Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
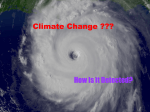
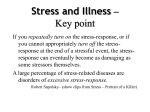
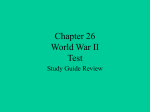
Review Article Perineural Invasion in Cancer A Review of the Literature Catherine Liebig, MD1; Gustavo Ayala, MD2; Jonathan A. Wilks, MD1; David H. Berger, MD1; and Daniel Albo, MD, PhD1 Perineural invasion (PNI) is the process of neoplastic invasion of nerves and is an under-recognized route of metastatic spread. It is emerging as an important pathologic feature of many malignancies, including those of the pancreas, colon and rectum, prostate, head and neck, biliary tract, and stomach. For many of these malignancies, PNI is a marker of poor outcome and a harbinger of decreased survival. PNI is a distinct pathologic entity that can be observed in the absence of lymphatic or vascular invasion. It can be a source of distant tumor spread well beyond the extent of any local invasion; and, for some tumors, PNI may be the sole route of metastatic spread. Despite increasing recognition of this metastatic process, there has been little progress in the understanding of molecular mechanisms behind PNI and, to date, no targeted treatment modalities aimed at this pathologic entity. The objectives of this review were to lay out a clear definition of PNI to highlight its significance in those malignancies in which it has been studied best. The authors also summarized current theories on the molecular mediators and pathogenesis of PNI and introduced current research models that are leading to advancements in the understanding of this metaC 2009 American Cancer Society. static process. Cancer 2009;115:3379–91. V KEY WORDS: perineural invasion, perineural spread, neurotropic carcinoma, cancer, neurotrophins, axon guidance molecule. A key feature of malignant cells is their ability to dissociate from the primary tumor and to establish metastatic deposits at distant sites. Vascular and lymphatic channels are well accepted routes of metastatic spread. They are well characterized in the literature and are the focus of much current research on tumor biology. However, another route of tumor spread that occurs in and along nerves has been described in the literature since the mid-1800s but has received relatively little research attention. Perineural invasion (PNI) is the process of neoplastic invasion of nerves. It also has been called neurotropic carcinomatous spread and perineural spread. PNI was reported first in the European literature by scientists who described head and neck cancers that exhibited a predilection for growth along nerves as they made their way toward the intracranial fossa.1,2 PNI has emerged since then as a key pathologic feature of many other malignancies, including those of the pancreas, colon and rectum, prostate, biliary tract, and stomach. For many of these malignancies, PNI is a marker of poor outcome and a harbinger of decreased survival.3-7 Corresponding author: Daniel Albo, MD, PhD, Michael E. DeBakey VA Medical Center, 2002 Holcombe Boulevard, OCL 112-A, Houston, TX 77030; Fax: (713) 794-7352; [email protected] 1 Department of Surgery, Michael E. DeBakey Veterans Affairs Medical Center, Baylor College of Medicine, Houston, Texas; 2Department of Pathology, Baylor College of Medicine, Houston, Texas Received: September 9, 2008; Revised: December 5, 2008; Accepted: January 7, 2009 C 2009 American Cancer Society Published online: May 29, 2009 V DOI: 10.1002/cncr.24396, www.interscience.wiley.com Cancer August 1, 2009 3379 Review Article PNI is a distinct pathologic entity that can be observed in the absence of lymphatic or vascular invasion. It can be a source of distant tumor spread well beyond the extent of any local invasion; and, for some tumors, PNI may be the sole route of metastatic spread. PNI is neither an extension of lymphatic metastasis nor simply tumor cell migration through a low-resistance plane. Definitive studies have proven that there are no lymphatics within the inner sanctum of the nerve sheath, and several layers of collagen and basement membrane separate the inside of the nerve from the surrounding lesion; this is not a low-resistance path.8-11 Despite increasing recognition of this metastatic process, there has been little progress in the understanding of molecular mechanisms behind PNI and, to date, no targeted treatment modalities aimed at this pathologic entity. In fact, the true prevalence of PNI in various malignancies still has not been established. Lack of a concise, universal definition for PNI across all disciplines has resulted in significant confusion and probably is 1 reason for the