Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
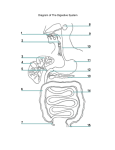
Coeliac Trunk It is the artery of foregut, it supplies GIT from lower 1/3 of esophgus down as far as the middle of second part of duodenum. Origin : is very short and arises from front of abdominal aorta at level of lower border of T12 vertebra. It is surrounded by the celiac plexus of nerves. It lies behind the lesser sac of peritoneum. It has 3 terminal branches : 1-Left gastric artery. 2-Splenic artery. 3-Hepatic artery. 1- Left gastric artery It is the smallest branch of celiac trunk. It passes upwards and to left side to reach cardiac end of stomach. It then passes downwards between the 2 layers of lesser omentum along lesser curvature of stomach. It ends by anastomosing with right gastric artery. Branches : 1-Esophageal branches to lower end of esophagus. 2-Gastric branches : to supply both surfaces of stomach along lesser curvature. 2- Splenic Artery It is the largest branch of celiac trunk. It runs behind the stomach to the left side in a wavy course along upper border of pancreas. On reaching left kidney , it enters splenico-renal ligament to reach the hilum of spleen. 2- Splenic Artery Branches : 1-Pancreatic branches. 2-Left gastroepiploic artery : arises near hilum of spleen and passes in the gastro-splenic omentum (ligament) to supply the stomach along greater curvature of stomach and anastomoses with right gastroepiploic artery. 3-Short gastric arteries : arise from splenic artery at the hilum of spleen, and pass in the gastro-splenic omentum to supply fundus of stomach. They anastomose with left gastric & left gastroepiploic arteries. 3- Hepatic Artery It is one of the 3 branches of celiac trunk. It runs to the right and ascends between 2 layers of lesser omentum to lie in front of the opening into lesser sac., to the left of bile duct and in front of portal vein. At the porta hepatis, it divides into Rt. & left branches to supply the corresponding lobes of liver. 3- Hepatic Artery Branches : 1-Right gastric artery : arises from the hepatic artery at the upper border of pylorus to pass to the left in the lesser omentum along lesser curvature of stomach to anastomose with the left gastric artery. 2-Gastrodudenal artery : is a large branch that descends behind 1st part of duodenum. It divides into : -Right gastro-epiploic artery : that runs along greater curvature of stomach between the layers of greater omentum. & -Superior pancreatico-duodenal artery : that descends between 2nd part of duodenum & head of pancreas. 3-Right & left hepatic arteries : enter the porta hepatis of liver. Right hepatic artery gives off cystic artery, which run to neck of gallbladder. Small intestine It extends from the pylorus of stomach to the ileocecal junction. It is divided into 3 parts : duodenum, jejunum, & ileum. Duodenum It is a C-shaped tube, about 10 in.(25cm) long, that joins stomach to jejunum. It lies in epigastric & umbilical regions. It receives openings of bile & pancreatic ducts. It curves around the head of pancreas. It has 4 parts, /its 1st inch (2,5 cm) as the stomach in that it is covered completely anterior & posterior with peritoneum and has lesser omentum & greater omentum. Remainder of duodenum is retroperitoneal. Jejunum and Ileum They are about 6 meter long The jejunum begins at duodenojejunal flexure and ileum ends at ileocecal junction . The coils of jejunum & ileum are freely mobile and are attached to posterior abdominal wall by a fan-shaped fold of peritonium known as mesentry of small intestine which has a root along a line that extends downward and to right /from the left side of 2nd lumbar vertebra to the region of right sacroiliac joint. The root of mesentry contains superior mesenteric vessels. Lymph drainage : into superior mesenteric nodes. N.supply : sympathetic + parasympathetic (vagal) from the superior mesenteric plexuses Jejunum and Ileum Jejunum Ileum It lies in the upper part of peritoneal cavity. It lies in the lower part of abdominal cavity. It has wider lumen. It has narrower lumen. Its wall is thicker due to presence of larger & numerous circular folds of the m.m, the plica circularis. Its wall is thinner since the circular folds are smaller & fewer, and may be absent in its lower part. It is more vascular and redder. It is less vascular and paler. Jejunum and Ileum Jejunum Its mesentry is attached to posterior abdominal wall above & to left of aorta. Ileum Its mesentry is attached below & to right of aorta. Its mesenteric vessels form a series of 3-4 Its mesenteric vessels form only one or or more arcades, that send numerous short 2 archades, with long & infrequent terminal vessels. branches passing to the intestinal wall. It has a great amount of mesenteric fat. It has scanty of mesenteric fat. Aggreggations of lymphoid tissue (Peyer ‘s It has No lymphoid follicles. patches) are present in the m.m of lower ilum along antimesenteric border Large Intestine It extends from ileocecal junction to anus. It includes cecum, appendix, ascending colon, transverse colon, descending colon, sigmoid colon, rectum & anal canal. It is about 1 ½ meters. Differences between Large & Small intestines Large intestine is 150-180 cm. long, while small intestine is 6 meters long. It is wider than small intestine. Most of large intestine is fixed in position (retroperitoneal), while most of small intestine is mobile. It has 3 longitudinal muscle bands on its surface, the toenia coli ( but form a continuous longitudinal muscle layer in the small intestine). Teniae coli are shorter than the length of colon, leading to sacculation of the colon (sacculation is absent in small intestine). It has (except caecum, appendix & rectum) small peritoneal folds filled with fat called appendices epiploicae (but absent in small I.). Its