Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
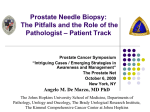
european urology 54 (2008) 728–739 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review – Prostate Cancer Does the Extent of Carcinoma in Prostatic Biopsies Predict Prostate-Specific Antigen Recurrence? A Systematic Review Patricia Harnden a,*, Michael D. Shelley b, Brian Naylor c, Bernadette Coles b, Malcolm D. Mason d a Cancer Research UK Clinical Centre, St James’s University Hospital, Beckett Street, Leeds LS9 7TF, United Kingdom Cochrane Urological Cancers Unit, Velindre NHS Trust, Cardiff, CF14 2TL, United Kingdom c Histopathology, Airedale General Hospital, Keighley, United Kingdom d Cardiff University, Cardiff, CF10 1AA, United Kingdom b Article info Abstract Article history: Accepted June 16, 2008 Published online ahead of print on June 26, 2008 Context: The biologic potential of prostate cancer (pCA) is variable, and the ability to identify tumours that might cause morbidity and mortality is limited. Objective: This systematic review sought to establish whether measurement of tumour extent in biopsies provides additional prognostic information on the risk of disease progression. Evidence acquisition: A comprehensive 31-step search strategy was run in MEDLINE, EMBASE, and the Web of Knowledge (January 1990–July 2007) and supplemented by the hand-searching of references in retrieved articles and relevant journals to identify publications related to the measurement of the length of cancer in biopsies and biochemical or clinical recurrence or pCA death. Thirteen papers reporting on at least 100 patients were identified and included patients treated by watchful waiting or hormonal therapy (n = 1), radical prostatectomy (n = 11), or radiotherapy (n = 1). Only two studies reported on clinical progression or mortality. Sources of bias included patient selection and missing data resulting from the retrospective nature of the studies. Confounding factors included differences in biopsy strategies and measurement methods. Evidence synthesis: The percentage of cancer in biopsies (overall percentage or the greatest percentage in the most involved core) was an independent predictor of prostate-specific antigen (PSA) and clinical outcomes regardless of the form of treatment and was generally superior to simply counting the number of positive cores. The marked variability in study design, conduct, and reporting precluded meta-analysis of the data and precise risk estimation. Conclusions: Tumour quantitation is a promising prognostic tool in the assessment of risk of pCA progression. However, well-designed, population-based studies, controlling for confounding factors, are required to provide more accurate risk estimation and develop management strategies. This review highlights the need for new approaches in the assessment of pathologic prognostic factors to reach the level of evidence achieved in other areas of medical practice. # 2008 Published by Elsevier B.V. on behalf of European Association of Urology. Keywords: Prostate cancer Biopsy prognostic factors Tumour extent * Corresponding author. Bexley Wing, St James’s University Hospital, Leeds LS9 7TF, United Kingdom. Tel. +44 (0) 113 2067531; Fax: +44 (0) 113 2067610. E-mail address: [email protected] (P. Harnden). 0302-2838/$ – see back matter # 2008 Published by Elsevier B.V. on behalf of European Association of Urology. doi:10.1016/j.eururo.2008.06.068 european urology 54 (2008) 728–739 1. Introduction One of the major problems facing urologic oncologists and urologists today is how and when to treat asymptomatic men with prostate cancer (pCA). Offering radical therapy is associated with potential morbidity resulting from urinary, bowel, and sexual dysfunction [1–4]. Active surveillance, whereby treatment with curative intent is only instituted if there are signs of progression, is seen as a viable option to avoid ‘‘over-treatment’’ [5] and is most appropriate for patients at low risk of progressive disease. Assessing the magnitude of this risk in individual patients remains a challenge, as current nomograms [6–8] and risk tables [9,10], incorporating pretreatment prostate-specific antigen (PSA) levels, Gleason score, and stage of disease provide relatively wide estimates. More detailed biopsy information, particularly the percentage of positive cores, is used in clinical practice to refine risk assessment, particularly for low-risk patients [11– 18], and these predictive tools have been validated [19,20]. However, methods of estimating the linear length of cancer have varied among studies, with no consistency in approach even among dedicated uropathologists [21], and these measurements are used with caution by urologists [22]. The aim of this systematic review was to identify and summarize all studies relating linear extent of cancer on biopsy with recurrence, progression, or death from pCA and to determine which, if any, of these pathologic variables should be reported in routine practice to stratify patients into groups at different risk of progression. It also sought to establish whether these more complex measurement methods were superior to the simple measure of counting the number of positive cores. 2. 