Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hepatitis B wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Antibiotics wikipedia , lookup
Herpes simplex wikipedia , lookup
Henipavirus wikipedia , lookup
Orthohantavirus wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Neonatal infection wikipedia , lookup
Oesophagostomum wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Gastroenteritis wikipedia , lookup
Meningococcal disease wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Herpes simplex virus wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Leptospirosis wikipedia , lookup
Lymphocytic choriomeningitis wikipedia , lookup
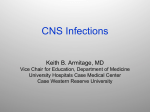
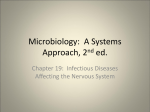
Alexander Saveriano PGY-4 Neurology General Principles Acute Meningitis ◦ Bacterial ◦ Viral Clinical presentation Causative organisms Treatment Complications Acute Encephalitis ◦ Common ◦ “Weird & Wonderful” Important to recognize the clinical syndromes of meningitis & encephalitis Remember the differential diagnosis ◦ NMS, SAH, stroke/CVST, PRES, toxic/metabolic encephalopathy, immune-mediated encephalitis Clinical severity ranges from benign to devastating Both host and pathogen factors influence clinical presentation and outcome Inflammation of the meninges “Pachy-” vs. “lepto-” Acute vs. subacute vs. chronic (>4 weeks) ◦ Time course depends on etiology Infectious categories: ◦ ◦ ◦ ◦ Account for most Bacterial acute meningitides Viral Fungal Mycobacterial Affects all ages, though incidence has declined (HIB vaccination) Mortality rate remains high ◦ 9.4% in children ◦ 20% or higher in adults Pathogen depends on age group and patient characteristics ◦ Knowledge of common pathogens guides treatment ◦ S. Pneumoniae responsible for majority of cases in all age groups except infants younger than 2 months ◦ Gram negatives responsible for 1/3rd of nosocomial cases “Triad” of fever, nuchal rigidity and altered mental status in 44% 95% have at least 2/4 classic signs/symptoms of headache, neck stiffness, fever and altered mental status Altered level of consciousness present in 2/3rds Presentation typically acute to hyper-acute (hours-1 day) Caveats: ◦ Headache may improve after LP ◦ Absence of nuchal rigidity, Kernig’s sign or Brudzinksi’s sign should never be used to exclude bacterial meningitis ◦ Children more likely to have a clear syndrome of otitis or URI before meningitis Rapid Succinct history: ◦ Time course ◦ Recent trauma/surgeries ◦ PMHx/meds (?immuno-compromised) Don’t forget antipsychotics ◦ Any suggestion of seizure? ◦ Behaviour changes? ◦ Recent infectious prodrome ◦ Travel, sick contacts, animal contacts Physical Examination ◦ ◦ ◦ ◦ ◦ ◦ Vitals Assess level of consciousness Assess for nuchal rigidity Assess for any lateralizing signs Dermatologic exam Cardio-resp exam Medical emergency Guiding principles: ◦ Rapid diagnosis (Hx, PE, LP) ◦ Administration of appropriate antibiotics as soon as possible ◦ Excluding structural brain lesions ◦ Identifying pathogen Delays in administration of antibiotics worsen outcomes, increase mortality Need urgent lumbar puncture – confirms diagnosis, identifies pathogen What about timing of scan? ◦ Abnormal CT in 24% (associated with age >60, immuno-compromise, seizure, focal deficits, inability to follow 2 consecutive commands) ◦ Absence of any of these findings has NPV of 97% considered safe to proceed with LP ◦ In practice in tertiary care centre, CT essentially always performed prior to LP ◦ Do not delay antibiotics for scan – start them, then send patient to scan What antibiotics to start? Why? Broad coverage – No margin for error here Ceftriaxone – Neisseria, most strep, H. Flu Vancomycin – Beta-lactam resistant strep Ampicillin – Listeria +/- Acyclovir – HSV coverage (Ddx) Practical dosing: Ceftriaxone 2 g IV q12h Vancomycin 30-45 mg/kg/day divided q812h (e.g. 1 g IV q12h), monitor levels ◦ Goal trough levels 15-20 mcg/ml Ampicillin 2 g IV q4h Yield of LP decreases within “hours” of antibiotic administration, not