Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
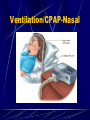
Acute Interventions for the Chronic Care Patient Ray Taylor Valencia Community College Topics Home Health Care Home Care Providers Home Care Pathologies ALS Support for Home Care Patients Hospice Introduction A major trend of health care involves the shifting of patients out of the hospital and back into their homes as soon as possible. The result has been a huge increase in home health care services. Epidemiology of Home Care A number of factors have promoted the growth of home care in recent years. They include: Enactment of Medicare in 1965 The advent of HMOs Improved medical technology Changes in the attitudes of doctors and patients toward hospital care In 1992… Almost 75% of home-care patients were age 65 or older. Of the elderly home-care patients, almost two-thirds are female. Responses to Home Care A number of situations may involve you in the treatment of a home-care patient: Equipment failure Unexpected complications Absence of a caregiver Need for transport Inability to operate a device Home Health Care Home health care problems requiring intervention by a home health practitioner or physician Chemotherapy Pain management Hospice care Figure 6-3 Types of Home Care Patients Airway pathologies Inadequate pulmonary toilet Inadequate alveolar ventilation Inadequate alveolar oxygenation Circulatory pathologies Alterations in peripheral circulation GI/GU pathologies Ostomies Catheters Home dialysis Types of Home Care Patients Infections Cellulitis, sepsis Wound care Surgical wound closure Decubitus wounds Drains Hospice care Maternal child care Apnea monitors New parent Progressive dementia in the patient at home Chronic pain management Home chemotherapy Transplant candidate Infection and Ulceration Home Health Preparation Table 6-4 Prevention Table 6-5 General System Pathophysiology Assessment/Management Assessment of the home-care patient follows the same basic steps as any other patient. The one thing home-care calls have in common is their diversity. Try to ascertain from the primary health care provider a baseline presentation for the patient. Patient Assessment Assessment Scene size-up Body substance isolation Safety Infectious waste issues in home care environment Pets Firearems Milieu Ability to maintain a healthy environment Adequate nutritional support available (electricity, heat, etc.) Common Acute Home Health Situations Respiratory disorders COPD Bronchitis Asthma CHF Cystic fibrosis Bronchopulmonary dysplasia Common Acute Home Health Situations Neuromuscular degenerative diseases Muscular Dystrophy Poliomyelitis Guillain-Barré Syndrome Myasthenia Gravis Patients awaiting lung transplants Sleep apnea Respiratory Disorders Account for more than 630,000 of hospital patients discharged for home care annually Simple pneumonia and pleurisy account for 37% COPD accounts for 50% Respiratory Pathology Increased risk of airway infections in the respiratory compromised patient Progression of chronic respiratory diseases Increased secretions Obstructed or malfunctioning airway devices Improper application of medical device Common Respiratory Equipment Oxygen equipment Portable suctioning machines Aerosol equipment and nebulizers Incentive spirometers Home ventilators Tracheostomy tubes and collars COPD Triad of diseases Emphysema, chronic bronchitis, asthma Outflow obstructive diseases impending the exhalation of air from lungs Minimal lung capacity Inability to meet normal metabolic demands Decreased patient activity with increase use of 02 Increase C02 and decrease oxygenation Bronchitis/Emphysema Bronchitis Chronic excessive production of mucus Narrowing bronchial passages restricting air flow Large, obese patients (blue bloater) Emphysema Enlargement and stiffening of alveoli and acenus Loss of elasticity and compliance requires a higher pressure in lungs to facilitate gas exchange at alveolar level Patients have increased A/P dimensions (increased air retention and decreased outflow Thin patients due to increase caloric output Acute Exacerbation Patients have difficult compensatory mechanisms Signs and symptoms Wheezing, diminished breath sounds, use of accessory muscles, retractions, tripod positioning, inability to speak or form sentences Home health care treatments Oxygen, nebulized aerosol treatments Ventilator: PEEP (via ETT), CPAP, BiPAP (mask therapy) Treatment Intervention Oxygenation and ventilation Nebulized beta-2 agonists Nebulized anti-cholinergics IV corticosteriods Asthma Reactive and reversible