729 Methods A comprehensive 31-step search strategy was developed composed of a thesaurus and text-word terms describing pCA, outcomes, and pathology to identify studies reporting the pathology of pCA [23]. There were no language restrictions. The initiation of the search date (1990) coincided with the establishment of transrectal ultrasound (TRUS)-guided biopsy procedures and was updated to July 2007. The resulting bibliographic database (Fig. 1) was then searched using biopsy as a search term. Two authors scanned titles and abstracts for relevant studies. Only fully published studies were retrieved for further assessment. The electronic search was supplemented by hand-searching bibliographies of the retrieved papers and relevant recent cancer journals. A sample size of 100 patients was considered a minimum for meaningful statistical analyses. Papers addressing the specific issue of microfocal carcinoma were reviewed sepa- Fig. 1 – Flow diagram for evidence search. rately [24]. The selection process resulted in 13 papers examining the relationship of the absolute length (in millimetres) [25–27] or the relative length (percent) [28–37] of cancer in biopsy material with pCA mortality, clinical recurrence, or PSA recurrence. Two groups reported initial [29,34] and extended [30,33] follow-up data on overlapping groups of patients. The early reports are included, as they took a different analytic approach and contain comparative data on the significance of the number of positive cores. All were retrospective studies except one in which some of the data were collected prospectively [33]. Data were extracted and verified by at least two authors and consisted of study design and location, patient characteristics, details of biopsy pathology and method, types of interventions, statistical analysis, and clinical and/or PSA outcomes. Additional information concerning the measurement method was requested from the authors when required and was received in all but one case [35]. 3. Results 3.1. Measurements expressed in millimetres The study characteristics and findings of the three relevant papers [25–27] are summarized in Tables 1 730 european urology 54 (2008) 728–739 Table 1 – Characteristics of studies examining the length of cancer (in millimetres) in prostatic biopsies Study Institution (dates) n Stage Age (years) 178 T1 = 92 T2 = 70 T3 = 16 Mean: 64.9 (49–80) Median: 7.9 (1.2–136.0) <6 = 4% 6 = 54% >6 = 42% 6 = 44% 7 = 35% 8–10 = 21% Median: 41.5 (2.0–82.0) King et al, 2005 [26] Kitasato and Kurashiki Hospitals. 1992–1999 Stanford University and Palo Alto Veterans Hospital 1992–2001 124 ND Mean: 60.6 (39.9–73.1) 6 = 67% 8 = 19% 7–13 = 14% 6 = 58% 7 = 25% 8–10 = 17% ND Noguchi et al, 2003 [27] Stanford University 1998–1997 222 T1c Mean: 62.5 (43–79) 4 = 9% 4.1–10 = 65% 10.1–20 = 17% >20 = 10% 4 = 2% 4.1–10 = 72% 10.1–20 = 25% >20 = 1% Median: 6 (6–13) ND Mean: 52.4 (6–152) Egawa et al, 2001 [25] PSA ng/ml Biopsy number Gleason score Follow-up (months) ND, no data; PSA, prostate-specific antigen. and 2. All patients were treated by radical prostatectomy. 3.4. Relative value of the number of positive cores versus cancer length (in millimetres) 3.2. One study found that only the number of positive cores was significantly associated with biochemical recurrence [27] and another that it was also predictive [25]. Both of these studies dichotomized this variable, whereas the third, reporting negative results, did not [26]. The values were widely spread in this study (range: 1–11), and there were relatively few cases with three (19%) or four or more (15%) positive cores [26]. Cumulative cancer length (sum of cancer in all cores) In the report by King et al [26], values were spread across a wide range (1–44 mm), with cumulative lengths of cancer >9 mm in 43% of patients, and only this measure was significantly associated with biochemical recurrence (Table 2). Noguchi et al reported negative results [27]; 36% of patients had a cumulative cancer length of 3 mm, 30% had values of 3.1–6 mm, 13% had values of 6.1–9 mm, and only 21% had >9 mm of cancer. In the first study, cumulative length was analyzed as a continuous variable, but in the negative study, the mean value (6 mm) was used as the cut-off point. The skewed distribution and the choice of cut-off points may explain the negative findings. 3.3. Maximum length of cancer in any one core Maximum length of cancer in any one core was predictive of biochemical failure in the study by Egawa et al [25] but not that of King et al [26]. In this case, the use of a cut-off point resulted in a significant result [25], which was not reproduced when data were analyzed as continuous variables [26]. When patients were then stratified into three risk groups depending on clinical stage, presenting serum PSA levels, and biopsy Gleason score [25]— which were further subdivided (one positive biopsy and <3 mm of cancer, one positive biopsy or <3 mm, two or more positive biopsies, and 3 mm of cancer)—there was no improvement in risk stratification for PSA recurrence. However, the maximum number of patients in any of these subgroups was 39, and the statistical power may have been insufficient to detect a significant difference. 3.5. Cancer lengths expressed as a percentage The key characteristics of these 10 studies [28–37] are summarised in Table 3. The different methodologies are detailed in Table 4, and the findings are presented in Table 5. 3.6. Total percentage of cancer Cuzick et al reported on pCA mortality in patients treated conservatively after a diagnosis made either in transurethral resections or biopsy cores [28]. There were no data specific to measurement in biopsy material, but overall, the total percentage of cancer was more predictive for pCA death at 10 yr than clinical stage in multivariate models, although the major factor predictive of cancer mortality was Gleason grade followed by PSA levels. In the remaining papers, all patients underwent radical prostatectomy. Using the Shared Equal Access Regional Centre Hospital (SEARCH) database, Freedland and coworkers [29] reported that the total percentage of cancer was the strongest predictor of PSA recurrence when analyzed as a continuous value but was similar to other predictors as a categorical variable Number positive: 2.54 (1.04–6.20), p = 0.041 3.7. Relative value of the percentage of positive cores versus total percentage of cancer PSA, prostate-specific antigen; CI, confidence interval; mm, millimetres. Multivariate Cox proportional hazards model 0.07 ng/ml, increasing in subsequent samples/39 (18%) Noguchi et al, 2003 [27] Multivariate logistic regression analysis Detectable postoperative PSA >0.05 ng/ml/28 (24%) 1. Total cancer length on biopsy (mm) 2. Maximum