so with other CSF parameters Obtain blood cultures immediately before antibiotics ◦ Positive in 50% Don’t forget antibiotic prophylaxis for meningococcus (as early as possible!) ◦ Close contacts ◦ Family members/roommates Regimens include (adult dosing): ◦ Rifampin 600 mg po bid x 2 days ◦ Cipro 500 mg po x 1 ◦ Ceftriaxone 250 mg IM x 1 European trial of 301 patients randomly assigned to Abx alone or Abx + Dexamethasone 10 mg IV q6h x 4 days Primary endpoint death or neurological disability at 8 weeks Dexamethasone reduced mortality (7 vs. 15%) and disability (15 vs. 25%) ◦ All benefit seen in group with pneumococcal meningitis ◦ Should be given immediately before or with first dose of antibiotics ◦ Only to be continued if cultures confirms S. Pneumoniae Complications of bacterial meningitis 45F admitted to Medicine for confirmed bacterial meningitis. Received appropriate Abx with initial good clinical response. Several days later, Medicine senior calls because patient having worsening headache…asks to “please reassess”… Neurological complications in 28% Raised ICP/herniation Hydrocephalus Abscess formation Seizures (20%, negative prognostic indicator) Cranial nerve palsies Cerebrovascular disorders (stroke, venous thrombosis, arteritis, aneurysm formation) ◦ Hearing loss ◦ Cognitive impairment ◦ SIADH/Hyponatremia ◦ ◦ ◦ ◦ ◦ ◦ MRI/MRV performed: ◦ No abscess ◦ Transverse sinus thrombosis Most common cause of meningitis ~ “Aseptic meningitis” Symptoms of meningeal irritation ◦ ◦ ◦ ◦ Fever Headache Neck stiffness Photophobia Normal brain function ◦ Distinguishing feature from encephalitis Patients may be uncomfortable or distracted by headache, but they should not be encephalopathic per se Don’t forget ◦ ◦ ◦ ◦ Travel history HIV risk factors Animal/insect contact Dermatological exam Enterovirus family (esp. Late summer-Fall) HSV ◦ HSV2 an important cause of meningitis (30% of females with primary genital herpes infection) VZV HIV ◦ Inquire about HIV risk factors WNV Non-viral agents ◦ Lyme ◦ Syphillis ◦ Rocky mountain spotted fever “The classics” Inflammation of brain parenchyma Infectious vs. Post-infectious/immunemediated May be concurrent with meningeal irritation (“meningo-encephalitis”) Symptoms and signs of disturbed cerebral function, in addition to infectious “clues” ◦ ◦ ◦ ◦ Altered mental status/behavioural changes Seizures Fever Headache Extensive list of viral etiologies ◦ ◦ ◦ ◦ ◦ ◦ ◦ HSV VZV Eastern Equine Encephalitis St. Louis Encephalitis WNV CMV (esp. HIV patients) Enterovirus (esp. Rituxan patients or IgG def.) ◦ ◦ ◦ ◦ Treponema Mycoplasma Listeria Rickettsia Non-viral agents: 21-year-old woman on her way to college reports smelling an unusual, unpleasant odor that was unapparent to everyone else in her family. Upon arriving at college, she went to bed. Her roommate was unable to waken her the next morning, and she was brought to the emergency department. Neurologic examination: Deeply somnolent, no response to voice, some reaction to pain No neck stiffness and optic discs flat Left-sided hyperreflexia and left Babinski sign CSF: 41 RBC, 327 WBC (87% lymphs), Ptn 1.8, glucose WNL Encephalitis and Postinfectious Encephalitis Greenlee, John E. CONTINUUM: Lifelong Learning in Neurology. 18(6, Infectious Disease):1271-1289, December 2012. doi: 10.1212/01.CON.0000423847.401 47.06 Copyright © 2013 American Academy of Neurology . Published by Lippincott Williams & Wilkins. 37 ◦ ◦ ◦ ◦ ◦ ◦ ◦ HSV Neurosyphillis WNV VZV EBV HHV6 Congenital CMV 10-15% of viral encephalitides Male=Female No seasonal variation May occur at any age HSV1 implicated in 90% of cases Predilection for orbitofrontal and temporal lobes Cingulate gyrus commonly involved as well Unilateral or bilateral Involvement of other areas of cortex or brainstem without temporal lobe involvement does not exclude HSV Diagnosis confirmed with HSV PCR in CSF 98% diagnostic accuracy Yield falls to 21% after 2 weeks of therapy Possible to be falsely negative very early in disease ◦ Repeat in 4-7 days Acyclovir – Inhibits HSV