m.m. has No Peyer’s patches as in the small intestine. Its m.m is smooth, but the small I. has villi. Cecum It is a blind-ended pouch (6cm.), lies in the right iliac fossa. Peritoneal covering : it is completely covered with peritoneum, except at its upper part of its post. wall, so it has a considerable range of mobility. The opening of the ileum : lies at the posteromedial side of the junction of cecum with ascending colon. It is a horizontal opening which is gaurded by ileo-cecal valve. It plays No role but the circular ms. of lower end of ileum is thickened in the region of the valve, forming the ileo-cecal sphincter acts as a sphincter to control the flow of contents from ileum into colon. The opening of appendix : lies 1 inch below and behind the ileocecal opening. anteriorly : coils of small intestine, greater omentum, anterior abd.wall. Posteriorly : psoas & iliacus ms.+ lateral cut. N.of thigh + femoral N. Appendix It is a muscular tube containing a large amount of lymphoid tissue, about 10cm.long. Its base is attached to postero-medial surface of cecum below the ileocecal valve. It has a complete peritoneal covering. It has mesentry, the mesoappendix, which contains appendicular vessels & nerves. Lymph Drainage of cecum & appendix : superior mesenteric L.Ns. Nerve Supply of cecum & appendix : sympathetic & parasympathetic (vagal) nerves from superior mesenteric plexus. It lies in right iliac fossa, in relation to anterior abd. wall. Its base lies one third of the way up the line joining the right anterior superior iliac spine to umbilicus (McBurney’s point). The teniae coli of cecum collect at the base of appendix to become continuous with the longitudinal muscle coat of appendix. Common position of the tip of appendix : 1 & 2 1-Hanging down into the pelvis. 2-Coiled up behind cecum (retrocecal). 3-Passing upward along lateral side of cecum (subcecal) 4-Front of or behind terminal part of Ascending Colon It is about 15 cm.long, lies in right lower quadrant, extending from cecum to inferior surface of right lobe of liver. It turns to left, forming right colic flexure, and becomes continuous with the transverse colon. It is covered with peritonium in its front & sides, binding it to the post. abdominal wall. Anteriorly : coils of small intestine, greater omentum & anterior abd.wall. Posteriorly : iliacus, quadratus lumborum, origin of transversus abdominis, right kidney, iliohypogastric & ilioinguinal nerves. Lymph drainage & Nerve supply : as cecum & appendix. Transverse Colon It is about 50 cm. long, extending across abdomen, occupying umbilical region. It begins at right colic flexure, supended by transverse mesocolon from the pancreas, to end at left colic flexure below the spleen. Left colic flexure is higher than the right, and is suspended from diaphragm by phrenico-colic ligament. Nerve supply : proximal 2/3 : sympathetic & vagal parasympathetic nrves through superior mesenteric plexus. Distal 1/3 : sympathetic /& parasympathetic pelvic splanchnic (sacral)nerves through inferior mesenteric plexus. Anteriorly : greater omentum, anterior abd.wall. Posteriorly : 2nd part of duodenum, head of pancres, coils of small intestine. Lymph drainage : proximal 2/3: drain into superior mesenteric nodes. Distal 1/3: drains into colic nodes and then into inferior mesenteric nodes. Descending Colon It is about 25 cm.long, lies in left upper & lower quadrants, extending downwards from left colic flexure to the pelvic brim, where it becomes continuous with the sigmoid colon. The peritoneum covers the front & sides and binds to post.abd. Wall. Anteriorly : coils of small intestine + greater omentum + anterior abd.wall. Posteriorly : left kidney, origin of transversus abdominis, quadratus lumborum, psoas, iliacus. / Iliohypogastric, ilioinguinal, lateral cutaneous N. of thigh, and femoral N. Lymph drainage : colic & inferior mesenteric L.Ns. N.supply : sympathetic /& parasympathetic pelvic splanchnic (S 2,3,4) nerves through inferior mesenteric plexus. Sigmoid Colon It is about 40 cm.long, S-shaped loop. It descends in the pelvic cavity as a continuation of descending colon, to end at the 3rd sacral vertebra to begin the rectum. it is completely covered with peritoneum which form a fan-shaped sigmoid mesocolon attached to posterior pelvic wall, so it is freely mobile. Anteriorly : in male : urinary bladder. In female : uterus + upper vagina. Posteriorly : rectum + sacrum. Lymph drainage : the nodes along course of sigmoid arteries drains into inferior mesenteric nodes. N. supply : sympathetic + parasympathetic nerves from the inferior hypogastric plexus. Factors contribute in appendix’s infection It is long, narrow, blind-ended tube, which leads to stasis of large-bowel contents. It has a large amount of lymphoid tissue in its wall. Its lumen has a tendency to becom obstructed by hardened intestinal cotents, leading to further stagnation of its contents, Pain of appendicitis visceral pain is produced by distention of its lumen or/ spasm of its muscle. Afferent pain fibres enter the spinal cord at the level of T10 segment, and a vague referred pain is felt in the region of umbilicus. Later, the pain shifts to where the inflamed appendix irritates the peritoneum, here pain is precise, severe and localized in right lower quadrant. Variability of position of Appendix It should be borne in mind for diagnosis of appendicitis. In retrocecal appendix, it is difficult to elicit tenderness on palpation in right iliac fossa, irritation of psoas ms., may cause the patient to keep his right hip joint flexed. An appendix hanging down in the pelvis may result in absent right iliac region tenderness, but deep tenderness may be revealed just above the symphysis pubis, rectal or vaginal examination may reveal tenderness of peritoneum in the right side of pelvis.