tumour length (mm) 3. Number of positive cores 4. Percent of positive cores 1. Total cancer length on biopsy (<6, 6 mm) 2. Number of positive cores (<2, 2) King et al, 2005 [26] 731 (Table 5). When added to baseline PSA levels and Gleason score data to predict PSA recurrence, the area under the receiver operating characteristic curve (AUC) increased significantly from 0.653 to 0.722 ( p = 0.020). The optimized cut-off points (Table 4) also significantly improved risk stratification for PSA recurrence within risk groups defined by serum PSA and biopsy Gleason score (low risk: PSA 10 ng/ml and biopsy Gleason score <7; intermediate risk: PSA 10–20 ng/ml and biopsy Gleason score 7; high risk: PSA >20 ng/ml or biopsy Gleason score >7). These researchers then developed a preoperative model for the 2-yr risk of PSA recurrence following radical prostatectomy [30], using cut-off values for the percent of cancer on biopsy (<20%, 20–40%, and >40%), serum PSA (<10, 10–20, >20 ng/ml), and biopsy Gleason score (<7, 3 + 4, 4 + 3). For a patient with a Gleason sum score of 3 + 4 and a preoperative serum PSA level of <10 ng/ml, the risk of biochemical failure increased from 13% (95% CI, 10–16) if <20% of cancer was present on biopsy to 30% (95% CI, 13–47) if >40% of the tissue was involved. Sebo et al [37] and Ravery et al [36] demonstrated that the total percentage of cancer was predictive of PSA recurrence in univariate analysis [37] or by log-rank test [36]. Except for PSA density, all other preoperative parameters (age, clinical stage, PSA, Gleason score, the percentage of positive cores, and whether cancer was unilateral or bilateral) were not significantly associated with biologic progression. Neither factor significant in univariate analysis, number positive significant on multivariate analysis No details No details Both measures in conjunction with PSA, stage, and Gleason score significantly improved prediction of biochemical failure ( p = 0.009) Only total cancer length significant ( p = 0.05) Likelihood ratio test 2 consecutive rises 0.1 ng/ml, 1 mo apart/58 (33%) 1. Maximum length of cancer (<3 or 3 mm) 2. Number of positive cores (1 or >1) Egawa et al, 2001 [25] Statistical analyses Definition of PSA Recurrence/ number (%) of recurrences Measures reported Study Table 2 – Summary of findings of papers investigating the length (in millimetres) of cancer on biopsy Correlation with PSA recurrence Hazard ratio (95% CI), p value european urology 54 (2008) 728–739 One group compared the predictive value of the total percentage of biopsy tissue containing cancer with the percentage of positive cores, analyzing both variables as continuous and categorical variables [29]. There was a significant correlation between the two measures (Spearman rank: r = 0.778, p < 0.001), and the difference in the area under the receiver operating characteristic curve (AUC) was slight (percentage of cancer: 0.697; percentage of positive cores: 0.644) although statistically significant in favour of the percentage of cancer (no confidence intervals given, p = 0.022). The percentage of positive cores was also not independently predictive in another study [36] and was not tested in another multivariate model [37]. 3.8. Greatest percentage of cancer An initial study by Nelson and colleagues [34] found that the preoperative variables influencing recur- 732 Table 3 – Characteristics of studies examining the percentage of cancer in prostatic biopsies Study Institution (dates) Stage 1656, but ND for biopsy subgroup 355 ND for biopsy subgroup Median: 70.1 (44–76) T1 = 165 T2 = 184 T3 = 1 T1 = 224 T2 = 228 T3 = 1 All T1c Mean: 61.8 4 = 23% 4–10 = 21% >10 = 56% Median: 7.9 Mean: 61.8 Median: 7.8 ND Cuzick et al, 2006 [28] Six UK registries, 1990–1996 Freedland et al, 2003 [29] SEARCH database, 1990–2002 Freedland et al, 2004 [30] SEARCH database, 1990–2002 459 Gretzer et al, 2002 [31] John Hopkins Hospital, Baltimore, MD, USA, 1988–2000 Brigham & Women’s Hospital, Boston, MA, USA, 1989–2000 University of Michigan Hospitals, Ann Arbor, MI, USA, 1994–1998 University of Michigan Hospitals, Ann Arbor, MI, USA, 1994–2002 Memorial Sloan Kettering, New York, NY, USA, 1992–1999 Bichat Hospital, Paris, France, 1988–1998 Mayo Clinic, Rochester, MN, USA, 1995–1998 243 for percentage of cancer Linson et al, 2002 [32] Nelson et al, 2002 [34] Nelson et al, 2003 [33] Potters et al, 2002 [35] Ravery et al, 2000 [36] Sebo et al, 2002 [37] 184 588 T1c = 125 T2a = 31 T2b = 28 T1 = 413 T2 = 175 Age (years) PSA ng/ml Biopsy number Gleason score Primary treatment 6 = 32% 7 = 21% 8–10 = 18% Median: 6 Hormones/ WW (670/1663) Median: 117 (88–180) RP Median: 34 Median: 8 (4–19) Mean: 6 RP Median: 34 ND for relevant subgroup ND ND for relevant subgroup RP ND ND >10– <20 6 <6–7 RP Median: 33 (6–120) <55 = 28% 55–66 = 50% >66 = 22% Mean: 60.2 7.6 10 = 82% >10 = 18% ND 6–9 RP Mean: 16 (4–48) Mean: 7.7 7.2 ND 2–10 RP Median: 37 (2–99) ND Median: 8 (4–18) Follow-up (months) 1414 T1 = 898 >T1 = 502 1073 T1c = 641 T2a = 377 T2b = 55 Median: 69.8 Median: 7.6 (0.17–112) 6 2–10 Brachytherapy Median: 34.7 (6–91) 143 T1–T2 Median: 63 ND Median: 7 RP 454 97.7% confined clinical stage Median: 65 Median: 10.5 (1.4–61.8) Median: 6.3 (0.6–112.0) Mean: 6.6 (2–14) Median: 6 (4–9) RP Median: 40 (6–112) Mean: 3.4 (17 d–5.8 yr) PSA, prostate-specific antigen; ND, no data; RP, radical prostatectomy; WW, watchful waiting. european urology 54 (2008) 728–739 n 733 european urology 54 (2008) 728–739 Table 4 – Methods for the measurement of the percentage of cancer Study Terminology Measurement method Intervening benign tissue excluded Cuzick et al, 2006 [28] Percent of cancer in biopsy Sum of cancer lengths in each core/sum of each core length Yes Freedland et al, 2003 and 2004 [29,30] Gretzer et al, 2002 [31] Percent cancer in biopsy Sum of cancer lengths in each core/sum of each core length Yes Maximal percentage of biopsy core with cancer No Linson et al, 2002 [32] Percentage of core length with