seemingly slow progress. It is the objective of this review to lay out a clear definition of PNI and to highlight its significance in those malignancies in which it has been characterized best. We also aim to summarize current theories on the molecular mediators and pathogenesis of PNI and to introduce current research models that are leading to advancements in our understanding of this metastatic process. It is our hypothesis that PNI is as significant in some tumors as lymphovascular invasion. A better understanding of PNI may lend insight into tumor metastasis and recurrence and open doors to improved staging strategies, novel treatment modalities, and perhaps even paradigm shifts in our treatment of patients with patients. Definition Knowledge of the basic structure of the peripheral nerve sheath is integral to understanding PNI (Fig. 1). The nerve sheath is composed of 3 connective tissue layers. From outside to in, these layers are the epineurium, the perineurium (not to be confused with the perineurum, or area just outside of the nerve sheath), and the endoneurium.12 The epineurium, which binds 1 or more fascicles into a single nerve, is composed of 2 distinct layers: an outer layer of areolar connective tissue and loosely arranged collagen bundles and an inner layer of densely 3380 organized collagen fibrils and elastin fibers.13 It is within the areolar connective tissue on the outer portion of the epineurium that the epineurial component of the vasa nervorum, the rich vascular network of the peripheral nerve, and the perineural lymphatic channels reside. According to the most recent literature, these lymphatics do not penetrate the epineurium, although this issue historically has been the focus of considerable debate in the PNI literature.8,14,15 Akert et al., using electron microscopy to delineate the structural organization of the perineurial sheath of the peripheral nerve, describe a multilamellated structure of concentrically arranged endothelial cells.11 Each endothelial cell layer of the perineurium is flanked on either side by basement membrane.9,11 Junctions between the endothelial cells are formed by dove-tailing, that is, overlapping and tightly fitting projections of adjacent cell membranes.11 These junctions, or zonulae occludentes, work together with the multiple basal laminae to confer a highly selective barrier function to the perineurium. This effectively separates the intrafascicular compartment of the nerve from the surrounding epineurium. The endoneurium, or innermost layer of the nerve sheath, forms a matrix around individual nerve fibers and envelops the Schwann cells and individual axons of the nerve.14 The endothelial lining of endoneurial blood vessels is made up of tight junctions without evidence of transendothelial channels.14 The relative impermeability of the endoneurial blood vessels is an extension of the barrier function of the perineurium surrounding this compartment and is a key feature of the blood-nerve barrier. Descriptions of PNI have included tumor cells within every layer of the peripheral nerve sheath, from abutment of tumor cells within the perineurum to well formed cancerous glands within the perineurium or endoneurium, to small clusters of tumor cells within a nerve that is surrounded by normal tissue well away from tumor. Which of these tumor nerve configurations are true examples of PNI and which features are necessary for defining PNI? In his 1985 article on neurotropic carcinomas, Batsakis offered a broad definition of PNI, characterizing it as tumor cell invasion in, around, and through the nerves.8 The article is cited widely in the literature on PNI, and the definition has become the generally accepted 1 for PNI. It is sufficiently broad to cover most of the histopathologic varieties of this entity previously described in the Cancer August 1, 2009 Perineural Invasion in Cancer/Liebig et al FIGURE 1. Perineural invasion: Illustrated is a tumor enveloping a peripheral nerve in cross section revealing tumor cell spread. Molecules expressed by tumors interact with surrounding stroma as well as receptors associated with peripheral nerves. literature and has helped to focus later research efforts by eliminating any confusion about perineural lymphatics. However, in, around, and through has left tremendous room for further clarification. Some authors have suggested that tumor cells must be observed inside the perineurial layer, specifically, to cite PNI.16 This definition seems overly stringent and would exclude several examples of clear nerve invasion, such as gland formation within the collagen layers of the epineurium. We advocate that the