Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
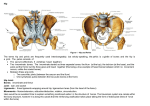
New Hampshire Musculoskeletal Institute 17th Annual Symposium, 2010 Michael J. Mullin, ATC, LAT, PTA OA Centers for Orthopaedics Physical Therapy Center Portland, Maine www.orthoassociates.com [email protected] Thank you Jim, Laura and NHMI. . . • Most PF conditions and general diffuse joint pain • Most knee –itis’ • Many foot/ankle chronic conditions such as plantar fasciitis, Achilles tendinitis, posterior tibialis tendinoses • Many acute injuries, especially noncontact, such as ACL, MCL injured or post‐op ACL surgery • Many meniscal pathologies, including post‐op • Pertinent joint anatomy, physiology and arthrokinematics. • Structural asymmetry • Examination techniques and considerations Anatomy Osseous structures Femur MFC/LFC Tibia Lateral plateau‐‐convex Medial plateau‐‐concave 50% larger than lateral Fibula Patella facets Anatomy Meniscus Lateral Larger than medial More fully circular Consistent in width Greater mobility than medial Medial C‐shaped and broader posteriorly than anteriorly Attached to deep medial capsule Anatomy Primary ligaments—varying tension measures on different portions depending on joint position ACL PCL LCL—thin and round Popliteus runs underneath MCL—broad and flat Superficial & deep fibers Deep fibers attach to medial meniscus Anatomy Capsular and supporting structures Medial structures— viewed as 3 layers Superficial / Layer I Middle / Layer II Fascia, sartorius, medial patellar retinaculum, fascial fibers of VMO, medial head gastroc Some distal insertions of semitendinosis and gracilis near pes anserinus MCL/superficial fibers Deep / Layer III Considered true capsule MCL/deep fibers, semimembranosus Provides rotational support to MFC Anatomy Capsular and supporting structures Lateral structures— divided into 3 layers Superficial / Layer I Intermediate / Layer II Prepatellar bursa, ITB, biceps femoris (LH/SH) tendons LCL, lateral patella retinaculum Capsule / Layer III Deep ligaments (arcuate, fabellafibular), capsule, popliteus often pierces deep capsule Anatomy‐‐other structures Posterior capsule and stabilizing ligaments and muscles Bursa, infrapatellar fat pad, plica, fascia Anatomy Muscular influences • No two human structures are the same • Each with our own set of compensations due to. . . • Asymmetries exist all over the body • These produce strong biases in terms of movement • There are commonly identified deficiencies side‐to‐side • They are positionally dependent • Muscles and tendons take on different roles: • depending on the joint(s) position of the bones that it influences • when changing their role from mover ↔ stabilizer • Most motor functions of the muscles can be altered in the presence of: pain, swelling, tissue damage, spasticity, trigger points, mechanical forces, and structural / functional malalignment Musculoskeletal structures Knee extensors Rectus femoris Also flexes hip Vastus intermedius Vastus lateralis Vastus medialis Patella tendon/ligament Articularis genus Iliotibial tract In ranges between 0‐30 degrees Musculoskeletal structures Knee flexors Biceps femoris Also extends hip Posterior ilium positioner (especially long head) Semimembranosus Also primary hip extensor Knee medial rotator Semitendinosis Also hip extensor Posterior ilium positioner Knee medial rotator Gastrocnemius Also primary ankle plantarflexor Iliotibial tract In ranges greater than 40 degrees Musculoskeletal structures Muscles influencing knee rotation Also function as stabilizers Popliteus Medial/ IR Also unlocks knee from terminal extension Medial hamstrings Medial / IR Biceps femoris Lateral/ER ITB/TFL • Poor muscle control in pelvis, hip and ‘core’ produces deleterious loads onto the knee and lower extremity. • Mechanical hip and pelvis malpositioning with movement produces altered loads distally. • Decreased trunk control allows momentum to carry the body past the point the pelvis and lower extremity can stabilize effectively. Proximal musculoskeletal influences •Adductors •Adductor group •Gracilis •Abductors •Glute med/min •Sartorius •Obturator internus •Medial rotators •Glute med/min •TFL •Pectineus •Lateral rotators •Glute max •Piriformis •Obturators •Gemellus •Iliopsoas Proximal musculoskeletal influences What does this position. . . . . . do to these muscles? Proximal musculoskeletal influences As clinicians we need to decide what we feel is proper alignment and base our treatments on these approaches What is considered “neutral”? Neutral spine, pelvis and/or hips What role do the ribs and thorax have on the pelvis, hips and LE Should we be calling something that is dynamic “posture”? Proximal musculoskeletal influences What do the glute muscles do? What position are the glute muscles in? Proximal musculoskeletal influences Important to recognize that there