Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
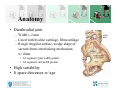
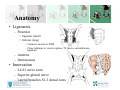
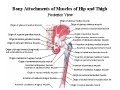
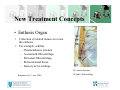
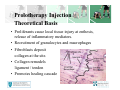
Sacroiliac Joint Dysfunction • Anatomy and Biomechanics • Epidemiology • Diagnosis – Clinical Presentation – Evaluation • Treatment – Standard – New treatments Anatomy • Diarthrodial joint – Width 1-2 mm – Lined with hyaline cartilage, fibrocartilage – Rough irregular surface, wedge shape of sacrum forms interlocking mechanism w/ ilium • S1 segment: post width greater • S3 segment: ant width greater • High variability • Jt space decreases w/ age Anatomy • Ligaments – Posterior • Superior (short) • Inferior (long) – Connects sacrum to PSIS – Close relations w/ erector spinae, TL fascia, sacrotuberous ligament – Anterior – Interosseous • Innervation – L4-S1 nerve roots – Superior gluteal nerve – Lateral branches S1-3 dorsal roots Sacroiliac Joint Biomechanics • Absorbs vertical forces b/t spine and pelvis/LEs • No muscles acting directly across SIJ • Stable, complex dynamic motion – 2-3 deg in transverse or longitudinal planes • Axis passing obliquely across pelvis – Hip flexion – ipsi ilium glides post/inf – Hip extension – ant and away from sacrum – ? Can motion be clinically detected • Transverses abdominus ctx: dec laxity of SIJ • Delayed activation of multifidus, internal oblique and glut max w/ SIJ pain • Netter mm attachments slide Piriformis Intimate Association • Piriformis syndrome Epidemiology • • • • • • LBP affects 70% of people Pain generator can be identified in 75% cases SIJ is source in 13-30% of chonic LBP Underappreciated cause of LB or buttck pain History of trauma in about 50% pts Athletes at risk – Unilateral loading: soccer, baseball, figure skating – Overuse: running, xcountry skiing, rowing • Pregnancy Differential Diagnosis • • • • • • Piriformis sydrome Hip joint pathology Discogenic pain Facet arthropathy Rheumatoid arthritis Ankylosing spondylitis • Trochanter pain syndrome • Visceral referral pain • Malignancy • Stress fracture • Radiculopathy Evaluation • Pain below the beltline – LBP, sacral, pelvic, gluteal • Less often numbness, popping, clicking, groin pain • Pain w/ transitional movements • Unilateral 4:1 • Pelvic obliquity: torsion/shear • SIJ provocative maneuvers • Normal neuro exam SIJ Provocative Maneuvers • Patrick’s Test – FABER – Flexion, Abd, ER – Positive: Pain contra SI • Gaenslen’s Test – Patient flexes hip and knee, holds – Examiner hyperextends contra hip – Positive: Pain HF side SIJ Provocative Maneuvers • • • • • Sacral sulcus tenderness Distraction/compression test Seated flexion test Standing Gillet’s Femoral shear test • Yoeman’s (Modified Gaenslen’s) Diagnostic Imaging • Generally not helpful • R/O other sources of pain – MRI – Bone scan – Plain radiographs • Intrarticular Diagnostics – Many consider guided injection gold standard – Clinical inj in office intraarticular in only 22% – More often periligamentous Treatment • • • • • • • Activity modification Ice, NSAIDs acutely Therapeutic Exercise SI Compression Belt Manual Therapy Therapeutic Cortisone Injection Regenerative Injection Therapy – Platelet Rich Plasma – Prolotherapy Somatic Dysfunction • Impaired or altered function of related components of the somatic system – skeletal, arthroidial, myofascial structures, related vascular, lymphatic, neural elements • Parameters -- Anatomic position determined by palpation, referenced to adjacent defined structure --Eval direction motion is restricted Restrictive (Pathologic) Barriers Limit of passive motion Anatomic barrier Limit of active motion Physiologic barrier Neutral Motion loss due to somatic dysfunction Pathologic (Restrictive) barrier OMT Techniques • • • • • • • • Thrust (HVLA) Articulatory (LVHA) Counterstrain Facilitated Positional Release Muscle Energy Myofascial Release Lymphatic Technique Visceral Manipulation Restrictive Barrier Soft - The elastic barrier; usually due to hypertonic muscles Responds well to MET, myofascial, counterstrain Hard - Firm barrier Responds well to HVLA, articulatory technique SIJ Dysfunction • Articulatory Treatment (ART): – Direct, passive technique – Low velocity / high amplitude – Dysfunctional joint is carried through its full ROM with an activating force of either