Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
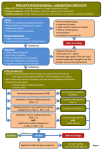
Overactive bladder: clinical evaluation and medical treatment Philip E.V. Van Kerrebroeck, MD, PhD, MMSc Professor of Urology Maastricht University Medical Centre the Netherlands Overactive bladder definitions Urgency1,2 Sudden compelling desire to pass urine that is difficult to defer Frequency1,2 Patient considers that he/she voids too often by day Normal is < 8 times per 24 hours Nocturia1,2 Waking to urinate during sleep hours Considered a clinical problem if frequency is greater than twice a night Urgency urinary incontinence (UUI)1 Involuntary leakage accompanied by or immediately preceded by urgency OAB “wet”1,2 OAB with UUI OAB “dry”2 OAB without UUI Warning time3 Time from first sensation of urgency to voiding 1Abrams P, et al. Neurourol Urodyn. 2002;21:167-178. AJ, et al. J Urol. 2006;175(3 pt 2):S5-S10. 3Zinner N, et al. Int J Clin Pract. 2006;60:119-126. 2Wein Overactive bladder syndrome (OAB) Urgency, with or without urgency incontinence, usually with increased day time frequency and nocturia, if there is no proven infection or other obvious pathology OAB Wet Abrams et al, Neurourol Urodyn, 2002 Abrams et al, Neurourol Urodyn, 2009 OAB Dry Prevalence of OAB in Europe & the US EU SIFO Study US NOBLE Study Milsom I et al. 2001 Stewart et al. 2001 40 Prevalence (%) 45 40 Men 35 35 Women 30 30 Men Women 25 25 20 20 15 15 10 10 5 5 0 0 40–44 45–49 50–54 55–59 60–64 65–69 70–74 Age (years) 75+ 18-24 25-34 35-44 45-54 Age (years) 17% of the adult population have symptoms of OAB Prevalence of OAB increases with age Similar prevalence among men and women (women may present more) 55-64 65-74 75+ Prevalence of OAB by age and gender 25 22.9 20 Prevalence, % 20.6 16.0 15.9 15 13.3 10.5 10 9.4 10.7 10.9 10.0 8.6 5 8.2 8.1 7.5 5.1 0 Age, years Irwin DE, Milsom I, Hunskaar S et al Eur Urol 2006; 50: 1306-15 Men 14.5 Women 10.3 8.6 9.5 15.4 Diagnosis: Initial Evaluation Diagnosis based on presenting symptomology and does not require invasive tests: Examine potential risk factors Thorough history Nature of symptoms Physical examination Urinalysis Bladder diary Medications influencing bladder function Differential diagnosis of OAB 6 Diagnosis: General OAB Risk Factors Smoking Relationship exists between smoking and UI Partly due to nicotine’s possible effect on bladder contractility Chronic/frequent coughing can lead to damaged urethral and vaginal supports, as well as perineal nerve damage Obesity Increased pressure on bladder Greater urethral mobility Possible impaired blood flow or bladder innervation 7 Diagnosis: OAB Risk Factors for Women Pregnancy and Childbirth Can flatten, stretch, and weaken many of the pelvic floor muscles Evidence that # of vaginal births related to increased OAB risk and incontinence later in life Menopause Weakens urethra’s ability to maintain tight seal Lack of estrogen weakens detrusor, and can cause the urethra to open unexpectedly during physical activity Pelvic surgery Weakens and damage pelvic floor muscles Women undergone removal of uterus have 40% increased risk of UI 8 Diagnosis: OAB Risk Factors for Men Benign Prostatic Hyperplasia Frequent cause of UI Detrusor contracting strongly and frequently to compensate for reduced urinary flow due to urethral obstruction Prostate/Bladder Surgery 2 to 3 times more likely to experience UI than those without the surgery 9 Diagnosis: Patient History How long? How old when started? How much (volume)? Degree of bother? Characteristics of leakage? Activity related? Day and night, wet pads at night = instability Urgency? suppressible = probably SUI not suppressible (urgency incontinence) = overactivity Other: fluid intake, UTI’s, pain, hematuria, LE swelling, medications 10 Diagnosis: Nature of OAB Symptoms Questions to Consider Do you frequently limit your fluid intake or map out restrooms when you are away from home? Do you urinate more than 8 times in a 24-hour period? Do you frequently get up 2 or more times at night to go to the bathroom? Do you have uncontrollable urges to urinate, resulting in wetting accidents? Do you use pads to protect your clothes? Are you bothered or concerned about bladder control? 