Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
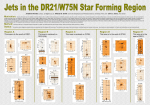
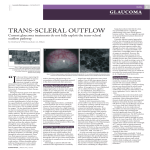
The effect of corticosteroids on aqueous humor formation rate and outflow facility W. W. Oppelt,* E. D. White, Jr., and E. S. Halpert The effect of corticosteroids on aqueous humor (AH) formation rate and outflow facility was measured in the cat eye. AH formation rate was determined by continuous posteroanterior chamber perfusion with an AH-like buffer containing inulin-C1*. It was found that the total quantity of inulin-CJi recovered through the anterior chamber outflow cannula could be used to estimate changes in outflow facility. Intravenous hydrocortisone in doses from 1 to 100 mg. per kilogram caused a dose-related decrease in AH formation rate. At the same doses and at 0.1 mg. per kilogram, there was a decrease in outflow facility averaging about 23 per cent. When various doses of hydrocortisone were perfused through the eye chambers or injected into the vitreous, there was no change in AH formation rate or outflow facility. When hydrocortisone or dexamethasone was dropped onto the cornea, there was again a slight reduction in AH formation rate and a significant decrease in outflow facility. Particularly with dexamethasone, the effect on the outflow facility seemed to predominate over the effect on AH formation rate. Data suggest that the rise in intraocular pressure reported after topical or systemic corticosteroids is mediated by a direct effect of these hormones on the outflow facility. The outflow facility appears to be more sensitive to corticosteroids than the mechanism controlling AH secretion. Key words: aqueous humor formation decrease, aqueous humor outflow facility, pharmacodynamics, hydrocortisone, dexamethasone, perfusion, intravitreal injection, intravenous injections, drug administration (topical), cats the glaucomatous eye. He found that, in comparable age groups, the dexamethasone-induced increase in intraocular pressure (IOP) was greater in the glaucomatous eye that in the normal eye. Becker and Mills3 demonstrated significant elevation of IOP after topical application of corticosteroids in glaucomatous patients and glaucoma suspects. This was interpreted as being due to a decrease in the outflow facility. In a later publication4 Becker categorized the IOP response to topical steroids into three groups, in decreasing order of response: (1) patients with open-angle glaucoma, (2) relatives of -here has been considerable interest in the effect of corticosteroids on aqueous humor (AH) dynamics. Armaly1-2 made a detailed study of the effect of topically applied dexamethasone on the normal and From the Department of Pharmacology and Therapeutics, University of Florida College of Medicine, Gainesville, Fla. 32601. Supported by a Fight-for-Sight Grant-in-Aid of the National Council to Combat Blindness, Inc., New York, N. Y., and National Institute of Health Grant GM 01764. "Burroughs Wellcome Scholar in Clinical Pharmacology. 535 Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933002/ on 05/10/2017 Investigative Ophthalmology October 1969 536 Oppelt, White, and Halpert patients with glaucoma and glaucoma suspects, and (3) normal persons. These responses were thought to be genetically determined.40 Francois and colleagues,7 however, could not confirm this theory. There have also been reports of increased IOP after systemic corticosteroid therapyS11 and after long-term topical prednisone treatment.1' It is thought that the mechanism of corticosteroid-induced ocular hypertension involves reduction of the outflow facility.1-3> 4 Nicholas,13 however, commented that the increased IOP values obtained in normal volunteers could not be completely explained by changes in outflow facility and suggested that there had to be a concomitant increase in AH formation. Armaly,1 however, reports a decrease in AH formation. Animal studies such as those of Tuovinen and co-workers14 and of Linner and Wistrand15 are, on the whole, inconclusive. We have in this study measured the effect of intravenous, intraocular, and topical corticosteroids on AH formation rates, utilizing the technique of continuous posterior-anterior chamber perfusion with an AH-like buffer containing inulin.10 Additionally, we present arguments that the perfusion technique can be used to estimate changes in the outflow facility of the eye. The effect of corticosteroids on this parameter could thus be determined. Methods Male and female cats of mixed breed, weighing from 2 to 4 kilograms, were anesthetized with single intrahepatic injections of 30 mg. per kilogram of pentobarbital. Continuous perfusion from the posterior to the anterior chamber of the eye with an AH-like buffer containing inulin-C14 was then begun, as