springing or repetitive circular movement through the restrictive barrier SIJ Articulatory Technique Techniques • Muscle Energy – Direct, active technique – Patient activates muscle group against isometric resistance controlled position at restrictive barrier. – Post-isometric relaxation utilized to correct somatic dysfunction. Repeat into new barrier. Techniques • Counterstrain: – Indirect, passive technique – Local tenderpoint(s), inappropriate stretch reflex. – Reflex inhibited by placing body segment in position exactly opposite to strain, extinguish the tenderpoint. – Inappropriate afferent signaling from the intrafusal muscle fibers (induced by the stretch reflex) reset to baseline, leading to normalized ROM and function. New Treatment Concepts • Enthesis Organ • • Collection of related tissues at or near the enthesis For example, achilles – Osteotendinous junction – A sesamoid fibrocartilage – Periosteal fibrocartilage – Retrocalcaneal bursa – Sensory nerve endings EF=tendon insertion Benjamin et.al. J Anat. 2006 SF and P=fibrocartilage What is Regenerative Injection Therapy? • Prolotherapy, Platelet Rich Plasma • Injection therapy used to treat chronic ligament, joint capsule, fascial and tendinous injuries • Technique for healing ligament, tendon, and cartilage injury by stimulating the growth of normal cells and tissue in a specific location Klein RG. Patterson J. Eek and Zeiger D. Prolotherapy for The Treatment of Back Pain. AAOM Postion Statement Prolotherapy Injection Theoretical Basis • Proliferants cause local tissue injury at enthesis, release of inflammatory mediators. • Recruitment of granulocytes and macrophages • Fibroblasts deposit collagen at the site. • Collagen remodels ligament / tendon • Promotes healing cascade Proliferant Solutions • Osmotic shock agents – Hyperosmolar dextrose/glucose and glycerin • Irritants – Phenol • Chemotactic agents – Sodium morrhuate • Particulates – Pumice flour Research • • • • • • Liu YK: An in situ study of the influence of a sclerosing solution in rabbit medial collateral ligaments and its junction strength. Connect Tissue Res; Jan 01, 1983, 11(2-3): 95-102 Hoksrud, A., L. Ohberg, H. Alfredson, et al. Ultrasound-guided sclerosis of neovessels in painful chronic patellar tendinopathy: a randomized controlled trial. Am. J. Sports Med. 34:1738Y1746, 2006 Ongley MJ: A new approach to the treatment of chronic low back pain. Lancet; Jul 18, 1987, 2(8551): 143-6 Reeves KD: Randomized prospective double-blind placebo-controlled study of dextrose prolotherapy for knee osteoarthritis with or without ACL laxity. Alter Ther Health Med; Mar 2000, 6(2): 68-74, 77-80 Yelland MJ, Glasziou PP, Bogduk N, Schluter PJ, McKernon M. Prolotherapy injections, saline injections, and exercises for chronic low back pain: a randomized trial. Spine. 2004 Jan 1;29(1):9-16 YellandMJ, Mar C, Pirozzo S, Schoene ML, Vercoe P. Prolotherapy injections for chronic low back pain. Cochrane Database Syst Rev. 2004;(2): CD004059 PRP INJECTION • Platelet-Rich Plasma (PRP) injection therapy: – Injection of autologous plasma rich in platelets and growth factors into dysfunctional tissues Research • • • • • • • • • Holloway et al. Wounds 1993 R. Gfatter, et al; The mitosis of fibroblasts in cell cell culture is enhanced by Binding GP IIb-IIa of activated platelets on fibrinogen Platelets, Vol 1, 2000. Furerst et al. Oral Maxillofac. Implants. 2003 Anitua et al. New Insights into and novel applications for platelet rich fibrin therapies. Trends in Biotechnology 2006; 5:227-234 Sanchez et al. Comparison of surgically repaired Achilles tendon tears using platelet rich fibrin matrices. Am J Sports Med 2007;2:245-251 Mishra and Pavelko. Treatment of Chronic Elbow Tendinosis With Buffered Platelet-Rich Plasma. AJSM. 2006 Murray M, et al. J Ortho Res 2006 Sampson et al. Platelet rich plasma injection grafts for musculoskeletal injuries: a review. Curr Rev Musculoskelet Med 2008. K. Ali, C. Pocock, et al. Ultrasound guided dry needling and autologous blood injection for patellar tendinosis. Br. J. Sports Med. 41:51, 2007 Cochrane Database of Systematic Reviews 2006 • Treatments for Lower Back Pain – – – – – – – – – TENS Traction Heat or Cold NSAID Massage Lumbar supports Epidural, facet and local injections Exercise therapy Acupuncture ¾ Convincing evidence lacking THANK YOU!! Should all asymmetries be fixed?