Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Globalization and disease wikipedia , lookup
Urinary tract infection wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Germ theory of disease wikipedia , lookup
Neonatal infection wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Whooping cough wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
CHILDRENS COUGH.
ACUTE PNEUMONIA
Lecture course for students of six-year
Associate professor
Abdusagatova Sh.Sh.
Cough
This is a protective
reaction of organism,
helps to restore
breathing passages
CHILDREN COUGH
Can occur in many diseases, but most often it is
a symptom of acute respiratory infection and
develops within 48 hours of onset.
The main causes of cough
Respiratory infections of the upper and lower
respiratory tract
Bronchial asthma
Foreign body aspiration
Chronic bronchopulmonary disease
Cystic fibrosis
Whooping cough
Tuberculosis
Other (swelling, pulmonary edema, etc.)
Causes of cough
Respiratory infections of the upper respiratory tract:
Rhinitis, rhinosinusitis
Syndrome of postnasal streaks
Pharyngitis
Adenoids grade 2-3
Acute constrictive laryngitis (croup)
Causes of cough
Lower respiratory tract
infections:
Tracheitis
Bronchitis
Pneumonia
The main causes of cough
Diseases of the cardiovascular system:
-heart failure
-heart disease
-pericarditis
The main causes of cough
Diseases of the gastrointestinal tract:
- gastroesophageal reflux
-hiatal hernia
The main causes of cough
Diffuse connective tissue disease
Medical reasons ("kapotenov" cough)
Iatrogenic causes (postintubatsionny syndrome)
Smoking (including passive)
The pathogenesis of cough
One of the main factors is a violation of
mucociliary clearance
This is due to excess formation and / or
increased viscosity of bronchial secretions
The pathogenesis of cough
Stagnation of the bronchial contents leads to
disruption of ventilation-protective function of
the lungs,
infection - the development of endobronchial or bronchopulmonary inflammation
The pathogenesis of cough
Produced by viscous secret may cause bronchial
obstruction due to accumulation of mucus in the
respiratory tract
The pathogenesis of cough
In severe cases of violations of air accompanied by the
development of atelectasis
Mucociliary transport
- Is a critical mechanism to ensure sanitation of
the respiratory tract.
Its speed of a healthy person
4 - 20 mm / min
Normally a day transported from 10 to 100 ml of
bronchial secretions
Bronchial secretion
Normally has a bactericidal effect
The pathology observed
compensatory increase of mucuse .
Increases the viscosity of sputum
Increased adhesion of pathogens to mucosal
Favorable conditions for the reproduction of
microorganisms
Reduced the bactericidal properties of mucus
Infectious agents and toxins have adverse effects on the
mucous
The drainage function of the
bronchial tree
Violations can result in her not only to vent
violations, but also reduce the local
immunological respiratory protection at high
risk of a protracted course of the inflammatory
process and contribute to its perpetuation.
Inflammation of the respiratory tract is a major
pathogenic element in the development of
mechanisms of bronchial obstruction
(bronchospasm, hypersecretion of viscous
mucus, swelling of the bronchial mucosa)
Children acute
pneumonia
Children Cough
Two of the three children attending the
clinic to see a doctor - it is children, with
complaints of cough
Acute Pneumonia
-acute infectious disease of lung parenchyma,
diagnosed by respiratory distress syndrome and
physical data, as well as infiltrative or focal
changes on chest radiograph.
Statistics
The average incidence of children aged 0 to 15
years is 7.1 per 1000 children per year
Up to 1 year - 11.4 per 1,000
1-4 years - 13.9 per 1,000
5 - 15 years - 3.7 per 1000
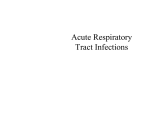
Другие
заболевания
24,4%
Травмы и
Отравления
9,7%
Инфекционные заболевания 5,5%
Врожденные
Аномалии
7,5%
Болезни
Органов
Дыхания
46,4%
Features breathing of children
Short airways
Weak expression of epithelium lining the
respiratory tract, track their vulnerability
The horizontal position of the ribs, the low mobility of
the chest
High standing of the diaphragm
Dimensions of light relatively larger than the size of the
chest
Incompleteness of bronchopulmonary apparatus
Factors predisposing to
pneumonia
From an unfavorable social environment
With variations in health status (rickets, malnutrition,
anemia, etc.)