are two distinct types of movements in the hips and pelvis: The femur moving in the acetabulum (FA) The acetabulum moving on the femur (AF) Muscles function with very specific tasks as stabilizers > movers Muscles have proximal and distal attachments vs. an origin and insertion They pull from both attachments with different resultant movements It is important to remember that the actions of most muscles changes based on alterations in joint position proximally and/or distally. One example is the gluteus med/min externally rotate the thigh when the hip is flexed but internally rotate the thigh with the hip extended. Another example is the role of the hamstrings as medial rotators of the tibia. Their effectiveness increases as the knee increases flexion closer to 90 degrees. Proximal musculoskeletal influences What about pelvic obliquities? . . .or scoliosis? Proximal musculoskeletal influences Most people function with some degree of pelvic obliquity along with its associated compensation Need to think rotation Every movement of every joint in the body has rotation The ability to control excessive rotation and timing in both a concentric and eccentric fashion is integral for optimal movement Tri‐planar motion needs to be considered when analyzing joint motion and positioning Need to think outside the circle Proximal musculoskeletal influences Does this. . . . . .lead to this? Proximal musculoskeletal influences Previous history of repetitious positional strain (ADL’s) will likely produce chronic or permanent change with poor adaptation patterns Lengthening and shortening of tissue Impingement, contractures and laxity of joint structures Deep muscular control of stabilizers and pelvic floor are closely linked with multiple other systems (i.e. respiratory) Educating athletes on awareness with ADL’s is imperative to reinforce good mechanics Sitting and standing positions Ambulation patterns Leaning Locked joints Proximal musculoskeletal influences Do ADL patterns influence. . . . . .these types of mechanics? Proximal musculoskeletal influences Imperative to recognize the role that every muscle plays in: Stabilization Both concentrically and eccentrically Rotation Joint and structural repositioning What is holding the center? Neutrality is the goal Proximal musculoskeletal influences Important to consider position of the bones and joints and subsequently the muscles affected in order to effectively train for use Are the muscles in a short or long position as a result? What types of altered forces will this produce? Structure dictates function Position dictates function Proximal musculoskeletal influences • Proper positioning of the hip and pelvis in a symmetrical pattern with no compensatory patterns further reduces strain onto knee. Most people fall into patterns of dysfunction in femoralacetabular (FA) and acetabulofemoral (AF) movement due to improper muscle sequencing. • SELF EVALUATION • Knee joint biomechanics directly influenced by proximal and distal joint position. • Joint movement also influenced by elastic energy, which is the stored energy of connective tissue when stretched. This stored energy is used to help return the joint to its original position when the stresses are removed. • Subtle variances in arthrokinematic movement can be palpated and influenced in NWB and PWB positions. Passive joint stiffness can be evaluated in static and passive movements. There is more excursion and general rotation in the lateral compartment vs. medial during movement in the sagital and transverse planes. If joint surfaces do not glide normally throughout the range of motion, then stretching of the passive stabilizers, increased tone of the movers and increased compressive forces onto the cartilage all takes place. Normal, passive arthrokinematics needs to be established before active can be achieved. Biomechanics •Pronation/supination influence • Proximal and distal bony alignment • Proximal femur positioning and control • Altered arthrokinematic TF movement—positional faults • Environmental (i.e. playing surface), level of activity, body awareness, holding an object • ADL patterns Forces affecting TF rotation •Pronation/supination: • As the foot goes from supination at heel strike to pronation, and the tibia goes from positionally oriented ER to IR, a lot of that motion is due to momentum. • Some of it is active IR, but medial knee muscular and capsular tissue needs to stabilize and decelerate; proximal and distal femur musculature needs to control excessive movement. • Capsular structures take on a role of acting like “check reins” to reduce further movement. •This produces thickening of surrounding soft tissue producing a change in the resting length of tissues. Forces affecting TF rotation What position are the toes in? What does this do to the trunk? Forces affecting TF rotation Important to