finding of tumor cells within any of the 3 layers of the nerve sheath represents PNI. A much more frequent finding in PNI is tumor-nerve contact within the perineurum without the finding of tumor cells inside of the sheath, and there is wide variability among authors regarding the degree to which this tumor-nerve contact is necessary to call it PNI. Various growth patterns have been described, Cancer August 1, 2009 including complete and incomplete encirclement, concentric lamination, and tangential contact.17 For instances in which this occurs outside of the main body of the tumor, the finding is recognized more easily as malignant carcinomatous invasion of a neural structure. However, in instances in which this occurs within the main body of the tumor, it is less clear cut. For these circumstances, many authors have proposed that at least 33% of the circumference of the nerve should be surrounded by tumor cells to call it PNI; anything less than 33% represents focal abutment and not invasion.17-19 In summary, we advocate a somewhat broad definition of PNI, in keeping with the original definition by Batsakis of in, around, and through the nerves, while incorporating many features that were cited previously in the literature: tumor in close proximity to nerve and involving at least 33% of its circumference or 3381 Review Article FIGURE 2. These photomicrographs depict perineural invasion (PNI) in human colorectal cancer specimens. Sections of human colorectal cancers were stained with hematoxylin and eosin and were reviewed by a pathologist for PNI. Tumor cells located within the peripheral nerve sheath either (a) in clusters or (b) forming glandular elements are clear examples of PNI. When tumor cells are not located inside of the nerve sheath but are in close proximity to the nerve in the perineural environment, at least 33% of the circumference of the nerve must be involved by tumor to diagnose PNI. This is true weather the nerve is located (c) within the main body of the tumor or (d) at a site outside of the primary tumor focus. tumor cells within any of the 3 layers of the nerve sheath (Fig. 2). Pathogenesis It has become evident that PNI is not an extension of lymphatic metastasis, as once was suggested. Definitive studies have demonstrated that lymphatic channels do not penetrate the inner sanctum of the nerve sheath.8-10,20 For the last 40 years, the predominant theory behind the pathogenesis of PNI has been that tumor cells spreading along neural sheaths are privileged to a low-resistance plane, which serves as a conduit for their migration. Once inside of the nerve sheath, tumor cells may be in a privi3382 leged growth environment that facilitates metastasis, but the multiple layers of collagen and basement membrane that compose the nerve sheath make access to this path anything but low-resistance. The reason certain carcinomas exhibit a predilection for PNI and others do not remains unknown. More recently, studies have demonstrated that PNI may involve reciprocal signaling interactions between tumor cells and nerves and that these invading tumor cells may have acquired the ability to respond to proinvasive signals within the peripheral nerve milieu. In a PNI model using mouse dorsal root ganglia (DRG) cocultured in a Matrigel matrix with prostate cancer cells, Ayala et al. demonstrated tumor cell migration along neurites toward Cancer August 1, 2009 Perineural Invasion in Cancer/Liebig et al Table 1. Neurotrophic Factors and Their Possible Functions and Expression Patterns in Cancer Factor Possible Function in Cancer Expression in Cancer References NGF May stimulate epithelial cancer cell growth and mediate nerve invasion through its interaction with trkA, an NGF-specific receptor; binding of NGF to trkA leads to activation of the p44/42 MAPK signaling pathway and up-regulation of MMP-2, a proinvasive mediator May be overexpressed by tumor cells to promote neurite growth; stimulates tumor cell invasion at low-to-moderate concentrations Overexpressed in pancreas cancer and prostate cancer cell lines; trkA is strongly expressed on the perineurium of peripheral nerves Ketterer 2003,27 Okada 2004,28 Zhu 1999,31 Zhang 2005,32 Zhu 2002,33 Geldov 1997,34 Kowalski 200235 Overexpressed in pancreas cancer and adenoid cystic carcinoma; expression does not correlate with the presence of PNI, suggesting that the BDNF-expressing phenotype may appear before nerves Overexpressed in specimens of human neural plexi; multiple pancreatic cancer cell lines express the RET protein tyrosine kinase receptor for GDNF Overexpressed in pancreas cancer specimens Ketterer 2003,27 Zhu 2002,33 Kowalski 2002,35 Miknyoczki 