synthesis by causing DNA chain termination Shown to reduce mortality ◦ 70% -> 28% 10 mg/kg IV q8h for 21 days Start early! Many have lasting complications of disease ◦ Epilepsy ◦ Cognitive/behavioural disorders 73F known DM2, renal impairment presents with 2-day history of headache, followed by increasing somnolence. On arrival to ER, she is drowsy and is febrile at 38.4. She is started on antibiotic and antiviral therapy. LP done-> 140 WBC (60% PMN), Ptn 1.1, glucose WNL In the ensuing hours, she becomes increasingly obtunded, requiring intubation Admitted to ICU Exam reveals comatose woman with intact brainstem exam, up-going plantars and cogwheel rigidity in the upper extremities MRI FLAIR sequence depicting basal ganglia hyperintensities MRI FLAIR sequence depicting hyperintensities in the midbrain and right mesial temporal lobe HSV PCR negative CSF bacterial cultures negative West Nile serology positive 10-14 days later Season runs from June – November Peak in late August Life cycle links mosquitoes, birds and humans ◦ Mosquito vector bites & infects bird... ◦ Bird serves as excellent host for replication of virus... ◦ Bird infects more mosquitoes... ◦ Which then infect humans History of mosquito bite not always present Travel to endemic areas (?) 5-15 day incubation About 20% become symptomatic ◦ Fever, headache, malaise, myalgias, rash, vomiting, back or limb pain ◦ Lasting 3-6 days Neurological complications typically arise days after systemic symptoms 3 syndromes of neuro-invasive disease ◦ Aseptic Meningitis ◦ Meningoencephalitis ◦ Acute flaccid paralysis Affects 1/150 of those infected Elderly & immune-compromised at highest risk ◦ Median age 70 Symptomatology: ◦ ◦ ◦ ◦ ◦ ◦ Confusion Disorientation Fever Behavioural changes Movement disorders/Parkinsonism Weakness “Classic” CSF profile: ◦ Pleocytosis (neutrophilic predominance in 37-45%) ◦ Elevated protein ◦ Normal glucose West Nile Serology (IgM/IgG) ◦ Serum or CSF Ferritin levels (?) ◦ Elevated in cases of WNV encephalitis, but not other encephalitides Study of 16 cases of WNV meningoencephalomyelitis with MR imaging ◦ 5 normal ◦ 11 abnormal 3 with “ischemic” changes on DWI 8 with “lesions in the basal ganglia, mesial temporal lobe, thalami, midbrain, pons, cerebellum, and hemispheric white matter” Supportive care ◦ Intubation ◦ Prevention of secondary infection No specific medication shown to be of benefit Acyclovir to cover possibility of HSV Development of limb weakness with dramatic progression over 48 hours Asymmetric Hypo/Areflexia Absence of sensory symptoms Bladder dysfunction common May occur in isolation or in combination with other neurological manifestations 76F seen 3 weeks ago for vesicular rash around L. Eye along with corneal involvement. She now presents with new-onset R. hemibody weakness and confusion On exam, she is mildly febrile (38.1) with a mild expressive aphasia and R. hemiparesis and hyperreflexia CT head shows multifocal L. hemispheric infarcts with hemorrhagic component Ideas? Occurs more often than previously recognized ◦ 15% of encephalitis where cause identified (Mailles et al., 2007) ◦ Most common cause after HSV in immunocompetent ◦ Even more common in immunocompromised Infects endothelial cells of small and large vessels (vasculopathy) Can lead to focal/multifocal ischemia or even aneurysm formation and hemorrhage “Classic” case is that of herpes zoster ophthalmicus, followed days-weeks later by a stroke with contralateral hemiparesis May occur without rash Immunocompromised state is a risk-factor Diagnosis by detection of VZV IgG in CSF PCR also available, but –ve test does not exclude VZV encephalitis Treatment with Acyclovir The Weird and [not so] Wonderful 42 year-old male presents to ER with “confusion” and bizarre behaviour. He was seen and discharged about 1 week ago for symptoms of myalgias, headache and malaise. For the past 2 days he has been increasingly aggressive and incoherent. His wife reports that he did not sleep all night. On exam, he is agitated, combative, and drooling He