cancer Nelson et al, 2002 and 2003 [33,34] Greatest percentage of cancer Estimate of the linear amount of cancer in the single most involved core Sum of lengths of cancer in each core/number of cores (assumed that all are of the same length) Estimate to the nearest 5% of the linear percent of cancer in the single-most involved core Potters et al, 2002 [35] 1. Mean percent cancer in an involved core 2. Maximum percent cancer in any core 3. Percent cancer at apex, midgland, or base 4. Maximum percent of cancer at apex, midgland, or base Length of core invaded by cancer ND ND Sum of cancer lengths in each core/sum of each core length Visual estimate in 5% increments of the amount of tumour relative to the total length of cores Yes, yes, also periprostatic tissues Yes, yes Ravery et al, 2000 [36] Sebo et al, 2002 [37] Percent surface area involved with cancer Yes Yes Cut-off points 6%, >6–20%, >20–40%, >40–75%, >75–100% Continuous variable and <20%, 20–40%, >40% Continuous variable and <50% vs >50% 25% vs >25% 2002: Stratification by 10% intervals and <10%, 10–59%, 60% 2003: 60–100% vs 0–59% Continuous variables <15%, 15–29%, 30–49%, 50–100% Continuous variables ND, no data. rence-free survival after radical prostatectomy were serum PSA ( p < 0.01) as a continuous variable, biopsy Gleason score (<7, 7, >7, p = 0.04), and the greatest percentage of cancer ( p < 0.01). Using these three parameters, a multivariate model was highly predictive of recurrence-free survival ( p = 0.0001). For a patient with Gleason sum score of 7 and a preoperative serum PSA level of 10 ng/ml, the 2-yr risk of biochemical failure increased from 5% (95% CI, 1–10), if the greatest percentage was <10%, to 16% (95% CI, 10–21), if it was 60%. The extended study [33] also demonstrated that the greatest percentage Table 5 – Summary of findings of papers investigating the percentage of cancer on biopsy Study Cuzick et al, 2006 [28] Freedland et al, 2003 [29] Reported outcomes; number (%) Death from pCA; ND (24%) Biochemical failure: PSA >2 ng/ml or two values of 2 ng/ml; 89 (25%) Statistical analyses Multivariate PHM Multivariate CPHM Correlation with reported outcomes Percent cancer significant in univariate and multivariate analysis Percent cancer as a continuous variable stronger independent predictor of PSA recurrence than biopsy Gleason score and serum PSA. Percent of positive cores not independent predictor. Hazard ratio (95% CI), p value No details for biopsy subgroup 8.25 (3.06–22.22), p < 0.001 compared to: Gleason score 1.34 (1.11–1.62) p = 0.003 PSA 1.03 (1.01–1.05), p = 0.003 734 european urology 54 (2008) 728–739 Table 5 (Continued ) Study Reported outcomes; number (%) Statistical analyses Correlation with reported outcomes Freedland et al, 2004 [30] Biochemical failure: PSA >2 ng/ml or 2 values of 2 ng/ ml; 118 (26%) Logistic regression and CPHM Using cut-offs, percent of cancer significant independent predictor of PSA failure similar to biopsy Gleason score and serum PSA Gretzer et al, 2002 [31] Biochemical failure: 0.2 ng/ml PSA; ND Recursive partitioning, Kaplan-Meier, and multivariate Cox regression Linson et al, 2002 [32] Biochemical failure: 2 consecutive levels >1.0 ng/ml; ND Univariate and multivariate Cox regression Nelson et al, 2002 [34] Biochemical failure: PSA >0.2 ng/ml; 71 (12%) Cox regression Nelson et al, 2003 [33] Biochemical failure: PSA >0.2 ng/ml; 183 (13%) Multivariate CPHM Maximum percentage of cancer (<50% or 50%) independent predictor of PSA failure; PSA, Gleason score, and number of positive cores not significant Both cancer volume measures significant predictors of PSA recurrence in univariate analysis; only percent of positive cores significant in multivariate analysis ( p = 0.03) PSA, Gleason, and greatest percent cancer highly predictive of PSA recurrence ( p = 0.0001), number of positive cores not significant GPC significant predictor of PSA recurrence-free survival with natural log PSA and biopsy Gleason score; number of positive cores not significant GPC significant predictor of clinical recurrence or metastasis independent of Gleason score ( p = 0.0065) Clinical recurrence or metastasis; 26 (1.8%) Potters et al, 2002 [35] Biochemical failure: 3 rises, not necessarily consecutive; 88 (8%) Principal components analysis and Somers D rank correlation Ravery et al, 2000 [36] Biochemical failure: PSA >0.5 ng/ml before September 1991: then PSA >0.1 ng/ml; ND Biochemical failure: PSA 0.4 ng/ml or local recurrence or systemic progression; 73 (16%) Kaplan Meier CPHM Sebo et al, 2002 [37] Kaplan-Meier Significant in univariate analysis: mean percent cancer in an involved core, percent cancer at apex and midgland, maximum percent at base; percent positive cores not significant Percent core length invaded by cancer and PSA density significantly predict biological progression, percent positive cores not significant Both percent positive cores (RR 1.02, 95% CI, 1.01–1.03) and surface area (RR 1.03, 95% CI, 1.02–1.04) significant predictors of cancer progression on univariate analysis ( p < 0.001) Hazard ratio (95% CI), p value 1.64 (1.25–2.15) compared with: Gleason score 1.62 (1.28–2.05) PSA 1.51 (1.17–1.97) (all p 0.001) 1.02 (1.01–1.03), p = 0.008 ND ND 1.449 (1.025–2.049), p = 0.0357 compared to: Gleason score 7–2.29 (1.60–3.27), score 8–3.17 (1.79–5.61) PSA 2.67 (2.15–3.32), all p < 0.0001 ND Log-rank test 30.1 Compared with PSA density 35.5, both p = 0.0001 Not included in multivariate analysis CI, confidence interval; pCA, prostate cancer; PHM, Proportional Hazards Model; PSA, prostate-specific antigen; ND, no data; CPHM, Cox Proportional Hazard Model; GPC, greatest percentage of cancer; RR, relative risk. was significantly associated with clinical recurrence or metastases independently of Gleason score. As reported by Gretzer and associates [31], the greatest percentage of cancer was also predictive of recurrence in a subgroup of patients with T1c pCA after radical prostatectomy. Using a PSA cut-off of 