Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
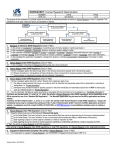
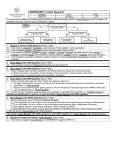
Regulatory Requirements for Drug Eluting Balloons Ashley Boam, MSBE for: Andrew Farb, M.D. Interventional Cardiology Devices Branch Division of Cardiovascular Devices U.S. FDA/CDRH THE DRUG ELUTING BALLOON SYMPOSIUM CRT 2010 Washington, DC February 22, 2010 DHHS/FDA DISCLOSURES Ashley Boam I have no real or apparent conflicts of interest to report. Components of a Drug-Eluting Balloon (DEB) Combination Product PTCA Balloon Coating Delivery System Therapeutic Agent DEB Regulatory Submission Pathway For a DEB identified as both a dilatation catheter and drug-delivery device – Otherwise primarily a drug delivery device – Different regulatory path Investigational Device Exemption (IDE) – Significant risk product (Class III) – Required to conduct clinical trial in the US Premarket Approval Application (PMA) – Comprehensive review of bench testing, animal studies, & all clinical data – Establish a reasonable assurance of safety and effectiveness DHHS/FDA DEB Preclinical Testing Objectives Complete characterization of the finished sterilized product – Coating/drug loading characteristics – drug and coating content, coating integrity & uniformity Particularly with varying balloon sizes – In vitro/in vivo PK studies Serum and tissue levels Adequate early time point sampling – Methods and specifications to allow stability testing Adequate bench and animal studies to assess safety prior to human studies DHHS/FDA Bench Testing See FDA Guidance documents – For PTCA component: Draft Class II Special Controls Guidance for PTCA Catheters – For Drug component: Draft Coronary DES Guidance Additional specific bench tests to support indication (e.g., ISR, coronary vs. peripheral arterial beds, small vessels) Testing to evaluate expected worst case clinical use and encompass product matrix Coating integrity and particulate testing are necessary DHHS/FDA Preclinical testing of PTCA Balloons (Including DEBs) – Biocompatibility Entire device without drug coating Balloon + drug coating material separately If drug retained in tissue>30 days, implant biocompatibility testing needed Cytotoxicity Sensitization Hemocompatibility Material-mediated pyrogenicity DHHS/FDA Preclinical Functional Testing of PTCA Balloons Dimensional Verification Balloon Rated Burst Pressure Balloon Compliance (Diameter vs. Pressure) Catheter Bond Strength Tip Pull Test Flexibility and Kink Test Coating Integrity Balloon Preparation, Deployment and Retraction Balloon Fatigue (Repeat Balloon Inflations) Balloon Inflation and Deflation Time Torque Strength Radiopacity Particulate Evaluation Other required information: Sterilization and shelf life testing (both functional testing and stability) DHHS/FDA Drug substance on DEB See DES Draft Guidance: http://www.fda.gov/downloads/Drugs/GuidanceCo mplianceRegulatoryInformation/Guidances/UCM07 2193.pdf DHHS/FDA Animal Studies-Safety High dose density (greater than DES) and drug delivery could lead to local toxicity Safety/Healing – – – – – Thrombus deposition Inflammation Re-endothelialization: SEM Edge effects Remodeling: Positive & negative Safety margin overdose studies Assessment of downstream myocardial pathology DHHS/FDA Animal Studies-Effectiveness Inhibition of neointimal proliferation Proof of principle vs. a stent (or POBA if appropriate) control group – Normal coronary arteries – In-stent restenosis disease model may be particularly useful for safety & effectiveness considerations, drug delivery, & PK Morphology similar to human ISR Optional: Vasomotor function DHHS/FDA Clinical Trials Feasibility/FIM trial(s) – Initial assessment of device performance and safety and effectiveness Pivotal trial for coronary indication – RCT recommended for initial FDA approval – Target lesion failure (TLF) rate primary endpoint – Superiority or non-inferiority to approved stent DHHS/FDA Indications for Use and Control Groups De novo CAD control – DES (or BMS in patients not able or unlikely to comply with prolonged DAPT use) Coronary BMS restenosis control – Approved DES for ISR (TAXUS Express or Liberté) If non-inferiority design, chose acceptable delta that also maintains headroom vs. brachytherapy historical data Peripheral artery control – Approved stents or POBA Depends on standard of care and approval status tailored to arterial target (e.g., SFA, tibial, etc.) DHHS/FDA Pivotal Study Duration Science-Based Approach Study duration depends on clinical indication and vascular biology – For ISR, restenosis a function of neointimal thickening – For de novo CAD treatment, restenosis post-POBA a function of neointimal proliferation + adventitial constrictive remodeling Preclinical animal & PK studies help define when healing complete and drug eliminated from periarterial tissues Candidate antiproliferative drugs on DEB delay healing For coronary ISR indication, 9 months study may be acceptable For de novo CAD treatment, 12 months probably indicated DHHS/FDA Other Clinical Trial Considerations Describe pre-dilatation procedure (e.g., undersized balloon) Clarify single use or multiple use of individual DEB Procedural results – Acute device success rate important Achievement of acceptable post-deployment stenosis with the test device alone Frequent use of adjunctive stents may confound results – Procedure success: Includes DEB plus adjunctive procedures/ devices – Clinical success: Device success without in-hospital MACE DHHS/FDA Clinical Imaging Cohort Measurements – In-lesion and in-segment MLD, late lumen loss, & %diameter stenosis – Neointimal area and volume – Edge effects & positive and negative remodeling Angio/IVUS assessment more challenging to identify treatment site post-DEB treatment – Blinding issues vs. a stent – Approaches to minimize bias Other potential target – Vasomotion DHHS/FDA Antiplatelet Therapy Propose and justify duration of thienopyridine use post-DEB use Attempt to limit confounders – Patients already on extended thienopyridines – Patients treated with DES on second coronary lesion at time of index procedure DHHS/FDA DEB Clinical Program Considerations Need adequate number of patients treated to detect uncommon but important safety events – Not all patients need to be part of a randomized trial – Can use multiple trials (both US and OUS) Patient clinical follow-up through 4-5 years – Assess rates of coronary thrombosis over time Track outcomes post-DEB restenosis treatment Plan for post-approval study – Real world use beyond labeled indication – Evaluate rates of ST, and CV death + MI DHHS/FDA Regulatory Paths for Drug-Eluting Balloons Discussions with FDA early in DEB program development recommended – Utilize the pre-IDE process Satisfactory data for a coronary indication does not automatically equal satisfactory data for a peripheral indication – Differences in drug content, vascular response, downstream territories DHHS/FDA Contact Information Interventional Cardiology Devices Branch 301-796-6343 [email protected] [email protected] DHHS/FDA