note direction of pull Forces affecting TF rotation • Proximal and distal bony alignment Hip retroversion or anteversion • Pelvic width/Q‐angle • Hip or pelvis malalignments • Tibial varum/valgum • Foot and ankle forefoot and rearfoot NWB and WB positions • • Only the foot and ankle alignment has been shown to be effectively altered conservatively (i.e. shoes, orthotics). Forces affecting TF rotation • Proximal femur control Important to have the ability of hip and pelvis stabilizers to allow for proper femoral‐acetabular (FA) and acetabular ‐femoral (AF) control. • Pelvis and thorax need to be in neutral positions before LE can be optimally stabilized. • Restricted or excessive mobility in the femoral‐acetabular joint will ultimately affect distal mechanics. • • More likely to see left posterior hip restrictions in capsular mobility with decreased hip and pelvis IR . Forces affecting TF rotation Proximal femur control “Subjects with greater gluteus maximus activity had a lower time to decelerate the tibia. We suggest that a high level of gluteus maximus activity results in a larger external torque being applied to the femur, which ultimately leads to a more rapid deceleration of the tibia.” (“The influence of gluteus maximus on transverse plane tibial rotation”, 27:4, Gait & Posture, 2008) Forces affecting TF rotation • Altered arthrokinematic TF movement Soft tissue tone and restrictions • Decreased meniscal mobility • Edema and/or joint inflammation • Guarding • Injury induced and post‐ injury patterns • • Post‐surgical considerations such as ACL graft choice influencing muscle recovery Forces affecting TF rotation Environmental considerations Forces affecting TF rotation Environmental considerations Sport‐dependent variations in arm position during single‐limb landing influence knee loading: implications for anterior cruciate ligament injury. Chaudhari AM, Hearn BK, Andriacchi TP. Am J Sports Med. 2005 Jun;33(6):824‐30. •Other considerations • “Joint laxity, stiffness, and energy loss were compared between male and female subjects. Women had higher laxity, lower stiffness, and higher energy loss in external tibial rotation than did men.” • • Gender differences in passive knee biomechanical properties in tibial rotation, Journ of Ortho Research, 26:7, 2008. “Even when researchers looked at non‐contact ACL injuries only, about half happened on the dominant leg, and half on the supporting leg. However, when they broken down by gender, the numbers changed drastically. Injuries on the dominant leg occurred in 74% of males, but only 32.3% of females.” • ACL injuries could be influenced by gender and which leg dominates, study finds. LA Times, August 2, 2010. • Pertinent joint anatomy, physiology and arthrokinematics. • Structural asymmetry • Examination techniques and considerations Structural asymmetry sym∙me∙try (sm‐tr) n. pl. sym∙me∙tries Exact correspondence of form and constituent configuration on opposite sides of a dividing line or plane or about a center or an axis. Beauty as a result of balance or harmonious arrangement Structural asymmetry What is asymmetry? The human body is not symmetrical. The neurological, respiratory, circulatory, muscular and vision systems are not the same on the left side of the body as they are on the right, and vice versa. They have different responsibilities, function, position and demands on them. This system asymmetry is a good thing and an amazing design. The human body is balanced through the integration of system imbalances. Postural Restoration InstituteTM Structural asymmetry Left vs. right brain‐‐controls opposite side Right Brain Left Brain Random Intuitive Holistic Synthesizing Subjective Looks at wholes Logical Sequential Rational Analytical Objective Looks at parts Because the left brain has more responsibilities for speech and language, the right upper extremity becomes a dominant extremity in communication, growth and development. Structural asymmetry Organ asymmetry Liver on the right, not on left Right diaphragm is more superiorly orientated than the left and supported by the liver Increased advantage producing a stronger respiratory muscle pull Left diaphragm leaflet is much smaller and does not have the advantage to pull the ribs up and out upon inhalation (relaxes left abdominal wall) Cardiac muscle more on left side than right Three lobes in the right lung, two on the left Vagal nerve is often more posteriorly and superiorly oriented on the right during development Structural asymmetry Respiratory asymmetry Structural asymmetry Polyarticular chains ANTERIOR INTERIOR CHAIN (AIC) Muscles: Diaphragm, Iliacus, Psoas, TFL, Vastus Lateralis, Biceps Femoris There are two anterior interior polyarticular muscular chains in the body that have a significant influence on respiration, rotation of the trunk, ribcage, spine and lower extremities. They