10 ng/ml and a biopsy Gleason sum of 7, two groups were defined with biochemical recurrence-free probabilities at 10 yr of 96% (95% CI, 94–98%, group T1cI) and 73% (95% CI, 62–81%, group T1cII; p = 0.0001). The first group was not investigated further because biopsy data were unlikely to improve prognostication; in the second group, the 5- and 10-yr PSA recurrence-free probability was european urology 54 (2008) 728–739 significantly higher (90% and 85%, respectively) if there was <50% involvement of the length of any one core compared to >50% (75% and 56%, p = 0.03). The greatest percentage of cancer was amongst the 23 biopsy variables investigated in a paper by Potter et al [35] reporting on patients treated by brachytherapy alone (78% of patients) or with additional external beam radiation therapy (22% of patients). When taken as the maximum percentage in any core, it was not significant in univariate analysis; but if restricted to biopsies taken from the base, it was significant. 3.9. Relative value of the number of positive cores versus the greatest percentage of cancer One group found no association between the number of positive biopsies and PSA recurrence using cut-off points of one (57% of patients), two (29% of patients), or three or more positive cores (14% of patients) [34] or using cut-off points of one versus two or more positive cores (patient distribution not given) [33]. The number of positive cores was not significant in another study, although it was recognized that the fragmented nature of some of the cores and the lack of record of the total number of cores taken limited interpretation [31]. Finally, no significance for the percentage of positive cores was found in patients treated by radiotherapy [35]. Using a model including PSA, Gleason score, and clinical stage, the Somers D rank coefficient was 0.32 (0 represents no discriminating ability, 1 is perfect discrimination). Adding the percentage of positive cores to this model increased the coefficient to 0.34. However, the best predictive model using principal component analysis was where all 23 pathologic variables, ranked by significance into component groups, were included and gave a coefficient of 0.39. 3.10. Mean percentage of cancer and its significance relative to the percentage of positive cores Linson and colleagues [32] specifically examined whether the mean percentage of core length with cancer provided significantly more information than the percentage of positive cores in predicting postoperative PSA outcome and found that only the percentage of positive cores was independently predictive. This study was restricted to men with intermediate-risk pCA defined as clinical stage 2b (1992 American Joint Consensus Committee criteria), biopsy Gleason score 7, or PSA 10–20 ng/ml, and 80% of patients had 50% positive cores. The radiotherapy study [35] did not clearly define ‘‘mean percentage of cancer in an involved core,’’ 735 and no clarification could be obtained. This measure could be interpreted as representing the total amount of cancer divided by the number of positive cores rather than by the total number of cores, as in the other study [32]. It was a significant predictor of PSA outcome ( p = 0.008), whereas the percentage of positive cores was not. 3.11. Limitations on interpretation All studies were biased because of the retrospective nature of data collection and the availability of quantitative biopsy data, in particular. There were variations in the spread of clinical stages (Tables 1 and 3), the definition of PSA recurrence, the number of recorded recurrences (Table 4), and length of follow-up, which was sometimes short (Tables 1 and 3). Furthermore, biopsy strategies and the number of cores obtained varied between and within studies (Tables 1 and 3), potentially affecting the amount of carcinoma sampled in a given patient. There was little information on laboratory handling of the biopsies, but separate embedding of cores was not mentioned, and fragmentation of multiple cores embedded together would make the assessment of the number of cores involved or the maximum amount of cancer in any core less reliable. Only three groups explicitly set quality criteria. Patients were excluded if <4 [29,30] or 6 [27] biopsies were taken, or a core was not measured if it measured <10 mm [36]. Methods of measurement also varied among studies (Tables 2 and 4), further limiting comparability among studies and the possibility of performing a meta-analysis. Two groups estimated the greatest percentage of cancer in the most involved core, but one excluded intervening benign tissue [33,34], whereas the other group included it [31]. Measurement methods were not tested for reproducibility, yet data from the External Quality Assurance Scheme (EQA) in Prostatic Pathology Reporting found that individual pathologists’ measurements were spread along a range of at least 10 mm in as much as 63% of cases [38]. Statistical methods varied, including the determination of cut-off points, which can distort the significance of results. 4. Discussion This systematic review set out to determine whether measures of tumour extent could significantly improve the estimation of risk in individual patients with pCA. There is a concern about using PSA recurrence as a surrogate for progression because it 736 european urology 54 (2008) 728–739 may not equate with clinical progression or cancerspecific death. However, the two studies that reported clinical outcomes found that tumour extent was an independent predictor of clinical recurrence or metastases [33] or cancer-specific survival [28], thereby establishing proof of principle of the potential of measures of tumour extent to refine prognostication. The results of the few studies [25–27] measuring tumour extent in millimetres were inconsistent, possibly because of variations in study design and statistical analyses. The cumulative length of cancer was a significant predictor when analyzed as a continuous [26] but not as a dichotomous variable [27], whereas the converse was true for the maximum length of cancer [25]. The distribution of measurements was also variably skewed, with 43% of patients with 9 mm cancer in one study [26] falling to 21% in the other [27]. Given the other limitations on interpretation already described, no firm conclusions can be reached regarding the value of providing measurements as absolute figures. By contrast, the studies that expressed tumour extent as a percentage were much more consistent, whether using the overall percentage of cancer in the biopsy tissue [28–30,36,37], the greatest percentage in any one core [31,33,34], or other measures [32,35]. Univariate analyses may be of limited relevance given the established value of clinical factors such as presenting PSA, but all except one [32] of the multivariate models [29–33,36], found that the percentage of cancer was independently predictive of PSA recurrence. The dissenting paper reported the average percentage of cancer, which may therefore not be as predictive as the greatest or the total percentage of cancer. The percentage of positive cores is an established predictor of PSA recurrence following radical prostatectomy [11–20], although a large study by Briganti et al [39] found that the number rather than the percentage of positive biopsies may be more informative. However, these measures may not be the best indicators of tumour burden [13]. Eleven of the 13 studies reviewed here included comparative data on the number or percentage of positive cores and the linear extent of cancer. In two, number [27] or percentage [32] was the independent predictor of PSA outcome, whereas the linear or surface area of cancer was not; in a further two, both parameters were significant—at least in univariate analysis [25,37]. However, number or percentage was not a significant factor in the other reports [26,29,31,33–36]. Possibly, the spread of values was too skewed detect differences. In the few papers with precise information in this regard [26,27,34], at least two-thirds of patients had only one or two positive cores. Furthermore, the issue of fragmentation was not specifically addressed, so that one fragmented core with three separate foci of cancer may have been recorded as one or three cores depending on the interpretation of different pathologists. Nevertheless, the weight of current evidence suggests that the linear percentage of cancer on biopsy may be more valuable in predicting PSA recurrence compared to the number or percentage of positive cores alone. The issue, therefore, is which method should be adopted in clinical practice, although demonstration of the limits of reproducibility—a requirement for any clinical test—could be a problem [38]. There is no evidence to support the independent value of the mean percentage of cancer [32,35], but there are consistent data to support the use of either the total percentage of cancer [28–30,36,37] or the greatest percentage of cancer in any one core [31,33,34]. A limited number of studies provided hazard ratios in a multivariate setting [29–31,33]. The method producing the highest reported hazard ratio (8.25) was the measurement of the total percentage of cancer analyzed as a continuous variable [29], which also appeared to have a superior predictive power compared with preoperative serum PSA levels or biopsy Gleason score. However, models using cut-off points for risk stratification rather than continuous variable are easier to adapt to clinical practice, and this was the approach subsequently taken [30]. Hazard ratios were then broadly similar [30] to those reported in papers using the greatest percentage of cancer [31,33] (Table 5). The hazard ratio was higher in the study in which intervening benign tissue was excluded from the measurement of cancer [33] compared to the method including intervening benign stroma [31], but the use of different cut-off points could account for some of this difference. The greatest percentage may underestimate tumour burden if several cores are involved. There are also theoretical advantages to using the total percentage of cancer, as the issue of fragmentation is not critical. Identification of individual cores is required for the assessment of the greatest percentage of cancer, but processing and sectioning individual cores separately has resource implications. However, fragmentation can be reduced by careful handling; individual cores can be separated between foam pads or other devices, and flat embedding can ensure that each core is fully represented. The disadvantage of measuring the overall amount of cancer is that the result will be european urology 54 (2008) 728–739 more strongly influenced by the amount of tissue sampled. In addition to the number of cores, which can vary quite widely (Tables 1 and 3), the needle direction is important, as shown by a recent systematic review of the effect of taking additional biopsies: Laterally directed cores increased the yield of pCA significantly ( p = 0.003), whereas centrally directed cores did not [40]. Additional negative cores will reduce the total percentage of cancer measurement, which may then underestimate large tumours—particularly if unilateral. This limitation might be overcome by measuring the total cancer percentage on the most involved side rather than overall, in the same way that the percentage of positive cores on the dominant side had stronger independent predictive value than the total percentage [41]. 