and the iliacus muscles, the femoral nerve, and the lateral cutaneous nerve of the thigh. The appendix is commonly found behind the cecum. Posterior abdominal wall showing posterior relations of the kidneys and the colon. Medially: The appendix arises from the cecum on its medial side. Blood Supply Arteries Anterior and posterior cecal arteries form the ileocolic artery, a branch of the superior mesenteric artery. Veins The veins correspond to the arteries and drain into the superior mesenteric vein. Lymph Drainage The lymph vessels pass through several mesenteric nodes and finally reach the superior mesenteric nodes. Nerve Supply Branches from the sympathetic and parasympathetic (vagus) nerves form the superior mesenteric plexus. leocecal Valve A rudimentary structure, the ileocecal valve consists of two horizontal folds of mucous membrane that project around the orifice of the ileum. The valve plays little or no part in the prevention of reflux of cecal contents into the ileum. The circular muscle of the lower end of the ileum (called the ileocecal sphincter by physiologists) serves as a sphincter and controls the flow of contents from the ileum into the colon. The smooth muscle tone is reflexly increased when the cecum is distended; the hormone gastrin, which is produced by the stomach, causes relaxation of the muscle tone. Appendix Location and Description The appendix is a narrow, muscular tube containing a large amount of lymphoid tissue. It varies in length from 3 to 5 in. (8 to 13 cm). The base is attached to the posteromedial surface of the cecum about 1 in. (2.5 cm) below the ileocecal junction. The remainder of the appendix is free. It has a complete peritoneal covering, which is attached to the mesentery of the small intestine by a short mesentery of its own, the mesoappendix. The mesoappendix contains the appendicular vessels and nerves. The appendix lies in the right iliac fossa, and in relation to the anterior abdominal wall its base is situated one third of the way up the line joining the right anterior superior iliac spine to the umbilicus (McBurney's point). Inside the abdomen, the base of the appendix is easily found by identifying the teniae coli of the cecum and tracing them to the base of the appendix, where they converge to form a continuous longitudinal muscle coat. Common Positions of the Tip of the Appendix The tip of the appendix is subject to a considerable range of movement and may be found in the following positions: (a) hanging down into the pelvis against the right pelvic wall, (b) coiled up behind the cecum, (c) projecting upward along the lateral side of the cecum, and (d) in front of or behind the terminal part of the ileum. The first and second positions are the most common sites. Blood Supply Arteries The appendicular artery is a branch of the posterior cecal artery. Veins The appendicular vein drains into the posterior cecal vein. Lymph Drainage The lymph vessels drain into one or two nodes lying in the mesoappendix and then eventually into the superior mesenteric nodes. Nerve Supply The appendix is supplied by the sympathetic and parasympathetic (vagus) nerves from the superior mesenteric plexus. Afferent nerve fibers concerned with the conduction of visceral pain from the appendix accompany the sympathetic nerves and enter the spinal cord at the level of the 10th thoracic segment. Ascending Colon Location and Description The ascending colon is about 5 in. (13 cm) long and lies in the right lower quadrant. It extends upward from the cecum to the inferior surface of the right lobe of the liver, where it turns to the left, forming the right colic flexure, and becomes continuous with the transverse colon. The peritoneum covers the front and the sides of the ascending colon, binding it to the posterior abdominal wall. Abdominal cavity showing the terminal part of the ileum, the cecum, the appendix, the ascending colon, the right colic flexure, the left colic flexure, and the descending colon. Note the teniae coli and the appendices epiploicae. Relations Anteriorly: Coils of small intestine, the greater omentum, and the anterior abdominal wall Abdominal contents after the greater omentum has been reflected upward. Coils of small intestine occupy the central part of the abdominal cavity, whereas ascending, transverse, and descending parts of the colon are located at the periphery. Posteriorly: The iliacus, the iliac crest, the quadratus lumborum, the origin of the transversus abdominis muscle, and the lower pole of the right kidney. The iliohypogastric and the ilioinguinal nerves cross behind it. Blood Supply Arteries The ileocolic and right colic branches of the superior mesenteric artery supply this area. Veins The veins correspond to the arteries and drain into the superior mesenteric vein. Lymph Drainage The lymph vessels drain into lymph nodes lying along the course of the colic blood vessels and ultimately reach the superior mesenteric nodes. Nerve Supply Sympathetic and parasympathetic (vagus) nerves from the superior mesenteric plexus supply this area of the colon. Transverse Colon Location and Description The transverse colon is about 15 in. (38 cm) long and extends across the abdomen, occupying the umbilical region. It begins at the right colic flexure below the right lobe of the liver and hangs downward, suspended by the transverse mesocolon from the pancreas. It then ascends to the left colic flexure below the spleen. The left colic flexure is higher than the right colic flexure and is suspended from the diaphragm by the phrenicocolic ligament. The right colic flexure, the left colic flexure, and the descending colon. Note the teniae coli and the appendices epiploicae. The transverse mesocolon, or mesentery of the transverse colon, suspends the transverse colon from the anterior border of the pancreas. The mesentery is attached to the superior border of the transverse colon, and the posterior layers of the greater omentum are attached to the inferior border. Because of the length of the transverse mesocolon, the position of the transverse colon is extremely variable and may sometimes reach down as far as the pelvis. Relations Anteriorly: The greater omentum and the anterior abdominal wall (umbilical and hypogastric regions) Posteriorly: The second part of the duodenum, the head of the pancreas, and the coils of the jejunum and ileum Blood Supply Arteries The proximal two thirds are supplied by the middle