are composed of muscles that attach to the costal cartilage and bone of rib 7 through twelve to the lateral patella, head of the fibula and lateral condyle of the tibia. These two tracts of muscles, one on the left side of the interior thoraco‐ abdominal‐pelvic cavity and one on the right, are composed of the diaphragm and the psoas muscle. With the iliacus, tensor fasciae latae, biceps femoris and vastus lateralis muscles this chain provides the support and anchor for abdominal counter force, trunk rotation and flexion movement. Postural Restoration InstituteTM Structural asymmetry Polyarticular chains The pattern that is most often prevalent involves the left anterior interior chain. The left pelvis is anteriorly tipped and forwardly rotated. This directional, rotational influence on the low back and spine to the right, mandates compulsive compensatory movement in one or more areas of the trunk, upper extremities and cervical‐ cranial‐mandibular muscle. The greatest impact is on rib alignment and position, therefore influencing breathing patterns and ability. It is very possible that respiratory dysfunctions, associated for example with asthma or daily, occupational, repetitive, work positions, can also influence pelvic balance and lead to a compensatory pattern of an anteriorly tipped and forwardly rotated pelvis on the left. Postural Restoration InstituteTM Structural asymmetry Common compensatory presentation Structural asymmetry Common compensatory presentation What does this produce? Right foot supination Tibial rotation restrictions Overactive right hamstrings, femoral adductors, IR’s and internal obliques All underactive on the left Poor control of left hemi‐pelvis Decreased ability to extend and adduct the left femur Lumbar right rotation bias with probable correction into thoracic spine with increased left rotation (functional scoliosis) Varying levels of increased lumbar lordosis and thoracic extension Shoulder imbalances Cervical‐cranial‐mandibular dysfunction Structural asymmetry What does asymmetry do? Structural asymmetry What does asymmetry do? Creates a pattern of comfort to one side that can be difficult to break, especially if there are contractures as a result. Can produce joint compression and tissue shortening and lengthening and thus poor activation patterns of certain muscle groups. OA Centers for Orthopaedics review of surgical hip labral repairs for 2 year time span revealed 68% more right procedures than left. Structural asymmetry “Development of scoliosis is “Significantly greater peak valgus connected with ‘gait’ and habitual ‘standing at ease’ on the right leg” “In all children with so‐called idiopathic scoliosis limited adduction of the right hip was found, or even abduction contracture of this hip, often connected with flexion and external rotation contracture.” torque during spin turn was found than that during step turn for the left leg, while there was no significant difference between 2 turn strategies for the right leg. The study indicated that, for right dominant people, turning with right leg or using step turn might reduce the stress on the ACL or ACL graft after reconstruction” (Biomechanical aetiology of the so‐ called idiopathic scoliosis: New clinical and radiological classification. Karski, TK, 2010). (Knee Rotation and Loading during Spin and Step Turn. Wang H, Zheng N, Int J Sports Med, 2010) Structural asymmetry What can be done? Recognize that there are differences side‐to‐side and understanding facilitation and inhibition principles can dramatically improve your outcomes. When treating a condition on one side of the body, there is likely something on the other side‐‐and likely something different‐‐ contributing to the problem as well. When introducing any corrective or therapeutic exercise, try and incorporate some activity on the opposite side and integrate upper body involvement as soon as able to demonstrate proficiency of earlier phases Structural asymmetry What can be done? When treating patients/athletes, consider: Make sure neutrality has been achieved prior to engaging in therapeutic exercise program Reduce the amount of extension and lordosis by better core positioning They all should do left hip adductor and IR exercises in a left posterior shifted position Have them work the right glute max in a left posterior shifted position Try to incorporate a little left thoracic sidebend with flexion as able Equal reciprocal arm swing should be addressed when teaching gait and exercises Most patients will benefit from stretching of the left posterior hip and right anterior hip Contemplating? Questions? • Pertinent joint anatomy, physiology and arthrokinematics. • Structural asymmetry • Examination techniques and considerations • Visual • Palpation • Passive/manual motion assessment • Other contributing factors • Evaluation considerations