11 Diagnosis: Patient Physical Examination Abdomen Masses: palpable bladder, etc. Abdominal masses f.e. palpable bladder Pelvis/perineum External genitalia • Prolapse (assoc. 50% of SUI patients) • Malignancy, fistula Rectal tone, masses, teach Kegels during exam Prostate Neurological (reflexes, LE’s, sensory, motor) 12 Diagnosis: Bladder Diary 13 Diagnosis: Urinary Tract Infection (= different from OAB!) UTI’s: Cystitis, Urethritis Timing of the onset of symptoms is usually very different UTI being acute and OAB being chronic Pain with urination (dysuria), costovertebral angle tenderness/pain and possibly elevated temperature are features of UTI’s not usually associated with OAB UTIs may also occur in individuals with OAB usually present with an exacerbation of their OAB symptoms and dysuria. 14 Diagnosis: Bladder cancer ( = different from OAB !!) Haematuria, in the presence of bladder symptoms, is the defining diagnostic feature of bladder cancer haematuria in the presence of OAB symptoms must be investigated further to rule out pathology or malignancy. 15 QoL: Physical Impact of OAB Increased risk of falls and fractures from rushing to the toilet Higher rate with nocturia (night time visibility) Elderly population most susceptible Experience more urinary tract infections (UTIs) and skin infections Sleep disturbances are reported by many patients with OAB correlated with poor health 16 Diagnosis: Key Consideration Overactive Bladder diagnosed if there is no proven infection, metabolic disorder, or other obvious pathology OAB cannot be diagnosed without the complaint of urgency, but can be without the complaint of incontinence 17 QoL: Emotional Impact of OAB Manage fear of incontinence and urgency episodes by developing coping mechanisms mapping toilet locations, voiding frequently, use of incontinence pads and limiting fluid intake Common daily activities (e.g., shopping, travel, physical activity) and personal relationships are often avoided due to fear of embarrassment Patients often express loss of self-esteem and depression. depression associated with OAB is the same as other chronic conditions: diabetes, rheumatoid arthritis, and hypertension 18 Patient Misconceptions and Fears “Part of normal aging or everyday life” “Not severe or frequent enough to treat” “Too embarrassing to discuss” “Treatment won't help” 19 Which Patient - Which Treatment Diagnosis of the problem Understanding the major component SUI associated with exertion onset in reproductive years Urgency incontinence associated with urgency in post menopausal women Mixed incontinence affects approximately 30% Having a clear picture of the patient’s goals from treatment 20 Non-invasive treatments for OAB Lifestyle modification Behavioural intervention Electrical stimulation Acupuncture Hypnotherapy Drugs Lifestyle intervention fluid intake, caffeine, tea, Coke, wt reduction Significant reduction in U, F, and N with 25% reduction in fluid intake. Increasing fluid intake worsened F Hashim et al, 2008 High caffeine intake is an independent risk factor for DO The relationship may be dose dependent Myers et al, 2000 Tea drinking (but not coffee) epidemiologically associated with all forms of incontinence Hannested et al, 2003 Diet Coke and caffeine-free Diet