Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
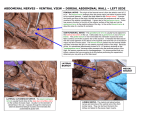
Revisiting anterior leg anatomy and analgesia after total knee replacement P.J. Cowlishaw P. Kotze Optimal anaesthesia and analgesia for total knee arthroplasty (TKA) presents a unique challenge for Anaesthetists. Elderly patients with significant co-morbity are subjected to major tissue trauma resulting in severe prolonged acute pain and systemic stress response. Successful surgical outcome is reliant on safe and early patient mobilisation. Common obstacles in preventing this are pain, muscle weakness, sedation and confusion. These can be minimised by using an opiate sparing multimodal anaesthetic and analgesic regimen utilising continuous regional anaesthesia. Publications investigating the best regimen have filled the orthopaedic and anaesthetic journals over the last couple of decades. It remains a huge source of debate. Many regional anaesthesia techniques can be used to achieve neural blockade from the central nervous system (epidural), to the major peripheral nerves (sciatic, femoral and obturator nerve blocks) through to the terminal branches and plexuses (local infiltration at the surgical site). There are benefits and risks and protagonists and antagonists for all. A thorough appreciation and understanding of the neuroanatomy is paramount. The knee is innervated by three nerves:- femoral, obturator and sciatic. Anatomy of the sciatic nerve is not included in this review. The femoral nerve arises from the dorsal divisions of the second, third and fourth lumbar nerves. The nerve runs in the muscle fibres of psoas and emerges on its lateral border. From here it courses between iliacus and psoas below the iliacus fascia. After passing under the inguinal ligament it immediately branches in to the anterior and posterior division. Within the femoral triangle the anterior division splits in to the a) intermediate and b) medial cutaneous femoral nerves and two muscular branches which supply pectineus and sartorius. a) The intermediate (middle) femoral cutaneous nerve pierces the fascia lata forming the roof of the femoral triangle and descends superficially to supply the skin of the anterior thigh. b) The medial (internal) femoral cutaneous nerve divides high in the thigh in front of the femoral artery. The anterior branch runs deep on sartorius and pierces fascia lata in the mid-thigh. Here it divides in two, one innervates the medial side of the knee and the other the lateral side of patella (communicating with the infrapatella branch of saphenous nerve). The posterior branch descends along medial side of sartorius giving off several cutaneous branches. The posterior division supplies the quadriceps and knee joint and forms the saphenous nerve. Branches to rectus femoris and vastus lateralis leave with or above the lateral femoral circumflex artery within the femoral triangle. The vastus medialis branch descends further down the thigh with the saphenous nerve and femoral artery in the adductor canal. This nerve divides further and usually has a terminal branch which supplies the knee. The saphenous nerve lies first lateral, then anterior and eventually medial to the femoral artery deep to the sartorius muscle in the adductor canal. It emerges between the tendons of gracilis and sartorius. At the middle of the thigh it gives off a branch which forms part of the subsartorial plexus. On the medial side of the knee a large branch leaves innervating the patella forming part of the infrapatella plexus. Terminal branches of the obturator often form part of this plexus. The obturator nerve originates from the ventral division of the second, third and fourth lumbar nerves. It also descends through the fibres of psoas and emerges on the medial border near the pelvic brim. It enters the thigh through the obturator foramen and divides into anterior and posterior branches. The anterior branch innervates the adductor longus and pectineus. It communicates with the anterior cutaneous and saphenous nerve at the lower border of adductor longus contributing to the subsartorial plexus. The posterior branch supplies the adductor brevis and magnus and usually gives off an articular knee filament. This is sometimes absent but usually perforates the adductor magnus and passes through the opening which transmits the femoral artery. Research suggests that continuous blockade of the femoral nerve provides excellent analgesia for knee replacement surgery with or without the addition of continuous sciatic blockade1,2. The femoral nerve innervates many of the hip flexors (iliacus, rectus femoris, pectineus and Sartorius) and all the knee extensors (quadriceps). Dense motor blockade inhibits early mobilisation and may increase the risk of falls post TKA surgery 3,4. Selective sensory and articular blockade of the femoral nerve could provide optimal conditions for patient satisfaction and surgical outcome. Recent clinical studies have investigated blockade of the femoral nerve in the adductor canal. These studies have shown that ‘adductor canal blocks’ provide similar analgesia to traditional femoral nerve blockade with preservation of quadriceps function: Thus facilitating early and safe mobilisation.5-7 Using MRI imaging and cadaver dissection we set out to find an anatomical explanation for these clinical findings. In a pilot cadaver study we inserted catheters at the proximal start of the adductor canal using an in-plane ultrasound guided technique. The entry point of the catheter was 10-13 cm below the midpoint of the inguinal ligament. 