colic artery, a branch of the superior mesenteric artery. The distal third is supplied by the left colic artery, a branch of the inferior mesenteric artery. Veins The veins correspond to the arteries and drain into the superior and inferior mesenteric veins. Lymph Drainage The proximal two thirds drain into the colic nodes and then into the superior mesenteric nodes; the distal third drains into the colic nodes and then into the inferior mesenteric nodes. Nerve Supply The proximal two thirds are innervated by sympathetic and vagal nerves through the superior mesenteric plexus; the distal third is innervated by sympathetic and parasympathetic pelvic splanchnic nerves through the inferior mesenteric plexus. Inferior mesenteric artery and its branches. Note that this artery supplies the large bowel from the distal third of the transverse colon to halfway down the anal canal. It anastomoses with the middle colic branch of the superior mesenteric artery (arrow). Descending Colon Location and Description The descending colon is about 10 in. (25 cm) long and lies in the left upper and lower quadrants. It extends downward from the left colic flexure, to the pelvic brim, where it becomes continuous with the sigmoid colon. The peritoneum covers the front and the sides and binds it to the posterior abdominal wall. Relations Anteriorly: Coils of small intestine, the greater omentum, and the anterior abdominal wall Posteriorly: The lateral border of the left kidney, the origin of the transversus abdominis muscle, the quadratus lumborum, the iliac crest, the iliacus, and the left psoas. The iliohypogastric and the ilioinguinal nerves, the lateral cutaneous nerve of the thigh, and the femoral nerve also lie posteriorly. Posterior abdominal wall showing posterior relations of the kidneys and the colon Blood Supply Arteries The left colic and the sigmoid branches of the inferior mesenteric artery supply this area. Veins The veins correspond to the arteries and drain into the inferior mesenteric vein. Lymph Drainage Lymph drains into the colic lymph nodes and the inferior mesenteric nodes around the origin of the inferior mesenteric artery. Nerve Supply The nerve supply is the sympathetic and parasympathetic pelvic splanchnic nerves through the inferior mesenteric plexus. Clinical Notes Colonoscopy is now being extensively used for early detection of malignant tumors. In this procedure, the mucous membrane of the colon can be directly visualized through an elongated flexible tube, or endoscope. The interior of the large bowel can be observed from the anus to the cecum . Photographs of suspicious areas, such as polyps, can be taken and biopsy specimens can be removed for pathologic examination. Series of the interior of the large bowel taken during a colonoscopy procedure. A. The rectal mucosa shows a small benign polyp (arrowhead). B. The sigmoid mucous membrane shows evidence of a mild diverticulosis. Arrowheads indicate the entrances into the mucosal pouches. C. The splenic flexure is normal. Note the light reflections from the drops of mucus on the mucous membrane. D. The transverse colon shows the characteristic normal folds or ridges (arrowheads) between the sacculations of the wall of the colon. E. The ileocecal valve shows the upper lip (arrowheads) of the valve, which has a normal appearance. F. Finally, the mucous membrane lining the inferior wall or floor of the cecum looks normal. Variability of Position of the Appendix The inconstancy of the position of the appendix should be borne in mind when attempting to diagnose an appendicitis. A retrocecal appendix, for example, may lie behind a cecum distended with gas, and thus it may be difficult to elicit tenderness on palpation in the right iliac region. Irritation of the psoas muscle, conversely, may cause the patient to keep the right hip joint flexed. An appendix hanging down in the pelvis may result in absent abdominal tenderness in the right lower quadrant, but deep tenderness may be experienced just above the symphysis pubis. Rectal or vaginal examination may reveal tenderness of the peritoneum in the pelvis on the right side. Pain of Appendicitis Visceral pain in the appendix is produced by distention of its lumen or spasm of its muscle. The afferent pain fibers enter the spinal cord at the level of the 10th thoracic segment, and a vague referred pain is felt in the region of the umbilicus. Later, the pain shifts to where the inflamed appendix irritates the parietal peritoneum. Here the pain is precise, severe, and localized. Trauma of the Cecum and Colon Blunt or penetrating injuries to the colon occur. Blunt injuries most commonly occur where mobile parts of the colon (transverse and sigmoid) join the fixed parts (ascending and descending). Penetrating injuries following stab wounds are common. The multiple anatomic relationships of the different parts of the colon explain why isolated colonic trauma is unusual. Cancer of the Large Bowel Cancer of the large bowel is relatively common in persons older than 50 years. The growth is restricted to the bowel wall for a considerable time before it spreads via the lymphatics. Bloodstream spread via the portal circulation to the liver occurs late. Diverticulosis Diverticulosis of the colon is a common clinical condition. It consists of a herniation of the lining mucosa through the circular muscle between the teniae coli and occurs at points where the circular muscle is weakest that is, where the blood vessels pierce the muscle. Blood supply to the colon (A) and formation of the diverticulum (B). Note the passage of the mucosal diverticulum through the muscle coat along the course of the artery. Cecostomy and Colostomy Because of the anatomic mobility of the cecum, transverse colon, and sigmoid colon, they may be brought to the surface through a small opening in the anterior abdominal wall. These procedures are referred to as cecostomy or colostomy, respectively, and are used to relieve large-bowel obstructions. Volvulus Because of its extreme mobility, the sigmoid colon sometimes rotates around its mesentery. This may correct itself spontaneously or the rotation may continue until the blood supply of the gut is cut off completely. Intussusception Intussusception is the telescoping of a proximal segment of the bowel into the lumen of an adjoining distal segment. Needless to say, there is a grave risk of cutting off the blood supply to the gut and developing gangrene.