previously described.10 After an initial equilibration period, to insure adequate mixing, perfusion was maintained at a steady rate and samples were collected in 30 minute periods. Radioactivity due to inulin-C14 was determined in inflow and outflow samples and AH formation rates were calculated, with the use of the rate of inflow and the degree of dilution of the inulinC14.16 The total amount of inulin recovered in each 30 minute period was also measured and compared to the total amount of inulin infused. Protein concentrations were determined in each outflow sample, as previously described,10 and experiments in which the protein concentrations exceeded 300 mg. per 100 ml. were discarded. The basic protocol of each experiment consisted of a 2 hour control period to establish the normal values of AH formation rates and inulin recovery, followed by a 4 hour experimental period when various doses of hydrocortisone sodium succinate were injected intravenously, added to the perfusate, given topically, or injected into the vitreous. In our system, where IOP and rate of perfusion are maintained constant, some of the infused inulin will leave the eye through the normal outflow facility and the remainder will exit through the outflow cannula. It is reasoned that the total amount of inulin exiting through the outflow cannula during each time period is a function of the resistance of the outflow facility. As long as the pressure of the system is held constant, it can be assumed that any change in the total amount of inulin collected must therefore indicate some change in the resistance of the outflow fa- Table I' AH formation (nl/min.) No. of experiments Drug dose First 2 hr. Inulin recovery (per cent infused inulin) Average per Average per Last 4 hr. cent change\ First 2 hr. Last 4 hr. cent change\ 13.710.5 +11.3 ±4.7 68.9 ±2.3 68.6 ± 1.4 +1.8 ±2.9 No drug 12.7 ±0.6t 30 °No drug was administered in these experiments. AH formation rates and inulin recovery during the initial 2 hours of the experiment were compared to the values for the final 4 hours. AH formation was calculated for each 30 minute period.10 These periods were then averaged to calculate control and post-drug formation rates. Inulin recovery was calculated for each 30 minute period. These periods were then averaged to calculate control and postdrug inulin recovery. Inulin recovery was calculated as follows: (Volume of outflow in ml./30 min.) x (outflow inulin-C14 counts/min./ml.) (Volume of inflow in ml./30 min.) x (inflow inulin-C14 counts/min./ml.) x 100 = per cent infused inulin recovered. An increase in inulin recovery indicates a decrease of the outflow facility, as explained in the text. It should be noted that there is no significant change in inulin recovery during the first 2 hours of the experiment, compared to the last 4 hours. | The average per cent change values are the mean of the individual experiments. 1 Standard error of the mean. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933002/ on 05/10/2017 Effect of corticosteroids on aqueous humor 537 Voiitme 8 Number 5 cility of the eye. Thus, we would expect to recover a greater proportion of infused inulin when there is a decrease in outflow facility and a smaller proportion when there is an increase in outflow facility. As we know the rate of perfusion, inulin concentration in perfusate, and rate of outflow, and can calculate rate of AH formation, it would be possible to estimate the actual volume of fluid passing through the outflow facility of the eye. However, a more simple and direct estimation of a change in outflow facility can be made by simply noting the change in the total amount of inulin recovered through the outflow cannula. Results Control experiments. A series of control experiments (30 eyes) was performed to obtain normal values of inulin recovery (Table I). AH formation rates and the percentage of infused inulin recovered were calculated for the first 2 hour period and for the following 4 hour period of each experiment. The mean rate of AH formation was 12.7 /.il per minute during the initial 2 hour period and 13.7 /.J per minute during the subsequent 4 hour period. These are similar to previously reported control values.10 During the first 2 hours of the experiment, 68.9 per cent of the infused inulin was recovered in the outflow, whereas 68.6 per cent was recovered in the subsequent 4 hour period. Thus, the percentage of inulin recovered is remarkably stable over a 6 hour experimental period, suggesting no change in outflow facility under control conditions. Intravenous hydro cortisone. A significant reduction in AH formation rate was noted after intravenous hydrocortisone when given in doses of 1 to 100 mg. per Table No. of experiments 10 Drug dose AH formation (nl/min.) Average per cent Control Drue, change} Inulin recovery (per cent infused, inulin) Average per cent Drug Control 100 21.0 ± 2.0| 12.7 ±1.0 13.3 ± 1.7 9.8 + 0.9 -38 ± 2.7 10 -22 ± 5.9 62 ±1.4 75 ±2.3 75 ±2.4 88 ±2.8 +23 ±4.3 +18 + 4.4 -24 ± 3.4 62 ± 3.5 75+1.9 +22 ±4.5 -15 + 3.5 56 ±2.5 72 ±3.5 +28 ± 4.5 +4 ±4.5 60 ± 3.3 62 ±4.0 +4 ±2.1 1 14.7 ±1.1 11.1 ±0.9 0.1 13.7 ± 0.7 11.6 ±0.7 0.01 13.1 + 0.5 13.7 + 0.9 "Hydrocortisone sodium succinate in the indicated quantities was given in a single intravenous injection at the end of a 2 hour control period. AH formation rates and inulin recovery values were calculated as shown in Table I. fThe average per cent change values are the mean of the individual experiments. J Standard error of the mean. Table III* No. of experiments Drug dose (tig/ml.) 100 10 AH formation (irt/min.) Average per cent Control Drue, changef 16.4±0.5| 16.2 ±1.2 -0.4 ±7.6 13.3 ±1.4 12.4+1.2 -4 +5.5 Inulin recovery (per cent infused inulin) Average per cent Control change Dm a 70 ±3.6 63 ± 2.3 74 ±2.5 70 ± 1.7 + 5.6 ±4 .0 +1.1 ±3 .7 61 + 2.7 + 9 + 3 .2 69 ± 3.6 1 16.0 ±2.0 15.5 ±2.0 -4 ±3.0 "Buffer, containing hydrocortisone sodium succinate in the indicated concentrations, was substituted for the control buffer at the end of the control period and was used for the rest of the experiment. AH formation and inulin recovery values were calculated as shown in Table I. fThe average per cent change values are the mean of the individual experiments. (Standard error of the mean. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933002/ on 05/10/2017 Investigative Ophthalmology October 1969 538 Oppelt, White, and Halpert kilogram (Table II). However, there was a significant increase in inulin recovery after doses of hydrocortisone ranging from 0.1 to 100 mg. per kilogram. This indicates a hydrocortisone-induced decrease of outflow facility, which is substantially the same at low or high doses of this agent. It should also be noted that at 0.1 mg. per kilogram of hydrocortisone there was still a maximum effect on outflow facility, while the reduction in AH formation rate was insignificant. Intracameral perfusion with hydrocortisone. Here we note that concentrations of hydrocortisone in the perfusate, ranging from 0.001 to 0.1 mg. per milliliter, produce no change in either AH formation rate or outflow facility (Table III). Intravitreous injection of hydrocortisone. At the beginning of each experiment, either 0.1 or 0.01 mg. of hydrocortisone was injected into the vitreous of one eye and the other eye was injected with an equal volume of AH buffer. There was no difference in AH formation rate or outflow facility in the hydrocortisone-injected eye, compared to the buffer-injected eye (Table IV). Topical application of hydrocortisone or dexamethasone (ophthalmic solution). In these experiments, after the 2 hour control period, hydrocortisone, either 0.25 or 0.025 mg., was dropped onto the cornea every 30 minutes for 4 hours. At the higher dose there was a 20 per cent decrease in AH formation rates with a 23 per cent increase in inulin recovery, indicating a decrease in outflow facility. Somewhat greater effects were noted toward the end of the experiment, suggesting a cumulative drug effect. Table IV* AH formation (nl/min.) No. of experiments 4 Drug dose injected (ne) 100 Control 15.4 ±1.9$ Drug 14.4 ±1.9 Inulin recovery (per cent infused inulin) Average per cent chang.e\ Control Drug Average per cent changed -6 ±2.6 66 + 3.9 73 ±4.4 +10 ±2.2 73 + 4.7 70 ± 4.3 4 13.0 ±1.1 -1±5.7 + 4 ±3.0 10 13.2± 1.1 °At the beginning of each experiment the vitreous of the control eye was injected with 100 /tl of AH buffer and the vitreous of the contralateral eye was injected with 100 /ttl of AH buffer containing hydrocortisone sodium succinate in the indicated quantities. Each injection was made with a Hamilton syringe and a 27 gauge needle through the sclera in the temporal quadrant of the eye, approximately 4 mm. posteriorly to the limbus. AH formation rates and inulin recovery values were calculated as shown in Table I. tThe average per cent change values are the mean of the individual experiments. t Standard error of the mean. Table V* AH formation (nl/min.) Drug Control Drug Average per cent change} 14.7 ±0.9$ 11.8 ±0.6 -20 ± 3.2 59 ± 3.6 73 ±5.0 +23 ± 2.6 13.2 ±1.7 12.1 ±0.5 - 8 ±2.5 56+ 1.2 62 ±1.8 +11+ 0.9 15.3 + 3.5 14.9 ±4.0 - 5±4.1 56 ± 12.7 64 + 2.4 +17 ±11.6 No. of experiments Control 6 0.25 (H) 6 0.025(H) 0.1 (D) 3 Inulin recovery (per cent infused inulin) Average per cent change} Drug dose (mg./half hour) 76 ±7.9 +13 ± 4.9 58+ 4.4 12.4 + 2.7 -18 + 4.0 4 0.4 (D) 14.0 ±2.5 "After a 2 hour control period, hydrocortisone sodium succinate (H) or dexamethasone ophthalmic solution (D), in the indicated quantities, was dropped directly onto the cornea of each eye every 30 minutes. AH formation rates and inulin recovery values were calculated as shown in Table I. | The average per cent change values are the mean of the individual experiments. t Standard error of the mean. