Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
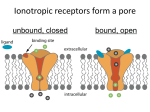
Glaucoma Viviany Taqueti and Scott Vafai HST 150 What is glaucoma? • Optic neuropathy that is the leading cause of irreversible blindness in the world • Major types are open angle and closed angle • Differences among various types of glaucoma complicate the nomenclature • Glaucoma is commonly associated with elevated intraocular pressure (IOP), but the disease can occur in the context of normal IOP • Our understanding and treatment of the disease is very focused on IOP From www.ahaf.org Case 1 Mr. S presents to you with diminished peripheral vision. He complains that he feels like the world is closing in on him. He also notes that he has trouble looking at lights as they all appear to be surrounded by halos. You perform fundoscopic and gonioscopic exam with tonometry and diagnose glaucoma. Open Angle Glaucoma • Obstruction at the level of the trabecular meshwork • Progressive loss of visual field over time from periphery to center • Presence of hollowed out optic disc (‘cupping’) due to retinal ganglion cell death • Open anterior chamber angle • Majority of patients have IOP > 21 mmHg, asymptomatic From http://www.merckfrosst.ca/e/health/glaucoma/glaucoma/classify/home.html Case 2 Mrs. P is a 65 yr. old female who has become acutely ill in the waiting room. An ophthalmologic assistant had dilated her eyes in preparation for examination. She is now complaining of nausea, diaphoresis and pain in her right eye, which is now red and swollen. Closed Angle Glaucoma • Apposition of iris and trabecular meshwork • Parasympatholytics (pupillary dilation) can precipitate attack • Increase risk with age, increase in volume of lens • Acute onset, patient complains of nausea, headache (rather than eye ache), malaise, general distress • Requires immediate treatment BOTTOM LINE: IOP from Aqueous Flow, 3 Sites 1. Obstructed Trabecular Mesh Open Angle: Age-related, genetic Closed Angle: Anatomic, exacerbated by: 2. Pupillary Block Dilation of pupil iris flattens, flow via pupil, iris forward iris-cornea angle 3. Swelling of Ciliary Body 1 2 3 Modified from: Wood et al. NEJM 339:1298 (1998) SIDENOTE: WHY WOULD YOU WANT TO DILATE MRS. P’s PUPILS WITH PHENYLEPHRINE VS. AN ANTICHOLINERGIC? REVIEW: Autonomic NS Effect on the Eye RECEPTOR ACTIVATION WILL: TO LOWER IOP, AIM FOR: IRIS, Circular Fibers mAchR : Constrict Pupil Activity IRIS, Radial Fibers 1 R Activity CILIARY MUSCLES mAchR : Contract for Accomodation 2 R : Relax for Far Vision : Dilate Pupil Activity Activity Modified from: http://pharma1.med.osaka-u.ac.jp/textbook/Autonomic/Autonomic.html TREATMENT RATIONALE LOWER IOP BY: (1) Decreasing Production of Aqueous Humor (2) Increasing Outflow of Aqueous Humor Focus on Pharmacologic Rx: First-line DRUGS THAT DECREASE AQUEOUS PRODUCTION I. Beta-Blockers [levobunolol, timolol, carteolol, betaxolol] -Mechanism: Act on ciliary body to production of aqueous humor -Administration: Topical drops to avoid systemic effects -Side Effects: Cardiovascular (bradycardia, asystole, syncope), bronchoconstriction (avoid with 1-selective betaxolol), depression II. Alpha-2 Adrenergic Agonists [apraclonidine, brimonidine] -Mechanism: production of aqueous humor -Administration: Topical drops -Side Effects: Lethargy, fatigue, dry mouth [apraclonidine is a derivative of clonidine (antihypertensive) which cannot cross BBB to cause systemic hypotension] III. Carbonic Anhydrase Inhibitors [acetazolamide, dorzolamide] -Mechanism: Blocks CAII enzyme production of bicarbonate ions (transported to posterior chamber, carrying osmotic water flow), thus production of aqueous humor -Administration: Oral, topical -Side Effects: malaise, kidney stones, possible (rare) aplastic anemia DRUGS THAT INCREASE AQUEOUS OUTFLOW I. Nonspecific Adrenergic Agonists [epinephrine, dipivefrin] -Mechanism: uveoscleral outflow of aqueous humor -Administration: Topical drops -Side Effects: Can precipitate acute attack in patients with narrow iriscorneal angle, headaches, cardiovascular arrhythmia, tachycardia II. Parasympathomimetics [pilocarpine, carbachol, echothiophate] -Mechanism: contractile force of ciliary body muscle, outflow via TM -Administration: Topical drops or gel, (slow-release plastic insert) -Side Effects: Headache, induced miopia. Few systemic SE for direct-acting agonists vs. AchE inhibitors (diarrhea, cramps, prolonged paralysis in setting of succinylcholine). Why isn’t Ach used? III. Prostaglandins [latanoprost] -Mechanism: May uveoscleral outflow by relaxing ciliary body muscle -Administration: Topical drops -Side Effects: Iris color change LOWERING IOP SLOWS PROGRESSION OF VISUAL LOSS OPEN ANGLE GLAUCOMA Early Manifest Glaucoma Trial: -1st (adequately powered) randomized trial with untreated control arm to evaluate effects of IOP reduction in patients with open-angle glaucoma. -Treatment significantly delayed progression. IN Rx GLAUCOMA: ADDITIONAL CONSIDERATIONS 1. No single medication can be used in all patients 2. Compliance - Critical: Rx often requires several agents, multiple times a day, everyday Role of slow-release drug delivery devices (Langer) 3. Non-pharmacologic ways to lower IOP: - Laser (argon laser trabeculoplasty) - aqueous outflow, loses effectiveness over time Surgical (trabeculectomy) - Creates alternative path for aqueous outflow - Only definitive therapy for closed angle 4. Effectiveness of Rx measured by ability to lower IOP, but other factors may be (more) important: - Neuroprotection/increased blood flow to optic nerve GLAUCOMA: Key Points • Glaucoma: -Visual loss from optic neuropathy -Open angle chronic, Closed angle acute -Final common pathway: IOP (usually) • Drug Rx: -All directed towardsIOP either via: - aqueous production: Beta blockers Alpha-2 agonists Carbonic anhydrase inhibitors - aqueous outflow: (Adrenergic agonists, nonspecific) Parasympathomimetics Prostaglandins • Treatment slows progression • Understanding ANS effect on the eye is critical for reasoning through drug mechanisms of action • Understanding ANS effect on the whole body is critical for predicting and avoiding dangerous side effects