Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Congenital heart defect wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Atrial septal defect wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
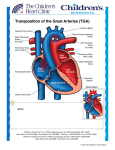
Dextro-Transposition of the great arteries wikipedia , lookup
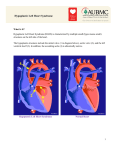
RSPT 2353 – Neonatal/Pediatric Cardiopulmonary Care Congenital Disorders Lecture Notes Reference & Reading: Czverinske Chapter 29 & 31 I. Congenital Anomalies – Pulmonary involvement a. Diaphragmatic Hernia More common on left than right Symptoms: 1. Polyhydramnios 2. Cyanosis, respiratory distress 3. Bowel sounds in chest 4. Flat abdomen, scaphoid chest Diagnosis 1. Usually prenatal 2. CXR – bowel in chest 3. Depending on degree of herniation there may be a presence of lung hypoplasia Treatment 1. Immediate intubation at birth 2. Placement of NG or OG tube 3. Ventilate patient as necessary 4. UAC & UVC need to be placed b. Tracheoesophageal Anomalies (TE fistula) – Atresia of the upper esophagus, usually includes a fistula between the lower esophageal tube & trachea (most common Fig 29-2 (A)). Diagnosis - Suspicions usually arise with: 1. Accumulation of oral secretions 2. Sporadic or continuous respiratory distress 3. Repeated regurgitation Treatment – surgical repair 1. Keep bed at 30 degree angle 2. Post-op c. Omphalocele Diagnosis – prenatal Treatment d. Gastroschisis Diagnosis – prenatal Treatment – 1. Contents during delivery are placed in a protective sac 2. Pedi surgeons will place a silo on defect and reduce until patient is ready for surgery 3. Patient may or may not require respiratory intervention 4. Post-op II. Congenital anomalies – Cardiac defects 1 a. Affect about 1 in 100 deliveries. Signs, Symptoms and treatment depend on the type & degree of defect. b. Patent Ductus Arteriosus (PDA) Pathophysiology – 1. Pulmonary edema 2. With amount of blood shunting through PDA hypoperfusion occurs to all postductal organsNEC, and other disorders 3. Keeping the PDA can be important in some heart defects Diagnosis 1. Loud grade I or II murmur 2. Echocardiogram with color mapping can indicate presence and direction of blood flow 3. Pre/post ductal: a. R-to-L b. L-to-R Treatment 1. Usually self resolve 2. Indomethacin 3. Surgical ligation c. Atrial Septal Defect (ASD) Diagnosis – usually undected ASD is desirable in certain situations d. Ventricular Septal Defect (VSD) Diagnosed Treatment is usually withheld unless: 1. Failure to thrive 2. CHF that doesn’t respond to tx 2 e. Tetralogy of Fallot 4 defects: 1. VSD 2. overriding aorta 3. hypertrophy of the RV 4. obstruction to flow through PA Cyanosis is a result of blood flow through PA CXR Diagnosed by ultrasound Cardiac Cathetarization Treatment f. Transposition of the Great Vessels (TGV) aka TGA Aorta arises from R ventricle, PA arises from L ventricle Shunt dependant Mixing of blood occurs via an ASD, PDA or VSD Pt often show signs of CHF Diagnosis Treatment 1. Balloon septostomy 2. dissection of vessels and placement in correct ventricle 3 g. Coarctation of Aorta Constriction of aorta restricts blood flow Signs are related to CO Diagnosis 1. If suspected 2. Definitive Treatment: 1. Surgical repair 2. PGE h. Anomalous Venous Return (TAPVR) Return of oxygenated blood to R atrium instead of left ASD must be present to survive Diagnosis: cardiac cathetarization Treatment: 1. Immediate cardiac catheterization with balloon septostomy 2. Surgical repair involves placement of pulmonary veins into left atria 4 i. Truncus Arteriosus – One large vessel arises from both R & L ventricles with a large VSD Cyanosis usually present, depends on degree of pulmonary perfusion Diagnosis Treatment j. Hypoplastic Heart (Left or Right) Right hypoplastic heart 1. non PDA dependent, avoid fluid overload 2. better survival Left hypoplastic heart – involves several anomolies 1. coarc, hypoplastic L ventricle, aortic and/or mitral valve stenosis or atresia 2. Duct dependant 3. Treatment: a. 2 stage surgical repair: Norwood, Glenn, Fontan b. Heart transplant 5