199936 BDNF GDNF Exhibits a chemotactic and chemokinetic effect on tumor cells and mediates increased MMP-9 expression and activity NT-3 Stimulates tumor cell invasion at low-to-moderate concentrations Okada 1999,29 Okada 200330 Ketterer 2003,27 Miknyoczki 199936 NGF indicates nerve growth factor; trkA, tropomyosin receptor kinase A (a high-affinity catalytic receptor for nerve growth factor); MAPK, mitogen-associated protein kinase; MMP-2, matrix metalloproteinase 2; BDNF, brain-derived neurotrophic factor; PNI, perineural invasion; GDNF, glial cell line-derived neurotrophic factor; NT-3, neurotrophin 3. the ganglia of origin as well as focused, directional outgrowth of neurites toward cancer cell colonies.21 The addition of stromal cells to the aforementioned in vitro model resulted in increased neurite outgrowth and cell colony formation.22 This suggests that the signaling mechanisms behind PNI likely involve at least 3 different cellular elements, including tumor cells, nerve cells, and stromal cells, and may include autocrine and paracrine mechanisms. The increased neurite formation demonstrated in the previous in vitro studies suggests that axonal migration may be a key element of PNI. Axonal growth is a complex process that requires neurotrophic growth factors and axonal guidance molecules.23,24 The neurotrophins are the best characterized family of neurotrophic factors and comprise nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), neurotrophin 3 (NT-3) and neurotrophin 4/5 (NT-4/5).25 It is their potent effects on neuronal growth that have made the neurotrophins prime candidates for study in the PNI invasion pathway. There is a growing body of literature implicating these molecules as well as other neurotrophic factors in cancer (Table 1). Recent evidence in prostate cancer suggests that there is an up-regulation in neurotrophin expression by tumor cells as an escape mechanism from dependence on paracrine expression by stromal elements.26 Ketterer et al., by using polymerase chain reaction analysis of microdissection Cancer August 1, 2009 specimens, discovered that there is an up-regulation in neurotrophin expression by tumor cells as well as intratumoral nerves in pancreas cancer.27 Tumor cells cannot migrate through extracellular matrix or nerve sheath without expressing proteinases. Matrix metalloproteinases (MMPs), and, in particular, the gelatinases (MMP-2 and MMP-9), seem to play a pivotal role in PNI. Okada et al. reported that exogenous NGF led to a dose-dependent increase in MMP-2 expression and tumor cell invasion in pancreatic cancer cells.28 This effect was mediated by binding NGF to its tropomyosin receptor kinase A (trkA) receptor, which is expressed on the tumor cell surface, with subsequent activation of the p44/42 mitogen-associated protein kinase signaling pathway.28 Pancreatic cancer overexpresses glial cell line-derived neurotrophic factor (GDNF).29 Migration of pancreatic cancer cells is increased by GDNF-secreting glioma cells in a dose-dependent fashion, suggesting both a chemotactic effect and a chemokinetic effect of GDNF on tumor cells.29 Furthermore, this pancreatic cancer cell migration depends on GDNF-induced up-regulation of MMP-9 expression and activity.30 Experimental Models Our understanding of the pathogenesis of PNI has been limited by a lack of effective models for this complex 3383 Review Article FIGURE 3. This in vitro model of perineural invasion in prostate cancer was developed by Ayala et al.21 Mouse dorsal root ganglia (DRG) are cocultured in Matrigel with circumferentially placed prostate cancer cells. DRG exhibit directional outgrowth of neurites in response to tumor cells and tumor cell colonies reveal increased growth in (a) a brightfield image and (b) a darkfield image (original magnification, 40). interaction between nerve, tumor cell, and stroma. Few in vitro models have proven capable of capturing even a single aspect of the disease process, and much of their limitations stemmed from the difficulty in culturing peripheral nerve preparations and in replicating the neural microenvironment. In vivo models have proven more promising, but these only recently have been developed. Below, we outline the available, effective in vitro and in vivo models of PNI and highlight some of the current research using these experimental designs. A critical element in the metastatic cascade is the ability of tumor cells to invade through basement membranes. These thin, specialized sheets of extracellular matrix act as barriers against cellular and macromolecular movement, particularly across epithelial layers and endothelial-lined spaces of the