With a family history (on bronchopulmonary and allergic
diseases)
With perinatal disorders
With congenital malformations of the respiratory and cardiac
Since hereditary pathology
On the anomalies of the Constitution
Chronic foci of infection and hypothermia
The main functions of the lungs
Respiratory
Protective and adaptive
Surfactant-producing
The protective function of the lungs
Upper sections of the mucociliary system
Average departments - BALT
(bronhoassotiation lymphoid tissue)
Lower sections, alveolar macrophages, serum
immunoglobulin A
Respiratory cycle
Phase of respiratory
The diffusion of gases through the alveolarcapillary membrane lung
Transport of oxygen in the blood to tissues
Oxygen permeability through the membrane of
the capillaries in the mainstream of the
microcirculation
Tissue (cellular) respiration
Surfactant-producing lung
function
Prevents atelectasis on expiratory
Supports normal permeability aerogematic barrier of the lungs
Creates an optimum level of filtration pressure in the pulmonary
microcirculation
Prevents edema pulmonary epithelium and vascular endothelium
Plays the role of antibodies to create an immune barrier in the
lower regions of the lung tissue
The etiology of pneumonia
Pneumococci (65-85%)
Gold stafillokokk
Haemophilus influenzae
Gram-negative flora
The etiology of pneumonia
Stafilococcus
Klebsiella
Pseudomonas aeruginosa
The etiology of pneumonia of
infants
Viruses, mycoplasma (antenatal pneumonia )
colon bacillus
Stafillococcus
Klebsiella
Proteus
enterobacteria
Blue pus bacillus
pathogenic viruses
pnevmotsisty
The pathogenesis of P.
Paths of infection
The mechanism of NAM
Genesis of the formation of metabolic and
functional changes in organs and systems
Paths of infection
Bronchiogenic
Hematogenous
Lymphogenous
Forms DS
Ventilation.
Diffusion
Perfusion-Distribution
Restrictive
Pneumonia in a child is not a local disease, the
development of pneumonia is accompanied by
involvement in the process of not only
metabolic but also in many other organs.
Metabolic and functional
impairment in OP
Water deficit (shortness of breath, fever)
Gipernatremiya, decreased urine output,
increased ADH
violation of CBS
DIC
Increased proteolytic activity
Metabolic changes in the myocardium
Increased blood pressure
Violation of liver detoxification
Renal impairment
bowel dysfunction
Classification of acute pneumonia
In the form:
lobular
segmental
lobar
interstitial
Classification of the AP in
accordance with the severity of
uncomplicated
complications:
NAM
toxemia
Classification of AP
Adrift
Acute (up to 3 months)
Prolonged (more than 3 months)
Mycoplasma pneumonia
Can develop at any age
Incubus. Period 1-3 weeks
Start gradually
Catarrhal conditions, fever
Frequent debilitating cough up to 3 weeks.
NAM expressed
Physical data clearly
X-ray: interstitial changes
Treatment: macrolides are effective
Pneumocystis pneumonia
More common in premature infants, those
receiving corticosteroids, cytotoxic drugs
The incubation period is 2-3 weeks.
Start slow, the symptoms of intoxication
Painful cough with foam from the mouth
In sputum, pnevmotsisty
In the lungs, Physical data scarce
DN grade 2-3
X-ray "padded easy"
Stafillokok pneumonia
More often in children 1 year of age
fever
toxemia
Hepato-splenomegaly and
diarrhea
Krepitiruschie crackles in the lungs
Pulmonary and extrapulmonary complications
Anemia, leukocytosis
Klebsiellez pneumonia
Gram-rod
Hospital infection
acute onset
intoxication
In the lungs, necrotic and hemorrhagic changes,
"creeping pneumonia"
Abscesses, pneumoempyema
Metastases, sepsis
Chlamydial pneumonia
More often in children younger than 6 months.
Start gradually
Catarrhal conditions, conjunctivitis, vaginitis
dyspnea
Kryahtyaschee breath
cough pertussoid
In the lungs, wheezing krepitiruyuschie
during prolonged
Virus pneumonia
More often the exception than the rule
Observed during an influenza outbreak
hemorrhagic pneumonia
Fungal pneumonia
In protracted infections in children with eating
disorders, digestive diseases, immune defects
Cough with expectoration of gelatinous
Anorexia, fever, sweats Heavy
In sputum - fungi
Yeast, lactic dermatitis
The effect of antifungal drugs
Deterioration in the background of antibiotic
therapy
Criteria for pneumonia
Respiratory complaints
The syndrome of intoxication
Respiratory distress syndrome
Local changes in lung
Infiltrates and patchy shadows on chest
radiograph
Rapid breathing (WHO criteria)
60 Up to 2 months or more / min
12.2 months - 50 or more
1 - 5 years - 40 or more / min
Complications of pneumonia
Bulla
abscesses
pyothorax
pneumothorax
mediastinal emphysema
pericarditis
osteomyelitis
sepsis
Treatment of pneumonia
Provision of urgent measures
Treatment in the somatic hospital or ambulatory
on a "hospital at home"
Follow-up care in the office of Rehabilitation
Clinical supervision for 6-12 months.