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933002/ on 05/10/2017 Volume 8 Number 5 Effect of corticosteroids on aqueous humor 539 Smaller, but similar, changes in AH dynamics were noted after the smaller dose of hydrocortisone (Table V). In other cats, dexamethasone ophthalmic solution containing either 0.4 or 0.1 mg. of dexamethasone was dropped onto the cornea every half hour after the 2 hour control period. Particularly at the higher dose, a significant increase in inulin recovery was noted (indicating a decreased outflow facility) with a small, insignificant reduction in AH formation rate. This indicates that the outflow facility is more sensitive to dexamethosone than the AH secreting system. Discussion Continuous posterior-anterior chamber perfusion of the eye has proven to be a useful technique for the study of AH dynamics. We have used it to measure AH formation rates directly.10 Here it is particularly applicable, as drug effects can easily be determined because it is possible to use each eye as its own control and the measurements can be made independently of change in intraocular pressure. The current report describes the application of the technique to an estimation of a change in outflow facility of the eye. We found that the total amount of inulin recovered from the outflow facility is quite stable over a 6 hour experimental period (Table I). As inulin acts as an inert molecule in the eye,10 any change in the outflow facility of the eye, as long as the rate of infusion and the pressure of the system are kept constant, will be reflected in a change of the total quantity of inulin recovered through the outflow cannula. It is thus possible to determine and separate effects of pharmacologic manipulations on the AH formation rate and outflow facility. This, again, can be done using each eye as its own control and independently of any effects the agent may have on vascular volume of the eye, which might also affect IOP. There is agreement in the literature that topical corticosteroids frequently cause an increase in IOP. Becker4 suggests that this is more likely to happen in glaucomatous patients or their relatives and that the rise in IOP in response to corticosteroids can be used to make the diagnosis of "preglaucoma." Occasionally, increased IOP has also been observed after systemic corticosteroids are given. Most authors have suggested that the increase in IOP after topical or systemic corticosteroids is due to a decrease in the outflow facility, although a direct demonstration of such an effect has not been available. Our studies indicate that intravenous hydrocortisone has a moderate effect in reducing the rate of formation of AH. At very high doses (100 mg. per kilogram) a 38 per cent reduction in AH formation is noted; surprisingly, there still is some reduction in AH formation at 1 mg. per kilogram. Thus, the secretory system for AH seems to be quite sensitive to an acute increase in blood corticosteroid activity and responds to this by decreasing the rate of AH secretion. The increase in inulin recovery, noted after intravenous doses of hydrocortisone, indicates that there is a significant decrease in the outflow facility of the eye. It is interesting to note that the degree of response of the outflow facility does not change with different doses of hydrocortisone. For example, the effect noted at 100 mg. per kilogram is quite the same as the one noted at 0.1 mg. per kilogram. This suggests that the "receptor" controlling outflow resistance is extremely sensitive to systemic corticosteroids and has high affinity for the agent. This may be the explanation for the "all-or-none" type of response noted in the outflow resistance when using small doses of intravenous hydrocortisone. It is thus quite likely that the occasional increase in IOP noted after systemic corticosteroids is due to the effect of these agents on reducing the outflow facility. This system appears to be more sensitive to corticosteroids, at least by a factor of 10, than the one controlling AH secretion. This is seen at the 0.1 mg. per kilogram dose level when the effect on AH Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933002/ on 05/10/2017 Investigative Ophthalmology October 1969 540 Oppelt, White, and Halpert secretion is insignificant, while there is still a full effect on outflow facility. Perfusion of high and low concentrations of hydrocortisone through the eye chambers, as well as injection of the agent directly into the vitreous humor, did not cause any change