Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
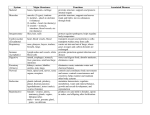
SEX CHROMOSOME ABNORMALITIES Sometimes during meiosis, the paired (MI) or daughter chromosomes (MII) go to the same pole. This is described as "nondisjunction". If nondisjunction involves the sex chromosomes, it results in eggs or sperm with abnormal numbers of X and/or Y chromosomes. In eggs, a single nondisjunction event leads to XX eggs and O (no X chromosome) eggs. Fertilization of an XX egg with an X sperm producesXXX (Triplo X) females Fertilization of an XX egg with a Y sperm produces XXY (Klinefelters) males. Fertilization of an O egg with an X sperm leads to XO (Turners) females Fertilization of an O egg with a Y sperm is lethal Nondisjunction in males can lead to XX, XY, O and YY sperm. Combining these with an X egg will produce the syndromes described above plus XYY(Jacobs). Females with the karyotype 47; XXX are fertile, tend to have XX and XY offspring, generally fall in the normal range of IQ, and have no distinguishing characteristics. Many are considered "shy" when young and may be delayed in social development. There is great tendency for metal retardation when there are 4, 5, or 6-X chromosomes present. Overall frequency: about 1 in 4,000 live births. Females with Turner syndrome (45; XO) are very short, sterile, and have problems with "spatial" tests but otherwise tend to fall in the normal IQ range. Development of secondary sex characteristics and stature can be addressed by hormone therapy. Heart and kidney problems are also common. Frequency: 1 in 2,000 to 1in 2,500 live female births Klinefelter males (47; XXY) tend to be tall, are infertile with very small testes, generally lag in development of language skills, and often display breast development at puberty. The latter is easily treated with testosterone, but fertility is not restored. Frequency is estimated at 1 in 500 to 1 in 1,000 male births. XYY males (Jacob syndrome) also tend to be taller than average and have problems withacne but are fertile and have XY and XX children. As a group they generally fall near the normal IQ range. Although there is increased"risk" for XYY males to end up in penal institutions (populations there are about 1 in 300 males compared to 1 in 1,000 at birth) the vast majority are in the normal population. Early studies suggesting "super" aggressive male behavior have not been borne out. SEX DETERMINATION Based on the previous information, it is clear that the primary determinant of sex in humans is the presence or absence of the Y chromosome, which is determined at fertilization; no Ys results in female development; 1 Y, no matter how many Xs, produces male development. Special cells that can develop into gonads where meiosis takes place are set aside very early in embryology. The tissue is called "ovotestes" since it can develop into either ovaries or testes. Mullerian ducts are present that can develop into female internal components. Wollfian ducts that can develop into male components are present. If a Y chromosome is present all the cells will display Hy antigen, a cell surface protein coded by a gene on the Y chromosome. After about 7 weeks, another Y encoded gene (called Tdf for testes determining factor, or Sryf or sex-region of Y) is activated and directs ovotestes to develop into testes. Testes produce androgens, including testosterone, which induces development of the Wollfian ducts and regression of the Mullerian ducts. After about 11 weeks, in the absence of a Y chromosome, female development is initiated with the conversion of the ovotestes into ovaries, regression of Wollfian ducts, and development of Mullerian ducts. Hormonal changes at puberty further advance sexual development. Gonadotropic hormones (FSH and LH) from the pituitary, via a signal from the hypothalamus, start monthly cycle of egg maturation and release in females which increases estrogen, which decreases FSH and LH, etc. In males, trace levels of the same hormones lead to induction of secondary sex characteristics, (beards, voice, etc.). Adrenal hormones lead to puberty changes in females. Very few if any of the genes needed for sexual development/identity are on the sex chromosomes. After birth, it becomes difficult to separate genetic effects from non-genetic effects since males and females often are treated with "different expectations". As would be predicted since many hormones are involved, each of which is produced via biosynthetic pathways, many different mutations can affect normal sexual development. The bulk of the genes are not sex-linked or holandric, but are located on somatic chromosomes. Examples of genetic defects that alter sex development include: Tfm, an X-linked gene that codes for testosterone receptors. Females whoare XTfmXtfmare normal. Their XtfmY progeny, expected to be males, developinto sterile females (condition is called testicular feminization or completeandrogen insensitivity). Although the ovotestes become testes andproduce testosterone, it has no effect, so the outward and mentaldevelopment becomes female. Unfortunately, the Mullerian ductsdisintegrate so there is no chance of fertility, and the undescended testesshould be removed after puberty to diminish the risk of cancer. In guevodoces, infants are classified as female at birth based on external genitalia. At puberty they "convert" to fully functional males; which some, but not all have claimed to be all along. When hormone therapy or surgery is used, the best bet is to make the appearance match the "brain-sex" of the individual.