5. Conclusions Until there is better evidence, reporting both the total and greatest percentage of cancer may identify patients who are definitely at low risk of progression if they satisfy the criteria established by both predictive models [30,33]. Reporting the number of positive cores may provide additional information [39] and is recommended in the European Association of Urology (EAU) guidelines on pCA [17]. These different measurement methods are currently being tested within the prostatic biopsy EQA scheme developed in the United Kingdom. Cumulatively, the studies reviewed have included >7000 patients, but conclusions are limited by the retrospective nature of the studies, the variations in patient characteristics, and the lack of standardized methodology. All have used the traditional method of investigating pathological prognostic factors, which is to identify all patients within an institution or database, select those who have been treated in a specific way, and then perform the analysis on the data available. These observational studies are valuable for generating hypotheses but not for producing definitive answers [42], as has been documented in previous systematic reviews of pathological prognostic factors [23,24,43]. Quality criteria have been established for the investigation of molecular markers [44], but equal rigor should be applied to the more traditional pathological factors. A well-designed prospective trial using current best-practice biopsy protocols [45], well-defined measurement methods, and standardized outcome reporting is the only way to determine the true significance of biopsy quantitative data and how these data should be used to 737 advise patients on the most appropriate management option. Author contributions: Patricia Harnden had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Coles, Harnden, Mason, Naylor, Shelley. Acquisition of data: Coles, Harnden, Naylor, Shelley. Analysis and interpretation of data: Harnden, Naylor, Shelley. Drafting of the manuscript: Harnden, Naylor, Shelley. Critical revision of the manuscript for important intellectual content: Coles, Harnden, Mason, Naylor, Shelley. Statistical analysis: None. Obtaining funding: Coles, Harnden, Mason, Shelley. Administrative, technical, or material support: Coles, Harnden, Mason, Naylor, Shelley. Supervision: None. Other (specify): None. Financial disclosures: I certify that all conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the manuscript (eg, employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending), are the following: None. Funding/Support and role of the sponsor: Cancer Research UK and Cancer Research Wales for collection and management of the data. Acknowledgment statement: This work was initiated for the revision of the guidance on reporting of urological cancers for the Royal College of Pathologists, United Kingdom. Cancer Research Wales contributed to library facilities and Cancer Research UK to salary costs (PH). We are grateful to D Berney, AV D’Amico, JI Epstein, SJ Freedland, CP Nelson, A Renshaw, V Ravery, and TJ Sebo for their prompt and helpful clarifications of measurement methodology. References [1] Burnett AL, Aus G, Canby-Hagino ED, et al. Erectile function outcome reporting after clinically localized prostate cancer treatment. J Urol 2007;178:597–601. [2] Dubbelman YD, Dohle GR, Schröder FH. Sexual function before and after radical retropubic prostatectomy: a systematic review of prognostic indicators for a successful outcome. Eur Urol 2006;50:711–20. [3] Gambacorta MA, Manfrida S, D’Agostino G, et al. Impact of dose and volume on rectal tolerance. Rays 2005;30: 181–7. [4] Stone NN, Stock RG. Complications following permanent prostate brachytherapy. Eur Urol 2002;41:427–33. [5] Klotz LH. Active surveillance for good risk prostate cancer: rationale, method, and results. Can J Urol 2005; 12(Suppl 2):21–4. 738 european urology 54 (2008) 728–739 [6] Kattan MW, Eastham JA, Stapleton AM, Wheeler TM, Scardino PT. A preoperative nomogram for disease recurrence following radical prostatectomy for prostate cancer. J Natl Cancer Inst 1998;90:766–71. [7] Kattan MW, Zelefsky MJ, Kupelian PA, et al. Pretreatment nomogram that predicts 5-year probability of metastasis following three-dimensional conformal radiation therapy for localized prostate cancer. J Clin Oncol 2003;21:4568–71. [8] Kattan MW, Zelefsky MJ, Kupelian PA, Scardino PT, Fuks Z, Leibel SA. Pretreatment nomogram for predicting the outcome of three-dimensional conformal radiotherapy in prostate cancer. J Clin Oncol 2000;18:3352–9. [9] Makarov DV, Trock BJ, Humphreys EB, et al. Updated nomogram to predict pathologic stage of prostate cancer given prostate-specific antigen level, clinical stage, and biopsy Gleason score (Partin tables) based on cases from 2000 to 2005. Urology 2007;69:1095–101. [10] Partin AW, Kattan MW, Subong EN, et al. Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer. A multi-institutional update. JAMA 1997;277: 1445–51. [11] Antunes AA, Srougi M, Dall’Oglio MF, Crippa A, Campagnari JC, Leite KR. The percentage of positive biopsy cores as a predictor of disease recurrence in patients with prostate cancer treated with radical prostatectomy. BJU Int 2005;96:1258–63. [12] Fröhner M. Editorial comment on: Chun FK-H, Karakiewicz PI, Briganti A, et al. Prostate cancer nomograms: an update. Eur Urol 2006;50:914–26. [13] Cooperberg MR, Pasta DJ, Elkin EP, et al. The University of California, San Francisco Cancer of the Prostate Risk Assessment score: a straightforward and reliable preoperative predictor of disease recurrence after radical prostatectomy. J Urol 2005;173:1938–42. [14] Crippa A, Srougi M, Dall’Oglio MF, et al. A new nomogram to predict pathologic outcome following radical prostatectomy. Int Braz J Urol 2006;32:155–64. [15] D’Amico AV, Whittington R, Malkowicz SB, et al. Combination of the preoperative PSA level, biopsy Gleason score, percentage of positive biopsies, and MRI T-stage to predict early PSA failure in men with clinically localized prostate cancer. Urology 2000;55:572–7. [16] Gancarczyk KJ, Wu H, McLeod DG, et al. Using the percentage of biopsy cores positive for cancer, pretreatment PSA, and highest biopsy Gleason sum to predict pathologic stage after radical prostatectomy: The center for prostate disease research nomograms. Urology 2003;61:589–95. [17] Heidenreich A, Aus G, Bolla M, et al. EAU guidelines on prostate cancer. Eur Urol 2008;53:68–80. [18] San