in AH formation rates or inulin recovery. This indicates either that the agent does not reach the sites where secretion and outflow resistance are controlled or that these sites are sensitive to corticosteroids only from the blood side. This situation is somewhat similar to the response of AH formation to ouabain. Here, intravenous drug also is effective while intracameral drug is not.17 On the other hand, intravitreous ouabain has a profound effect in reducing IOP.18 Another possibility for the lack of effect produced by intraocular hydrocortisone is that the agent is rapidly inactivated in the eye. The effects of topical steroids, particularly dexamethasone, are quite intriguing. Here, again, we have a definite decrease in the outflow facility to the same degree as that seen with intravenous hydrocortisone. Again, especially with dexamethasone, we have the suggestion that the corticosteroid effect on outflow facility is considerably greater than the effect on AH formation. This may be the explanation for the observation that topical corticosteroids cause an increase in IOP more frequently than systemic steroids. It is very puzzling why there is such a striking effect on outflow facility when rather small quantities of corticosteroids are given topically, whereas there is no effect when large concentrations are perfused through the eye chambers or injected directly into the vitreous humor. It is difficult to pinpoint a molecular mechanism by which corticosteroids can reduce AH formation rate and outflow facility. One wonders about direct effect on ion transport or on blood vessels or blood flow. Recently, there have been suggestions that corticosteroids cause the mast cells in the trabecular network to release mucopolysaccharides.1'12 It is possible that this increases outflow resistance and may be the mechanism of the corticosteroid effect on outflow facility. REFERENCES 1. Armaly, M. F.: Effect of corticosteroids on intraocular pressure and fluid dynamics. I. The effect of dexamethasone in the normal eye, Arch. Ophth. 70: 482, 1963. 2. Armaly, M. F.: Effect of corticosteroids on intraocular pressure and fluid dynamics. II. The effect of dexamethasone in the glaucomatous eye, Arch. Ophth. 70: 492, 1963. 3. Becker, B., and Mills, D. W.: Corticosteroids and intraocular pressure, Arch. Ophth. 70: 500, 1963. 4. Becker, B.: Intraocular pressure response to topical corticosteroids, INVEST. OPHTH. 76: 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 484, 1966. Becker, B., and Chevrette, L.: Topical corticosteroids testing in glaucoma siblings, Arch. Ophth. 76: 484, 1966. Becker, B., and Hahn, K. A.: Topical corticosteroids and heredity in primary open-angle glaucoma, Am. J. Ophth. 57:543, 1964. Francois, J.: Heintz-De Bree, C , and Tripathi, R. C : The cortisone test and the heredity of primary open-angle glaucoma, Am. J. Ophth. 62: 844, 1966. Stern, J. J.: Acute glaucoma during cortisone therapy, Am. J. Ophth. 36: 389, 1953. Covell, L. L.: Glaucoma induced by systemic steroids therapy, Am. J. Ophth. 45: 108, 1958. Bernstein, H. N., and Schwartz, B.: Effects of long-term systemic steroids on ocular pressure and tonographic values, Arch. Ophth. 68: 742, 1962. Bernstein, H. N., Mills, D. W., and Becker, B.: Steroid-induced elevation of intraocular pressure, Arch. Ophth. 70:15, 1963. Spiers, F.: Unilateral acute rise in intraocular pressure following long-term bilateral local treatment with prednisone (ultracortenol) in a case of uveitis, Acta ophth. 43:323, 1965. Nicholas, J. P.: Topical corticosteroids and aqueous humor dynamics, Arch. Ophth. 72: 189, 1964. Tuovinen, E., Esila, R., and Liesmaa, M.: The influence of corticosteroids on intraocular pressure in rabbits. III. The immediate influence of massive intravenous doses of betamethasone and dexamethasone on the intraocular pressure of the rabbit eye, Acta ophth. 44: 823, 1966. Linner, E., and Wistrand, P. J.: Adrenal cortex and aqueous humor dynamics, Exper. Eye Res. 2: 148, 1963. Oppelt, W. W.: Measurements of aqueous Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933002/ on 05/10/2017 Volume 8 Number 5 Effect of corticosteroids on aqueous humor 541 humor formation rates by posterior-anterior chamber perfusion with inulin: Normal values and the eflFect of carbonic anhydrase inhibition, INVEST. OPHTH. 6: 76, 1967. 17. Oppelt, W. W., and White, E. D., Jr.: Effect of ouabain on aqueous humor formation rate 18. Bonting, S. L., and Becker, B.: Studies on sodium-potassium activated adenosine triphosand aqueous humor flow in the rabbit eye after intravitreal injection of ouabain, INVEST. OPHTH. 3: 523, 1964. phatase. XIV. Inhibition of enzyme activity in cats, INVEST. OPHTH. 7: 328, 1968. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933002/ on 05/10/2017