Examination of TF rotational dysfunction •Visual—standing posture • Bi‐ or unilateral femoral IR/”squinting patella” • “Corkscrew” leg→ • Often asymmetric foot stance with one leg more horizontally abducted (often more R out toe) • Increased pronated or supinated foot posture and often not the same on each side • Anterior pelvic tilt (often more on L side) and/or increased lumbar lordosis • Shoulder height differences Examination of TF rotational dysfunction Examination of TF rotational dysfunction Ambulation Increased apparent rotation more in the transverse plane throughout the lower kinetic chain Heel‐whip at toe‐off and swing phase of gait Poor ability to control pronation or to resupinate, especially barefoot Lateral shifting to one side more than contralateral or “Sailor’s gait” Tacking their way through life Out‐toe—”Lazy gait” vs. “Dancer’s gait” Can’t resupinate through feet if ambulating in out‐toe Decreased arm swing on one side or with arms in too much extension Arms in extension, the system is in extension Examination of TF rotational dysfunction Observing other functional movements which may be contributing to their symptoms important as well—especially tasks which are repetitive. • Visual • Palpation • Passive/manual motion assessment • Other contributing factors • Hip and pelvis evaluation considerations Examination of TF rotational dysfunction • • Palpation—common regions of tenderness and associated soft tissue restriction • Check myofascial mobility and general soft tissue mobility first • Inferior medial and/or lateral patella • Medial capsule and joint line • Pes anserinus • Medial hamstrings, especially where they pass the posteromedial tibia • Popliteus at both insertions • Proximal insertion pain often misdiagnosed as ITBFS • Medial gastroc head • Posterolateral capsule • Fibula head ant>post Move from examination to treatment fairly quickly to restore normal joint movement • Examination of TF rotational dysfunction Trigger points, soft tissue thickening or restriction, tenderness Palpation‐Inf. Med. patella Palpation‐Inf. Med. patella Examination of TF rotational dysfunction Palpation—medial capsule and joint line / assessing general soft tissue mobility as well as tender and/or thickened tissue Examination of TF rotational dysfunction Palpation—pes anserinus and medial hamstrings / assessing pes and HS mobility independent of more superficial and deeper structures Examination of TF rotational dysfunction Palpation—popliteus at tibial and femoral insertions Examination of TF rotational dysfunction • Palpation—medial gastrocnemius head, popliteus, posterior medial structures • Trigger points, tenderness, mobility • What gets tight as you move the joint into the pattern of restriction? • Visual • Palpation • Passive/manual motion assessment • Hip and pelvis evaluation considerations Examination of TF rotational dysfunction • Thorough knee exam with special tests to rule out associated pathology • Passive/manual motion assessment of knee joint • arthrokinematics Supine circumduction palpation exam Knee examination Ruling out associated pathology ER rotational laxity ‘Dial’ test at 90 and 30 deg. End‐feel and amount Observe tibial tubercle Passive/manual motion assessment Supine circumduction palpation exam One hand grasping the calcaneus while the other hand grasps joint line with thumb on lateral and forefinger (or 2‐4 pads of fingers) along medial. Thumb can be dropped to feel motion at fibula head for a few cycles as well. Starting with the hip and knee in fairly neutral positions. Begin with internally rotating tibia while bringing hip into flexion and ER. While cycling the knee through the motion, feel for the quality of movement of the tibia on the femur. Passive/manual motion assessment Supine circumduction palpation exam You should feel the medial tibial condyle drop posteriorly while the lateral condyle travels anterior and vice versa when bringing leg back into starting position. Perform a number of times to feel where restrictions seem apparent, i.e. bands of tissue getting taut under your fingers as you move the tibia. Also feeling for restrictions in femoral rotation suggestive of altered loads distally. Passive/manual motion assessment Supine circumduction palpation exam Examination of TF rotational dysfunction Other contributing factors Fibula position • Anterior talus orientation • Hip capsule restrictions • • Visual • Palpation • Passive/manual motion assessment • Hip and pelvis evaluation considerations Examination of TF rotational dysfunction Evaluation considerations Supine Sidelying Prone Seated Weightbearing Functional movements Examination of TF rotational dysfunction Evaluation considerations Supine “Set” the pelvis Visual assessment Leg length difference Most often due to asymmetry Anatomical? Helps determine symmetry Long axis hip IR/ER Helps determine