Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
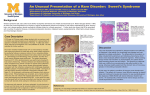
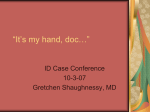
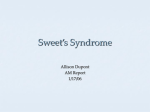
The Sweet Spot: A Case of Unusual Rash Associated with Cutaneous Trauma LT Laura Gilbert, MD, Associate CPT Nate Copeland, MD, Associate Catherine F. Decker, MD, Fellow Navy ACP Conference Walter Reed National Military Medical Center October 17, 2014 Case Presentation • 68yF presents with diffuse erythematous, non-pruritic and painful lesions involving face, legs, chest, and back • Endorses low grade fever • Placed on TMP-SMX post I/D of a left axillary MRSA abscess nine days PTA Past Medical/Surgical History • GERD, hyperlipidemia, overactive bladder • Hysterectomy • Left total knee arthroplasty Jan 2014 – Complicated by post-op MRSA joint infection in Mar 2014 • Left axillary MRSA abscess s/p I&D Aug 2014 – Started on TMP-SMX 9 days prior to presentation Social History • • • • • Non-smoker, rare alcohol, no IV drug use Originally from Thailand No recent travel, sick contacts or tick exposure Swimming in pool 4 days prior to presentation Dog at home, no new pet or animal exposure Medications • Outpatient Medications: – – – – – – Atorvastatin Aspirin Esomeprazole Conjugated Estrogen Solifenacin Succinate TMP-SMX • Allergies: – Shellfish Physical Exam • • • • Vital signs: afebrile HEENT: no conjunctival injection, oral ulcers Extremities: no edema Skin: Laboratory Data • Complete blood count: – WBC 9.9K, Hgb 11.9 g/dL, Plt 36K (repeat - 22K) • Serum chemistry: normal • Urinalysis: normal • ESR: 43 mm/hr • CRP: 9.475 mg/dL • Skin biopsy: Neutrophilic Dermatosis: Differential Diagnosis • Infections – Bacterial, Fungal, Mycobacterial • Inflammatory diseases – Vasculitis: Polyarteritis nodosa – Erythema nodosum, Pyoderma gangrenosum – Acne fulminans, Psoriasis – Cutaneous Sarcoidosis – Behçet's disease – Sweet Syndrome Sweet Syndrome • First described in 1964 – “Acute febrile neutrophilic dermatosis” – Initially called GommButton disease – First reported druginduced case in 1986 • TMP-SMX Characteristics • Fever with characteristic rash and pathology – Neutrophilic dermatosis without vasculitis – Rash: painful, raised erythematous papules • 3 Major classifications – Classical – Malignancy-associated – Drug-induced Classification • Classical – Infections, Inflammatory Bowel Disease, Pregnancy • Malignancy-associated • Drug-induced – Granulocyte-colony stimulating factor, antibiotics, chemotherapy Clinical Features Cohen PR. Sweet’s syndrome – a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007 Jul; 2:34. Diagnostic Criteria: Drug-induced • Sudden onset of painful, erythematous nodules • Neutrophilic infiltration of dermis without vasculitis • Fever > 38 C • Relationship between drug ingestion and symptoms • Improvement in symptoms after discontinuation of medication or treatment with steroids Pathophysiology • Not well understood • Hypersensitivity reaction – Immune reaction to antigen: activation cytokines and PMNs • Cytokine dysregulation • Genetic susceptibility – HLA B54 linked to Sweet in Japanese women Management • Removal of inciting drug if applicable • Treatment of underlying condition • First line agents: – oral steroids or potassium iodide • Second line agents: – Dapsone or Colchicine Hospital Course • TMP-SMX and Aspirin were discontinued • Dermatology recommendation: no oral steroids • Daily CBC – Platelet count recovered to 118K by HD 3 • Decrease in erythema • Recommended age-appropriate cancer screening • TMP-SMX was listed as an allergy Sweet Syndrome and Pathergy • Definition: hyper-reactivity of the skin in response to cutaneous trauma • Rare association with Sweet syndrome – Case reports associated with burns, radiation, biopsy site, bites, surgical scars • First documented case of Sweet syndrome associated with non-acute trauma? Conclusion • Sweet syndrome mimics a variety of diseases characterized by rash and a fever • Association with malignancy and drugs • Biopsy is essential for diagnosis • Treatment with oral steroids is gold standard • Pathergy is rare clinical manifestation of Sweet syndrome associated with cutaneous trauma References • • • • • • • • • • • Awan F, Hamadani M, Devine S. Paraneoplastic Sweet’s Syndrome and the pathergy phenomenon. 2007; 86:613-614. Bi XL, Gu J, Yan M, Gao CF. A case of Sweet's syndrome with slack skin and pathergy phenomenon. Int J Dermatol. 2008 Aug; 47(8):842-4. Callen JP. Neutrophilic Dermatosis. Derm Clinics. 2002 Jul; 20:3. Cohen PR. Sweet’s syndrome – a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007 Jul; 2:34. De Moya MA, Wong JT, Kroshinsky D, Robbins GK, Shenoy-Bhangle AS, Gimbel DC. Case records of the Massachusetts General Hospital. Case 28-2012. A 30-year-old woman with shock and abdominal-wall necrosis after cesarean section. N Engl J Med. 2012 Sep 13; 367(11):1046-57. Minocha R, Sebaratnam D, Choi J. Sweet’s Syndrome following surgery: cutaneous trauma as a possible aetiological co-factor in neutrophilic dermatosis. Australias J Derm. Online publication: March 11, 2014. O’Halloran E, Stewart N, Vetrichevvel TP, Rea S, Wood F. Sweet’s syndrome mimicking alkali burn: a clinical conundrum. J Plast Reconstr Aesthet Surg. 2013 Jun; 66(6):867-869. Ramos I, Wiering C, Tebcherani A, Sanchez A. Sweet’s syndrome on surgical scar. An Bras Dermatol. 2006; 81(5):S324-6. Sweet RD. Br J Dermatol. 1964; 76:349-356. Varol A, Seifert O, Anderson C. The skin pathergy test: innately useful? Arch Dermatol Res. 2010; 302:155-168. Walker DC, Cohen PR. Trimethoprim-sulfamethoxazole-associated acute febrile neutrophilic dermatosis: Case report and a review of drug-induced Sweet’s Syndrome. J Am Acad Derm. 1996; 34:918-923. Thank you!