airway disease seen at any age Characterized by bronchospasm and swelling of mucus membranes Signs and symptoms of acute attack Home therapy O2, oral medications, variety of nebulizers and/or inhalants Treatment Oxygenation and ventilation, beta agonists, anticholinergics, corticosteriods Avoidance or elimination of reactants that trigger problem Cystic Fibrosis Generic disorder usually recognized in childhood Terminal disease Characterized by chronic overproduction of mucus, inflammation of small airways and hyperinflation of alveoli, chronic infections, and erosion of the pulmonary blood vessels secondary to infection Exocrine disease causing other abnormalities GI disturbances, pancreatic disorders, glucose intolerance Home Health Treatment Postural drainage of mucus Chest physiotherapy Mechanical vibrators to facilitate breakage of secretions Medications aimed at mucus reduction and control of systemic bacterial infections Bronchopulmonary Dysplasia Primarily affects infants of low birth weight Characterized by ongoing need for mechanical ventilation in newborns Infants fail to wean from mandatory ventilation or oxygenation Increased risk of respiratory infection Management EMS Oxygenation and oximetric monitoring Neonatal transport to appropriate facility Home health Intermittent mandatory ventilation (IMV) Pulmonary congestion and edema Limit fluid intake Management/Summary Improving airway patency Improve ventilation Improve oxygenation Psychological support Communication with the intubated patient Communication using a “talking trach” Neuromuscular Degenerative Diseases Affect respiratory action through degeneration of muscles used for breathing As disease progresses and involves more muscle groups, inability to ambulate increases infections and rapid decline of patients Neuromuscular Diseases Muscular Dystrophy Genetically inherited disorder causing a defect in the intracellular metabolism of muscle cells Leads to degeneration and atrophy of muscles which are replaced by fatty and connective tissues No cure to date EMS involvement: respiratory failure, accidental injuries usually related to falls Neuromuscular Diseases Poliomyelitis Infectious disease rarely seen today because of vaccine Destroys motor neurons leading to muscular atrophy, weakness, and paralysis Children often suffer crippling effects Neuromuscular Diseases Guillain-Barre Syndrome Autoimmune response to a viral infection Usually preceded by a febrile episode with a respiratory or GI infection Characterized by muscle weakness leading to paralysis caused by nerve demylenation Usually begins in distal extremities and moves proximally No cognitive or CNS involvement Neuromuscular Diseases Myasthenia Gravis Rare disease that affects the neuronal junction Due to a breakdown in acetylcholine receptors, nerve impulses are delayed Characterized by muscle weakness proximal to the body versus distal No cure to date Sleep Apnea Complex condition not fully understood by experts Characterized by long pauses in respiratory cycle that can be caused by a relaxation of the pharynx or lack of respiratory drive Can result in hypertension, arrhythmias, and chronic fatigue Sleep Apnea Symptomology Muscles of airway become more relaxed as mind falls deeper into sleep Leads to snoring, and in some cases, blockage of airway Decreased 02 levels cause a partial awakening of the patient Breathing then resumes and patient returns to sleep, often with no memory of the event Repeated over and over, interruptions destroy normal sleep patterns and the patient spends much of the sleeping in a hypoxic state Sleep Apnea General treatment Surgical alteration of the airway Medications Prescribed weight loss Avoidance of any CNS depressants (alcohol) Use of CPAP ventilator Medical Therapy Found in the Home Setting Home oxygen therapy Artificial airways/tracheostomies Vascular access devices Home Oxygen Therapy Many advantages for home care patients Easy to use Tolerated well by most patients Add to quality of a patient’s life Prevents hypoxia that may result in permanent cognitive damage or degeneration Oxygen Systems Artificial Airways/Tracheostomies Used for patients with long-term upper airway problems Tracheostomy may be temporary or permanent Technique is used on patients who require artificial ventilation for long periods of time Patients with damage to larynx, epiglottis, or upper airway structures from surgery or trauma Artificial Airway Tracheostomy consists: Surgical opening (stoma) Outer cannula Keeps stoma open Held in place by twill tape or velcro strap Inner