pelvis anatomy and symmetry Position of pelvis (A/P, in‐outflares, dorsal/caudal) Pelvis mobility A‐P and into rotation Short axis hip IR/ER Thomas test Long leg sit up to “confirm” Long axis draw Raise and drop the hips Palpation To determine flexibility, laxity and/or pelvis position? More specific hip mobility assessment Foot and ankle mobility Talar glide 1st MTP mobility Examination of TF rotational dysfunction Evaluation considerations Sidelying Ober test ITB tightness vs. positional fault Consistency with testing Knees need to be bent 90 degrees to start Pelvis needs to be stabilized Bring leg up and back before trying to adduct If you can’t extend, don’t bother trying to adduct End‐feel assessment as well when bringing into adduction Examination of TF rotational dysfunction Evaluation considerations Prone Pillow under hips best, lie flat, face down, possible pillow under ankles Arms relaxed and lying in as neutral/straight position as possible Palpate PSIS, ischial tuberosities, sacral prominences and coccygeal orientation prior to lumbar vertebrae Sacral position and play Thoracic mobility Assess QL, erector spinae, and piriformis tone Suggestive of positional fault more than primary problem Bend knees to 90 deg/assess IR / ER Actively and passively Quality Examination of TF rotational dysfunction Evaluation considerations Seated at end of table Passive hip IR to ER ratios Certain available amount (total norm) in either direction 60° ER / 40° IR at 90/90 Can be more in one direction than the other and different on contralateral side Anything greater than the total norm, consider laxity If unequal side‐to‐side with more IR on one side and more ER on the contra, than positional fault Examination of TF rotational dysfunction Functional movements Breaking down certain movement patterns to further isolate source(s) of impairment aids in the development of a comprehensive treatment plan. Looking for compensatory movement (i.e. forward trunk position, side leaning to counterbalance, hip hiking, poor foot/ankle control) Examination of TF rotational dysfunction Functional movements Examination of TF rotational dysfunction Functional movements Functional tests Single leg balance Two‐legged squat Single leg squat Bilateral jumping Unilateral hopping Assessing deficiencies • All knee conditions, acute or chronic, should be screened for TF rotational dysfunction. • Having a solid understanding of normal joint mechanics and mobility aids in quickly identifying pathological knees. • Recognize that there will almost always be compensations due to assymetry that is likely contributing to condition. • A thorough knee examination includes: • • • • assessment of knee soft tissue and joint mobility ruling out associated pathology proximal and distal contributing factors evaluation functional movements • It is imperative that other factors which may be contributing to the pathology implemented. walking and symmetrical. are identified and a treatment plan to address these is This includes educating the patient on sitting, standing, positional postures during the day. Make their day more • Knee Ligament Rehabilitation; Ellenbecker T. Churchill‐Livingstone, New York, NY; 2000. • Basic Biomechanics of the Musculoskeletal System; Nordin M, Frankel V. Lea & Febiger, Malvern, PA; 1989. • Athletic Therapy Today, Vol. 5, No. 2, 2000. • Biomechanical aetiology of the so‐called idiopathic scoliosis (1995 – 2007). New clinical and radiological classification. Rules of new rehabilitation treatment and causal prophylactics. Prof. Tomasz Karski MD PhD , (2010) Vincent Pol University in Lublin / Poland • Knee Rotation and Loading during Spin and Step Turn. Wang H, Zheng N, Int J Sports Med, 2010. • Gender differences in passive knee biomechanical properties in tibial rotation. Hyung‐Soon Park, Nicole A. Wilson, Li‐Qun Zhang; Journal of Orthopaedic Research, 26:7, 2008. • Tibial Rotation Affects Anterior Displacement of the Knee. Martin, D.E., Guskiewicz, K.M., Perrin, D.H., Kahler, D.M., & McCue, F.C. (1994). Journal of Sport Rehabilitation, 3:275‐281. • Tibiofemoral movement 4: changes of axial tibial rotation caused by forced rotation at the weight‐bearing knee studied by RSA. J. Karrholm, S. Brandsson, M. A. R. Freeman, From Sahlgrenska University Hospital, Gothenburg, Sweden. Journal of Bone and Joint Surgery, 82:8, 2000. • The Influence of Tibial and Femoral Rotation on Patellofemoral Contact Area and Pressure, Lee TQ, Morris G, Csintalan RP. JOSPT, 33:11, 2003. • The influence of gluteus maximus on transverse plane tibial rotation, Preece SJ, et al, Gait & Posture, 27:4, 2008. • Postural Restoration Institute course notes, website and personal communication. PRI, 5241 R Street, Lincoln, NE 68504, 888‐691‐4583, www.posturalrestoration.com • www.health.com • www.pponline.co.uk www.orthogate.org www.eorthopod.com