Coke cause greater U and F than carbonated water or Classic Coke Cartwright , ICS 2007 Weight loss decreases incontinence in moderately and morbidly obese women 4th ICI 2008, Level 1 Pelvic floor muscle/bladder training PFMT is better than no treatment, placebo, drug or inactive control treatment for women with SUI, UUI or MUI Level 1 Supervised PFMT should be offered as a first line therapy in all patients with SUI, UUI or MUI Grade A Not clear whether BT is more effective than drug therapy for women with DO or UUI Level 1 In a choice between BT and anticholinergic drug for women with DO or UUI, either may be effective Grade B Behavioural intervention Improves central control Underlying psychological abnormality Learn / re-learn both conscious and unconscious physiological processes Avoids side effects of drugs Bladder drill Requires high motivation Good support Encouragement High relapse rate Pharmacological treatment of OAB Antimuscarinics Drugs with mixed action Antidepressants Alpha-adrenoceptor antagonists Beta-adrenoceptor agonists Drugs acting on membrane channels Toxins Future drugs Antimuscarinic agents After lifestyle changes, antimuscarinic agents are the most common and currently the most widely used therapy for OAB syndrome Andersson, 2004 Antimuscarinics − − − − reduce intra-vesical pressure increase compliance raise volume threshold for micturition reduce uninhibited contractions Abrams et al, 2002 OAB: Antimuscarinics Oxybutynin Oral, Transdermal, Intra-vesical, gel Ditropan 2.5mg BD - 5mg QDS, Lyrinel XL 5-20mg OD, Kentera 3.9mgx2/wk, Oxybutynin in water 10mg TDS Tolterodine Oral Detrusitol 2mg BD, Detrusitol XL 4mg OD Propiverine Oral Detrunorm 15mg OD-TDS Solifenacin Oral Vesicare 5 or 10mg OD Trospium Oral Regurin 20mg BD, 60 mg OD Darifenacin Oral Emselex Enablex 7.5 or 15mg OD Fesoterodine Oral Toviaz 4 or 8mg OD Antimuscarinic side effects Tolerability and Compliance Questionnaire follow-up study of women with detrusor overactivity 5.5% were cured of their urinary symptoms 18.2% women continued drug therapy for more than six months Kelleher et al, 1997 Why do patients stop taking Antimuscarinics? Lack of efficacy is the major reason for failure of first-line antimuscarinic therapy: 0% 10% 20% 30% Female ≤55 Years of Age 50% 60% 70% 57 Male 50 In Employment/Activity Working 50 Retired/Unemployment 50 OAB Dry Pure UUI Insufficient efficacy 90% 24 18 3 31 7 30 26 61 24 Dosing convenience 16 Intolerable side effects 9 14 4 58 100% 2 9 4 8 39 66 Mixed UI 80% 30 47 Female >55 Years of Age Based on Market research 40% 2 10 3 10 2 13 Other reasons Antimuscarinic adverse effects: Meta-analysis Drug Constipation Blurred Vision Dry Mouth Darifenacin 7.5mg od 2.39 5.05 2.57 Darifenacin 15mg od 3.32 - 4.40 Fesoterodine 4mg od 1.47 0.20 3.01 Fesoterodine 8mg od 2.03 0.21 3.95 Tolterodine ER 4mg od 1.49 2.76 3.00 Solifenacin 5mg od 3.09 1.20 3.32 Solifenacin 10mg od 4.70 2.29 5.90 Oxybutynin IR 7.5-10mg 1.26 1.65 2.96 Oxybutynin 3.9mg TDS 0.26 1.18 1.41 Trospium Chloride 40mg 2.10 - 3.17 Propiverine ER 30mg 3.36 9.30 3.38 Chapple et al, 2008 83 trials: p=0.05; p=0.01 Vs placebo What’s new? Β3 -adrenoceptor agonist (mirabegron) Efficacy and Tolerance Significant effect in 60% of patients, dry rate 42% Equal efficacy in naïve and AM-resistant patients Side effects at placebo level Chapple et al, 2014. Combination therapy (AM + Β3) Efficacy and Tolerance Increased efficacy in naïve and non-naïve patients Reduced dosage of AM Acceptable side effects Drake et al, 2016. Surgical OAB Treatment Options Surgical (Invasive) Treatments Botulinum toxin (Botox 100 units?) Neuromodulation (TENS, PTNS, SNS) Augmentation enterocystoplasty (???) Urinary diversion (continent, Bricker) 35 THANKS ALL OF YOU