vasculature. Basement membrane also lines several cell layers of the neural sheath, making this metastatic process elemental to PNI as well. 3384 By using an in vitro assay that mimics tumor cell invasion of basement membrane and correlates with in vivo metastatic potential of cells, Miknyoczki et al. and Albini observed that BDNF and NT-3 stimulated pancreatic tumor cell invasion.36,37 In similar experiments, human prostate cancer cell invasion was up-regulated markedly in response to exogenous NGF and to NGF-like proteins secreted by human prostate stromal cells.34,38 These experiments suggest that there are complex signaling interactions between the peripheral nerve milieu, tumor stromal elements, and tumor cells. In 2001, Ayala et al. described a novel in vitro PNI model in which mouse DRG were cocultured with prostate cancer cells in a Matrigel matrix.21 The 3-dimensional Matrigel matrix suspends the ganglia and allows for multidirectional neurite outgrowth (Fig. 3). Some studies of neurite outgrowth have used cell suspensions of isolated neurons rather than explanted mammalian DRG; Cancer August 1, 2009 Perineural Invasion in Cancer/Liebig et al however, the influence that supportive glial cells have in promoting neurite growth and PNI certainly is lost.39 Three phenomena, as outlined above in the discussion of pathogenesis, were observed in the Matrigel/DRG model: 1) focused outgrowths of neurites projected into cancer cell colonies within 24 hours of culture; 2) cancer cell colony formation increased; and, 3) cancer cells migrated along contacted neurites toward the ganglion of origin. The results were reproducible across 3 different prostate cancer cell lines. This experiment effectively establishes the presence of a reciprocal growth interaction between cancer cells and neurites in vitro and also suggests that actively growing nervous tissue somehow may promote tumor cell invasion. To date, there are no data supporting this phenomenon in vivo. Several animal models recently have been developed for tumors that are known to metastasize through the perineural route. Pour et al. developed a Syrian hamster model of both carcinogenesis-induced and orthotopically transplanted pancreatic cancer.40 Both tumors demonstrated PNI in about 90% of cases. Furthermore, in this model, those authors demonstrated not only that tumor cells invade extrapancreatic neural plexi by this route but that they also reach distant metastatic sites, such as lymph nodes, through the perineural space. Eibl and Reber developed a model for pancreatic cancer recurrence in nude mice that underwent resection of pancreatic tumors at 4 weeks, 6 weeks, and 8 weeks after orthotopic implantation.41 Eighty percent of pancreatic tumors that were resected 6 weeks after orthotopic implantation recurred with extensive invasion of retroperitoneal nerves, but tumors that were resected at 4 weeks did not show signs of recurrence. These findings suggest that metastasis of retroperitoneal nerves may occur later in the disease process. This model may serve as an effective tool for studying early recurrences and may help with elucidating the role of nervous structures as sources of recurrence. Other animal models used for studying PNI include a chemically induced prostate carcinoma in Wistar rats that demonstrates frequent PNI and a nude mouse orthotopic injection model of human head and neck squamous cell carcinoma that leads to PNI in 100% of tumors.42,43 Both of these models result in tumors that closely mimic their human counterparts histologically and phenotypically and, thus, serve as useful tools for studying the molecular pathogenesis of PNI. Cancer August 1, 2009 Clinical Significance Some of the earliest observations of neural involvement by tumor were in cancers of the head and neck in which large nerves seemed to serve as ready conduits for intracranial extension. The incidence of PNI in head and neck cancers varies considerably by histology but is reported most commonly in squamous cell carcinoma in which the incidence is as high as 80%.44-46 PNI is a significant pathologic feature in head and neck cancers, heralding decreased survival, increased locoregional recurrence rates, and a shorter time to recurrence.17,45,47,48 In 1 series of 239 patients with mucosal squamous cell carcinomas, PNI was associated with a 23% 3-year survival rate versus 49% in patients with stage-matched, PNI-negative tumors in univariate analysis.45 Although treatment strategies for head and neck malignancies were beyond the scope of this review, it is noteworthy that PNI status often significantly affects surgical strategies and adjuvant treatments in head