Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
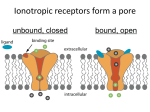
contact Leonardo Mastropasqua – [email protected] Update GLAUCOMA Trans-scleral outflow Current glaucoma treatments do not fully exploit the trans-scleral outflow pathway Courtesy of Leonardo Mastropasqua MD by Roibeard O’hEineachain in Milan Figure 1: Planar reconstruction of the superior bulbar conjunctiva in an eye with ocular hypertension. Microcysts appear as optically clear spaces within the conjunctival epithelium of the bulbar conjunctiva, indicating the trans-scleral aqueous humour passage “I n the near future, improving the trans-scleral outflow of aqueous humour could represent an important strategy for reducing intraocular pressure (IOP) in patients with glaucoma,” said Leonardo Mastropasqua MD, director of the Excellence Eye Centre at the University G d’Annunzio of Chieti-Pescara, Chieti, Italy. During his keynote speech at the Glaucoma Day sessions at the XXX Congress of the ESCRS, Prof Mastropasqua stated: “Transscleral outflow is the last step of the uveoscleral outflow pathway and plays a key role in ocular hydrodynamics. In fact, the sclera has a good hydraulic conductivity and offers poor resistance to aqueous humour passage. The sclera is also a very accessible structure for surgery.” He also noted that the human eye has two main pathways for aqueous outflow: the trabecular and the uveo-scleral outflow pathway. The first accounts for 80 per cent of aqueous outflow and the second for 20 per cent, on average, with measurements ranging from 12 per cent to 54 per cent. He explained how the aqueous humour that flows out from the anterior chamber through the uveo-scleral pathway first passes between the ciliary muscle bundles into the supraciliary and suprachoroidal spaces. Hence, aqueous humour drains either towards the choriocapillaris, reaching the blood circulation, or externally, passing through the sclera and conjunctiva. From here, final aqueous humour resorption is guaranteed by lymphatics vessels and veins, or by trans-conjunctival passage towards the ocular surface. All these terminal outflow pathways bring aqueous to extra-orbital tissue. Adding that uveo-scleral outflow EUROTIMES | Volume 18 | Issue 2 Figure 2: Slit-lamp image showing a cystic/diffuse functioning filtering bleb (A). In vivo confocal microscopy the conjunctiva shows numerous and wide fluid-filled hyporeflective microcysts, indicating the aqueous humour passage through the bleb-wall (B) tends to decrease with age because of an accumulation of fibrillar extracellular material in the ciliary muscle and ciliary processes. Improving uveo-scleral pathways At present there are both medical and surgical approaches to increase uveo-scleral outflow in eyes with glaucoma. For example, prostaglandin analogues improve this pathway by widening and decompressing the connective tissue in the ciliary muscle and remodelling the extracellular matrix by increasing the secretion of matrix metalloproteinases. Among surgical procedures, cyclodialysis increases both the rate of uveo-scleral (by a factor of four) and trans-scleral outflow. However, the procedure has a high frequency of complications, which can themselves result in a high rate of failure and elevated IOP. Another surgical possibility is to place a shunt between the suprachoroidal space and the anterior chamber, Prof Mastropasqua said. Although the treatment is effective at first, the lumen of these implants are prone to encapsulation and obstruction of flow with fibrous connective tissue. Improving trans-scleral pathways Another possibility is treatments focusing specifically on enhancing the trans-scleral portion of the uveo-scleral outflow, Prof Mastropasqua said. Laboratory studies have shown that the potential outflow of aqueous through the sclera is two to three times higher in vitro than it normally is in vivo, in the eye of a patient. Interestingly, in patients affected with untreated ocular hypertension or medically treated open angle glaucoma, trans-scleral outflow is two to five times greater than in healthy subjects, probably representing an adaptive mechanism for overcoming the increased trabecular resistance to aqueous outflow. (Ciancaglini et al. Invest Ophthalmol Vis Sci. 2008; 49(7):3042-8. Agnifili et al. Acta Ophthalmol. 2012;90(2):e132-7. doi: 10.1111/j.1755-3768.2011.02255.x.). Exploiting that potential through surgical or medical approaches could represent a useful strategy for IOP reduction, alternative to the current fistulasing procedures. Besides in vitro measurements, transscleral outflow may also be measured in vivo, by using laser scanning confocal microscopy to evaluate the density and surface of conjunctival epithelial microcysts. These microcysts represent the hallmark of the trans-conjunctival passage of the aqueous humour, as reported by Ciancaglini and Mastropasqua in 2008 (1. Ciancaglini et al. Invest Ophthalmol Vis Sci. 2008; 49(7):30428) (Figure 1). These structures were first described within the bleb wall of functioning trabeculectomy (Figure 2). Prof Mastropasqua and his associates reported epithelial microcysts were greater in both size P=0.017) and number (P=0.014) in the successful blebs when compared to failed blebs (Ciancaglini et al. J Glaucoma. 2008. 17(4):308-17.). As is the case with uveo-scleral outflow in general, there are already both medical and surgical techniques that specifically enhance trans-scleral aqueous outflow, he noted. For example, prostaglandin analogues increase the trans-scleral permeability by increasing the secretion of matrix metalloproteinases, which lead to remodeling of collagen fibres . Surgical procedures that thin the sclera may potentially lead to a significant enhancement of the trans-scleral aqueous humour outflow. This was originally reported in the partial thickness laminar dissection of the sclera, he said. Currently, different surgical approaches work by also reducing the scleral thickness. Canaloplasty, a standardised treatment that improves the trabeculo-canalicular outflow, appears to increase aqueous outflow also through the sclera and conjunctiva. Unlike trabeculectomy, a conjunctival bleb is not created since a watertight suture at the site of surgery is mandatory. However, like trabeculectomy it does increase the size and concentration of epithelial microcysts; probably because the sclera is thinned at the surgical site. In a study involving a series of 30 patients who underwent canaloplasty, there was a four-fold increase from baseline in the number of conjunctival microcysts in the 27 eyes in which the procedure was successful, but the microcyst concentration did not increase significantly in the eyes in which the procedure was unsuccessful (Mastropasqua et al. Br J Ophthalmol 2012; 96:634-639). New techniques Other techniques now in the pre-clinical phase of investigation include the creation of intrascleral canals injected with non-animal stabilised hyaluronic acid (NASHA). A study involving porcine eyes showed that the scleral canals had a significantly higher rate of aqueous outflow than control eyes (Mavrakanas et al. Invest Ophthalmol Vis Sci. 2009; 50: 37593762). Techniques that create intrascleral canals with femtosecond lasers may be even more promising. A three-dimensional finite element model indicated that creating partial thickness intrascleral channels may reduce IOP from 67.2 per cent to 80.6 per cent (Chai et al. Lasers Surg Med. 2008;40:188-195). In addition, an in vivo study showed that rabbit eyes that had undergone scleral channel creation with a femtosecond laser had significantly lower IOP than the contralateral control eyes. The IOP reduction appeared to result from an increase in aqueous humour outflow through the sclera (Chai et al. Lasers Surg Med. 2010; 42(7):647651). The investigators used a titanium/ sapphire laser system tuned to the wavelength of 1.7 microns with an optical parametric amplifier. They scanned the femtosecond laser beam along a rectangular raster pattern to create partial thickness subsurface drainage channels in the sclera. Prof Mastropasqua concluded, “Scleral thinning with a femtosecond laser represents a valuable field of research in glaucoma surgery and may enhance trans-scleral outflow while avoiding sub-conjunctival aqueous humour percolation and bleb formation.” 21