cannula Similar to a mini ET tube Slides down into trachea a few inches Distal low pressure cuff to hold in place and provide a good seal Tracheotomy tubes Top: Plastic tube Bottom: metal tube with inner cannula Artificial Airways Speech Artificial larynx Looks like a small flash light Creates an electronic vibration by pressing the device up against the neck and by patient changing shape of his/her mouth Routine Care of Tracheostomy Keep stoma clean and dry Prevent pulmonary infections Periodic changing of the outer cannula Changing and cleaning the inner cannnula from every few weeks to every months, depending on the patient For ventilator patients, routine changing of the ventilator hose connections Frequent suctioning, due to increased secretion Common Complications of Tracheostomy Patients Blockage of the airway by mucus and/or dislodged cannula Patient coughing to clear and suctioning Patient movement and child growth Infection of the stoma Drying of tracheal mucus leading to crusting or bleeding Tracheal erosion from an over-inflated cuff Tracheal necrosis Management/Ventilation Management Oxygenation and ventilation Sterile suctioning of the stoma/trachea with an endotracheal suction catheter Cannula obstruction Deflate cuff and remove Stoma intubation Remove inner cannula Use appropriate sized tube size and advance tube 1-2cm inside trachea Attach end tidal CO2 device and monitor with pulse oximetry Home Ventilation Types of ventilators Positive pressure Negative pressure Provision for ventilation Volume cycled ventilation Historical standard for ventilators Used to support multiple forms of respiratory failure Home Ventilation Positive pressure ventilators (PPV) Recommended for acute respiratory failure Push air into lungs through a mask, nasal mask, or tracheostomy Features Variations: tidal volume respiratory rate flow rate pressure Home Ventilation Negative pressure ventilators Imitate normal breathing process Apply negative pressure to the chest (pull chest allowing it to expand) Allows air to flow into lungs Patients usually use this form of device at night Iron lung is an old example PEEP/CPAP/BiPAP Three ventilator options Add pressures at various times during respiratory cycle May be used on a full-time or part-time basis Always possibility of pneumothorax due to increased pulmonary pressure PEEP Positive end expiratory pressure Used to maintain inflation of alveoli Functions by providing a little back pressure at the end of expiration Uses Premature infants with insufficient surfactant Adults with surfactant washout from PE, ARDS, near drowning COPD Emphysema patients require higher diffusion pressures for gas exchange CPAP Continuous positive airway pressure Used to keep pharyngeal structures from collapsing at end of a breath Often prescribed for sleep apnea Most patients use nasal CPAP Patients must keep mouth closed Idea behind CPAP is the same a PEEP CPAP is delivered with a mask while PEEP is delivered via ETT Ventilation/CPAP-Nasal Figure 6-7 BIPAP Bilevel positive airway pressure Provides two levels of pressure Inspiration Expiration Used for patients who require higher levels of pressure than CPAP Assessment Findings Work of breathing Tidal volume Peak flow Oxygen saturation Capnography Breath sounds Vascular Access Devices Approximately 500,000 long term therapy catheters inserted each year VAD’s are used to provide parenteral treatment on a long term basis Used for Chemotherapy Hemodialysis Peritoneal dialysis Total parenteral nutrition Antibiotic therapy Vascular Access Devices Hickman, Broviac, Groshong Peripherally inserted central catheters Surgically implanted medication delivery systems Dialysis shunts Hickman, Broviac, or Groshong Catheters Single, double, triple lumen catheters inserted into a central vein Subclavian vein most common All have an external port that look like an IV port External hub of the catheter is sutured into skin and has a cuff that promotes fibrous in-growth Anchors catheter to body and prevents infection from traveling down catheter Care of device includes: cleanliness and administration of anticoagulant therapy Peripherally Inserted Central Catheters PICC lines are most commonly inserted into median cubital vein in the ACF Catheter is threaded from insertion site into central venous circulation PICC lines are inserted under fluoroscopy Surgically Implanted Medication Delivery Systems Port-a-cath or Medi-port Infusion port is implanted completely below the skin Disc shaped devices that have a diaphragm that requires a specially shaped needle (Huber