20 mls of 0.25% Aniline blue (2.5 g in 1000 ml Saline (0.9%) = 2.5 mg/ml = 25%) was injected through the catheter. Careful dissection revealed that the dye had spread down the adductor canal to the adductor hiatus in all three cadavers. (figure 1). dye Figure 1 Dissection showing the muscular layer of the thigh form of the left leg. Dye are noted on the facia of the subsartorial canal form the apex of the femoral triangle and approximating the adductor hiatus. In all 3 cadaver dissections there was no spread of dye in to the femoral triangle with cephalad spread limited to 1-2 cm above the catheter. The fascia enveloping the femoral triangle was thicker and less compliant. Dye did not stain the motor nerves to sartorius, vastus lateralis, intermedius and rectus femoris. (figure 2) Figure 2 Detailed dissection of the right femoral triangle showing the unstained femoral nerve as it exits the femoral canal and branching 2cm distally. Key: 1 Femoral nerve, 2 M. Sartorius, 3 Motor nerve prior to split to quadriceps muscle, 4. Hip articular branch 5. Femoral vessel MRI and ultrasound imaging was also performed on a patient undergoing total knee arthroplasty. Figure 3 shows the ultrasound image and the catheter in situ after the femoral artery has branched into profunda, superficial and lateral circumflex. Figure 3 Catheter inserted between sartorius and rectus femoris distal to the splitting of the femoral artery Figure 4 illustrates the high signal density (white) of the local anaesthetic spreading under the sartorius muscle lateral to the femoral vessels. Figure 5 is a reconstructed coronal view demonstrating the high signal density of local anaesthetic spreading distally in the adductor canal but not cephalad. Figure 4 MRI image of catheter and spread of local anaesthetic in the sub-sartorial space Figure 5 Reconstructed coronal MRI image of thigh This anatomical evidence provides an explanation to why continuous adductor canal blocks can provide excellent analgesia with quadriceps sparing. In summary cutaneous analgesia is achieved with blockade of the saphenous, medial cutaneous nerve and sensory branches of the anterior obturator nerve. Knee analgesia is also provided from blockade of the articular branches of the posterior femoral nerve which lie in the adductor canal and possibly an articular branch of the posterior obturator nerve. Innervation to sartorius, vastus lateralis, intermedius and rectus femoris appears to be spared. Published descriptions of the adductor canal block describe an in plane ultrasound guided injection at a mid-thigh level when neurovascular bundle is tightly surrounded by sartorius, vastus medialis and adductor longus. Our needle entry site is different: a lateral in plane ultrasound guided approach 10-12cm below the inguinal ligament. The needle endpoint is inferior to sartorius, medial to rectus femoris and lateral or inferior to the superficial femoral artery. This catheter entry site is usually proximal to the tourniquet and away from the surgical site and dressings. It is well below the inguinal crease facilitating access and minimising infection risk. Further clinical trials are required to optimise local anaesthetic infusion regimes and catheter techniques. 1. Cowlishaw PJ, Scott DM, Barrington MJ. The role of regional anaesthesia techniques in the management of acute pain. Anaesth Intensive Care 2012;40:33-45. 2. Wegener JT, Van Ooij B, Van Dijk CN, Hollmann MW, Preckel B, Stevens MF. Value of single-injection or continuous sciatic nerve block in addition to a continuous femoral nerve block in patients undergoing total knee arthroplasty: A prospective, randomized, controlled trial. Regional Anesthesia and Pain Medicine 2011;36 (5):481-8. 3. Johnson RL, Kopp SL, Hebl JR, Erwin PJ, Mantilla CB. Falls and major orthopaedic surgery with peripheral nerve blockade: a systematic review and metaanalysis. Br J Anaesth 2013;110:518-28. 4. Ilfeld BM, Duke KB, Donohue MC. The association between lower extremity continuous peripheral nerve blocks and patient falls after knee and hip arthroplasty. Anesth Analg 2010;111:1552-4. 5. Kwofie MK, Shastri UD, Gadsden JC, et al. The effects of ultrasound-guided adductor canal block versus femoral nerve block on quadriceps strength and fall risk: a blinded, randomized trial of volunteers. Reg Anesth Pain Med 2013;38:321-5. 6. Hanson NA, Allen CJ, Hostetter LS, et al. Continuous ultrasound-guided adductor canal block for total knee arthroplasty: a randomized, double-blind trial. Anesth Analg 2014;118:1370-7. 7. Jenstrup MT, Jaeger P, Lund J, et al. Effects of adductor-canal-blockade on pain and ambulation after total knee arthroplasty: a randomized study. Acta Anaesthesiol Scand 2012;56:357-64.