periodically grabs his throat and appears to be in severe discomfort There is no focal weakness, though he is diffusely hyperreflexic and plantar responses are extensor. Anything else you would like to know on history/exam? ◦ Travel to Africa 1-2 months ago, travelled through rural villages ◦ Bitten by dog, sought local medical care Lyssavirus Predilection for neural spread Animal reservoir (dogs, bats, cats, skunks, foxes, etc.) 30,000-70,000 deaths per year worldwide ◦ Mostly developing countries ◦ 2 cases/year in USA Transmission: ◦ Exposure to saliva of infected animal ◦ Non-saliva exposure (aerosolized virus in bat caves) ◦ Transplanted tissue from infected patients Incubation 1-3 months (range from days to 1 year) 2 clinical stages of disease ◦ Prodromal ◦ Clinical rabies Prodromal symptoms are non-specific, viral ◦ Paresthesiae radiating proximally from wound would be suggestive May see percussion myoedema ◦ Mounding of muscle around percussion site 2 variants of “clinical rabies” ◦ Encephalitic (“Furious”) rabies – 80% ◦ Paralytic (“Dumb”) rabies – 20% Hydrophobia (33-50%) “After some preliminary feeling of discomfort in the throat or dysphagia, the patient suddenly develops an overwhelming terror of water based on involuntary pharyngeal muscle spasms during attempts to drink. Later in the disease, even the sight or mention of water may trigger these involuntary spasms.” Aerophobia – Also pathognomonic, less common (9%) Opisthotonus ANS instability Combativeness/aggression Ascending paralysis (GBS mimic) Flaccid paralysis, usually most apparent in bitten limb Absent DTRs, may see fasciculations Hydrophobia unusual Late cerebral involvement Diagnosis usually requires multiple tests ◦ ◦ ◦ ◦ Serum and CSF antibodies Isolation of virus from saliva Skin biopsy Pathologic hallmark – Negri Body Traditionally uniformly fatal disease “Best treatment is prevention” Pre-exposure vaccination Post-exposure prophylaxis ◦ High-risk groups (vets, travelers to endemic areas where contact with wildlife likely) ◦ Vaccine ◦ Rabies immunoglobulin 52M 3 ½ weeks post HSCT Neurology team called to assess for “confusion” for several days Pt reports some headache On exam, he is afebrile, has a supple neck, and is awake. He is disoriented and anterograde amnesia is evident. Remainder of exam non-focal Routine blood work relatively unremarkable Team asks for CT head -> “Normal” What next? ◦ LP: WBC 4 (lymphs), RBC 2, Ptn and glucose WNL ◦ HSV PCR sent ◦ Started empirically on Acyclovir Ubiquitous neurotropic virus Usually acquired early in life No clear adverse effects in immunocompetent adults Recently identified as an important cause of encephalitis in the immunocompromised host ◦ Specifically allogenic stem cell transplant patients Onset of anterograde amnesia, headache, confusion 2-6 weeks after SCT Seizures common as well (40-70%) CSF profile normal or only mildly abnormal ◦ Median cell count = 5 MRI ◦ T2/FLAIR hyperintensities in mesial temporal lobes ◦ Diffusion restriction may be seen as well Diagnosis established by viral CSF PCR Treatment with ganciclovir or foscarnet appears to be beneficial ◦ Optimal duration of therapy not known Little information regarding natural history Seems to be associated with worse prognosis after SCT (Bhanushali et al., Neurology, 2013) ◦ Not necessarily as direct result of encephalitis Do not delay antibiotics when considering bacterial meningitis (do not wait for CT/LP) Multiple neurological complications of bacterial meningitis Not all viral meningitis is enterovirus ◦ Remember travel history, animal/insect contacts, HIV risk factors Treat HSV encephalitis promptly with acyclovir Not all mesial temporal lesions are HSV, and not all HSV is in the mesial temporal lobe VZV may be an under-recognized cause of meningitis or encephalitis Rabies is an important cause of encephalitis in the developing world Remember WNV during Summer & Fall HHV-6 is an important cause of encephalitis in the immunocompromised patient, with its own treatment ◦ Don’t be fooled by “normal” CSF