needle) Typically implanted in upper chest Dialysis Shunt Used for patients undergoing hemodialysis to filter their blood Types of shunts AV shunt Loop connecting an artery and vein, most common in distal arm where dialysis apparatus evacuates and returns blood Fistula Connects artery and vein creating an artificially large blood vessel for access AV Shunt VAD Complications Obstruction Thrombus Embolus (air embolus) Catheter kinking Catheter tip embolus Inactivity increases risk of clots Infection Hemorrhage Cardiac Conditions (Home Health) Post MI recovery Post cardiac surgery Heart transplant CHF Hypertension Implanted pacemaker Atherosclerosis Congenital malformation (pediatric) GI/GU Crisis Devices to support GI/GU function are common. Be familiar with the various devices and their complications. GI/GU Devices Urinary catheters or urostomies Surgical diversion of the urinary tract to a stoma, or hole in the abdominal wall Indwelling nutritional support device (peg tube, G-tube) Colostomies NG tube External Urinary Catheter (Texas Sheath) Figure 6-9 Foley Catheter (Indwelling Catheter) Figure 6-10 Urinary Device Complications Infection or device malfunction Catheter device provides a pathway for infectious entry Foul smelling urine Discolored (cloudy) urine Blood tinged urine Systemic infection (fever) Redness, swelling of abdominal wall site with urostomies Device malfunction: accidental placement, obstruction, balloon ruptures Gastrointestinal Devices Nasogastric tubes Decompress gastric contents Lavage GI system Short term use Feeding tubes Rest on the duodenum or jejunum Weighted with steel filament to aid insertion and passage through pyloric sphincter Percutaneous endoscopic gastrostomy (PEG) Via abdominal wall Long term nutritional support Nasogastric Feeding Gastrostomy (PEG) Figure 6-12 Colostomy Opening of a portion of the large intestines (colon) through the abdominal wall, allowing feces to be collected outside the body Temporary or permanent Indications CA of bowel Diverticulitis Crohn’s disease Trauma Colostomy Figure 6-13 Assessment Findings Abdominal pain and distention Bowel sounds Palpation of bladder Color, character, amount of urine Acute Infections Increased rate of infections in the elderly, chronically ill and homebound Decreased ability to perceive pain or perform self-care in many homebound populations Pathophysiology Increased risk of respiratory infection in the immunocompromised patient Poor peripheral perfusion results in decreased healing and increased peripheral infections Sedentary existence leads to skin breakdown and peripheral infections Pathophysiology Percutaneous and implanted medical devices increase risk for infections and sepsis Patients discharged to home with open wounds and incisions Chronic diseases may further impair healing Poor nutrition, hygiene or ability to care for self impact infection rates Maternal & Newborn Care Many women who deliver their babies in the hospital will be discharged in 24 hours or less. ALS providers may be called upon to assist new parents in caring for newborns or post-partum complications. Post-partum bleeding and embolus are common complications Management includes: Massage of uterus Administration of fluids Administration of pitocin Rapid transport, if necessary Postpartum Depression “Let down” feeling experienced during the period following birth Occurs in 70%-80% of mothers Women have difficulty caring for both themselves and newborn Be sensitive to needs and non-urgent responses Infants and Children with Special Needs Many different types of children Premature babies Lung disease Heart diseases Neurological diseases Chronic diseases Altered functions from birth Infants and Children with Special Needs Common home-care devices Tracheostomy tubes Apnea monitors Home artificial ventilators Central intravenous lines Gastric feeding and gastrostomy tubes Shunts Common Infant/Child Complications Signs/symptoms of cardiorespiratory insufficiency include: Cyanosis Bradycardia (<100 BPM) Rales Respiratory Distress Hospice More than 2250 hospices provide support for the terminally ill and families. The goal of hospice care is to provide palliative or comfort care rather than curative care. Hospice Hospice Palliative care Comfort care Hospice care DNR Medical direction considerations Pain control in the terminal patient Common Hospice Diseases Congestive heart failure Cystic fibrosis COPD AIDS Alzhemier’s Cancer HIV Children Figure 6-14 Summary Home Health Care Home Care Providers Home Care Pathologies ALS Support for Home Care Patients Hospice