Treatment of pneumonia
causal treatment
-antibiotics
immunoglobulinpathogenetic therapy
NAM-fighting
-fight against cardiovascular disorders
-detoxification
physiotherapy
stimulation therapy
therapeutic exercise
Indications for hospitalization
Severe manifestations or complications
Focal and confluent pneumonia
prolonged duration
Pneumonia in disadvantaged background
(anemia, dystrophy, premature birth, etc.)
Treatment failure within 24-36 hours
Hospital at home
lack of toxicity
The absence of respiratory distress
The absence of cardiovascular dysfunction
Antibacterial therapy
Up to 6 months: first fell ill - ampicillin,
oxacillin, ampioks
Re - cephalosporins, aminoglycosides
Older than 6 months: ill the first time:
penicillin
Re-cephalosporins, aminoglycosides
Urgent actions
correction of hyperthermia
correction NAM
Normalization of pulmonary and peripheral
microcirculation
stabilization of the surfactant
Correction of hyperthermia
Cooling compress on my head
Acetic alcohol rubbing of the skin
Gipopiretiki: analgin, Panadol, Paracetamol, etc.
Antispasmodics: No-Spa, papaverine,
aminophylline, komplamin
Neurovegetative blockers: droperidol, pipolfen
Correction of the NAM and tissue
hypoxia
elevated position
aeration Chamber
Removing mucus from the respiratory tract
Oxygen
The elimination of hypokalemia and paresis of
the intestine
Tissue oxidants: riboflavin, cocarboxylase,
cytochrome C, nicotinamide
Correction of the pulmonary
microcirculation and bronchial
patency
Antispasmodics: aminophylline, no-spa,
papaverine, komplamin.
Antiplatelet: chimes, trental
B \ IV infusion: glucose, Lasix
glucocorticoids
Protease inhibitors: contrycal
Correction of surfactantproducing lung function
Dimefosfon (50 mg \ kg \ day)
Essentiale (w / w, 0.3 ml / kg / day)
Tocopherol (10mg/sut)
Glycerol (mixed to spray)
Ambroxol, Bromhexine
GVEK (glucose, vit.S, cocarboxylase,
cytochrome C)
Treatment of children cough
- Improving the drainage
function of bronchi
-restoration of adequate
mucociliary clearance
-anti-inflammatory
therapy
bronchodilator therapy
Treatment of children cough
The need to suppress cough, using real
antitussive drugs in children are rare, their
application to the pathophysiology of positions
is not justified.
Treatment of children cough in
Effective antitussive
therapy should not be to
suppress cough, and his
gain, subject to the
transfer of dry cough in
the productive.
Improving the drainage function
of bronchus
- Active oral rehydration
- The use of expectorants and mucolytic agents
- massage
- postural drainage
- breathing exercises
Means stimulating expectoration
Reflexively acting drugs:
Thermopsis, alteyka, licorice, terpingidrat,
essential oils, etc.
Drugs resorptive action:
Potassium iodide, ammonium chloride, sodium
bicarbonate, etc.
Means stimulating expectoration
(deficiencies)
Can significantly increase the volume of
bronchial secretions, which can lead to
significant disruption of drainage of lung
function, especially in young children, and
reinfection
Mucolytic drugs
is optimal for the
treatment of respiratory
diseases in children.
Bromhexine
Ambroxol
acetylcysteine
Mesnil
proteolytic enzymes
Proteolytic enzymes
Trypsin, chymotrypsin, RNA-ase
Reduce the viscosity and elasticity of sputum,
have edematous and anti-inflammatory action.
Practically not used in pulmonology
Mucolytic drugs
Acecylsysteine reduces the viscosity of mucus,
contributes to liquefaction of pus.
Indications: acute, recurrent and chronic
diseases of the respiratory tract, accompanied by
the formation of viscous mucus.
Mucolytic drugs
Bromhexine-has mucolytic, mukokineticheskim
and expectorant action.
Indications: acute and chronic bronchitis, acute
pneumonia, chronic bronchial disease.
Mucolytic drugs
Ambroxol-mucolytics new generation is a
metabolite of bromgeksina has a more
pronounced expectorant effect, affects the
synthesis of bronchial secretions, liquefies
phlegm and increases content of surfactant in
the lungs does not cause bronchial obstruction,
has anti-inflammatory and immunomodulatory
effects.
Treatment of children cough
When the complex treatment of respiratory
diseases, accompanied by a cough, mucolytic
agents are preferably used with multiple dosage
forms.
tablets
syrups
capsules
Solutions for oral
inhaled form
Bronchodilator therapy
Salbutamol (betta2-agonists)
Atrovent (anticholinergic drugs)
Aminophylline (theophylline short-acting)
Anti-inflammatory therapy
NSAIDs
antibiotics
glucocorticoids
fenspiride
Thank you for your attention!