Francisco IF, Regan MM, Olumi AF, DeWolf WC. Percent of cores positive for cancer is a better preoperative predictor of cancer recurrence after radical prostatectomy than prostate specific antigen. J Urol 2004;171:1492–9. [19] Cooperberg MR, Freedland SJ, Pasta DJ, et al. Multiinstitutional validation of the UCSF cancer of the prostate risk assessment for prediction of recurrence after radical prostatectomy. Cancer 2006;107:2384–91. [20] May M, Knoll N, Siegsmund M, et al. Validity of the CAPRA score to predict biochemical recurrence-free survival after radical prostatectomy. Results from a European multicenter survey of 1,296 patients. J Urol 2007; 1957–62. [21] Egevad L, Allsbrook Jr WC, Epstein JI. Current practice of diagnosis and reporting of prostate cancer on needle biopsy among genitourinary pathologists. Hum Pathol 2006;37:292–7. [22] Parsons JK, Partin AW. Clinical interpretation of prostate biopsy reports. Urology 2006;67:452–7. [23] Harnden P, Shelley MD, Clements H, et al. The prognostic significance of perineural invasion in prostatic cancer biopsies: a systematic review. Cancer 2007;109:13–24. [24] Harnden P, Naylor B, Shelley MD, Clements H, Coles B, Mason MD. The clinical management of patients with a small volume of prostatic cancer on biopsy: what are the risks of progression? A systematic review and meta-analysis. Cancer 2008;112:971–81. [25] Egawa S, Suyama K, Arai Y, et al. Treatment outcome by risk group after radical prostatectomy in Japanese men. Int J Urol 2001;8:295–300. [26] King CR, Patel DA, Terris MK. Prostate biopsy volume indices do not predict for significant Gleason upgrading. Am J Clin Oncol 2005;28:125–9. [27] Noguchi M, Stamey TA, McNeal JE, Nolley R. Prognostic factors for multifocal prostate cancer in radical prostatectomy specimens: lack of significance of secondary cancers. J Urol 2003;170:459–63. [28] Cuzick J, Fisher G, Kattan MW, et al. Long-term outcome among men with conservatively treated localised prostate cancer. Br J Cancer 2006;95:1186–94. [29] Freedland SJ, Aronson WJ, Csathy GS, et al. Comparison of percentage of total prostate needle biopsy tissue with cancer to percentage of cores with cancer for predicting PSA recurrence after radical prostatectomy: results from the SEARCH database. Urology 2003;61:742–7. [30] Freedland SJ, Terris MK, Csathy GS, et al. Preoperative model for predicting prostate specific antigen recurrence after radical prostatectomy using percent of biopsy tissue with cancer, biopsy Gleason grade and serum prostate specific antigen. J Urol 2004;171:2215–20. [31] Gretzer MB, Epstein JI, Pound CR, Walsh PC, Partin AW. Substratification of stage T1C prostate cancer based on the probability of biochemical recurrence. Urology 2002;60:1034–9. [32] Linson PW, Lee AK, Doytchinova T, et al. Percentage of core lengths involved with prostate cancer: does it add to the percentage of positive prostate biopsies in predicting postoperative prostate-specific antigen outcome for men with intermediate-risk prostate cancer? Urology 2002;59: 704–8. [33] Nelson CP, Dunn RL, Wei JT, Rubin MA, Montie JE, Sanda MG. Contemporary preoperative parameters predict cancer-free survival after radical prostatectomy: a tool to facilitate treatment decisions. Sem Urol Oncol 2003;21: 213–8. [34] Nelson CP, Rubin MA, Strawderman M, Montie JE, Sanda MG. Preoperative parameters for predicting early prostate european urology 54 (2008) 728–739 [35] [36] [37] [38] [39] cancer recurrence after radical prostatectomy. Urology 2002;59:740–6. Potters L, Purrazzella R, Brustein S, Fearn P, Leibel SA, Kattan MW. A comprehensive and novel predictive modeling technique using detailed pathology factors in men with localized prostate carcinoma. Cancer 2002;95:1451–6. Ravery V, Chastang C, Toublanc M, Boccon-Gibod L, Delmas V. Percentage of cancer on biopsy cores accurately predicts extracapsular extension and biochemical relapse after radical prostatectomy for T1-T2 prostate cancer. Eur Urol 2000;37:449–55. Sebo TJ, Cheville JC, Riehle DL, et al. Perineural invasion and MIB-1 positivity in addition to Gleason score are significant preoperative predictors of progression after radical retropubic prostatectomy for prostate cancer. Am J Surg Pathol 2002;26:431–9. Harnden P, Coleman D, Moss S, Kodikara S, Patnick J, Melia J. Prostatic pathology reporting in the UK: development of a national external quality assurance scheme. Histopathology 2008;52:147–57. Briganti A, Chun FK-H, Hutterer GC, et al. Systematic assessment of the ability of the number and percentage of positive biopsy cores to predict pathologic stage and biochemical recurrence after radical prostatectomy. Eur Urol 2007;52:733–45. 739 [40] Eichler K, Hempel S, Wilby J, Myers L, Bachmann LM, Kleijnen J. Diagnostic value of systematic biopsy methods in the investigation of prostate cancer: a systematic review. J Urol 2006;175:1605–12. [41] Freedland SJ, Aronson WJ, Terris MK, et al. The percentage of prostate needle biopsy cores with carcinoma from the more involved side of the biopsy as a predictor of prostate specific antigen recurrence after radical prostatectomy: results from the Shared Equal Access Regional Cancer Hospital (SEARCH) database. Cancer 2003;98:2344–50. [42] Moore A, McQuay H. Making sense of the medical evidence. Oxford, United Kingdom: Oxford University Press; 2006. [43] Harnden P, Shelley MD, Coles B, Staffurth J, Mason MD. Should the Gleason grading system for prostate cancer be modified to account for high-grade tertiary components? A systematic review and meta-analysis. Lancet Oncol 2007;8:411–9. [44] McShane LM, Altman DG, Sauerbrei W, Taube SE, Gion M, Clark GM. Reporting recommendations for tumor MARKer prognostic studies (REMARK). Nat Clin Pract Urol 2005;2:416–22. [45] Scattoni V, Zlotta A, Montironi R, Schulman C, Rigatti P, Montorsi F. Extended and saturation prostatic biopsy in the diagnosis and characterisation of prostate cancer: a critical analysis of the literature. Eur Urol 2007;52:1309–22.