and neck cancers.49-53 The rationale for changing therapy based on PNI status is largely anecdotal without significant evidence.53 This is 1 of the only malignancies for which assessment of PNI status is a required component of the pathologic analysis according to the reporting protocols published by the College of American Pathologists.54 PNI is observed in as many as 75% of resected prostate cancer specimens and in 25% of biopsies from patients without lymph node metastases, and many authors agree that it is the most significant route of extracapsular spread in this malignancy.55,56 In 1 series of 78 prostatectomy specimens with extracapsular invasion, 50% of specimens had tumor penetrating the capsule solely along nerves; and, in the remaining 50% of specimens, capsule penetration through nerves was the predominant route.57 Several studies have demonstrated that the presence of PNI on prostate needle biopsy specimens can reliably predict capsular penetration at prostatectomy, although this claim remains disputed.58-60 In a series of 381 patients who received for low-risk prostate cancer, Beard et al. reported that the 5-year prostate-specific antigen (PSA) failure-free survival rate was 50% versus 80% in patients with and without PNI in their needle biopsy specimens, respectively.5 This association was observed only on univariate analysis, and PNI was not an independent predictor of PSA failure on multivariate analysis, as 3385 Review Article were pretreatment PSA level and Gleason score. However, there was a significant correlation between the presence of PNI and higher Gleason scores, suggesting that PNI may predict occult, high-grade disease in otherwise low-risk patients. Perineural involvement of benign prostatic glands is well recognized; PNI alone, without other signs of neoplasia, is not always diagnostic of prostate cancer.61 In a recent systematic review of investigations of PNI in prostate needle biopsy specimens, wide variability in study design, PNI frequency, and statistical analyses were observed; although the results suggested that PNI in prostate needle biopsy specimens may predict an adverse outcome after surgery or radiation, no conclusion could be reached based on data in that review, and there is no solid evidence that a PNI-positive biopsy should alter therapy.62 With regard to prostatectomy specimens, a study of 1550 patients from the University of Michigan indicated that PNI was a significant predictor of higher pathologic stage and positive margins on both univariate and multivariate analysis.63 However, investigations of PNI in prostatectomy specimens, like in studies of needle biopsies, lack consensus regarding biochemical failure rates and survival differences after surgery. Although there were 2 studies that revealed significantly worse outcomes associated with PNI, in the remaining studies, no statistical difference was oberved.55,64-70 In 1 study of 90 pancreatic adenocarcinoma specimens, PNI was observed in 88 tumors (98%).71 In that study, there was no association between PNI and tumor size, differentiation, or lymphovascular invasion; but there was a significant correlation between PNI and tumors with lymph node metastases. Reports on the incidence of PNI in pancreatic cancer cite a minimum of 70% of these tumors, and some authors even claim that 100% of these tumors. will exhibit PNI if enough sections are evaluated.3,72-75 Positive PNI status in pancreatic cancer predicts decreased survival, often independent of stage, but treatment remains unchanged by PNI status.3,71,73 In a subgroup analysis of 72 patients with lymph node-negative disease (stage I and stage II), the 5-year survival rate of patients without PNI was 75% versus 29% for those with PNI in their tumor specimens (P < .02).3 The pancreas is richly innervated by the autonomic nervous system, primarily through plexi from the celiac and superior mesenteric artery ganglia. Studies of extratumoral PNI in pancreatic cancer have focused on these plexi as likely sites 3386 of micrometastatic spread and sources for retroperitoneal recurrence, although these possibilities remain to be confirmed. Up to 72% of PNI-positive pancreatic adenocarcinomas demonstrate extrapancreatic nerve plexus involvement at the time of resection.71,76,77 The association between intratumoral PNI and extrapancreatic plexus involvement seems to correlate with the degree of invasion observed in the primary tumor and with the presence of PNI within the pancreas but outside of the main body of the tumor.71,76,77 PNI has been recognized in many series as a prevalent pathologic feature of colorectal cancer and is reported in up to 33% of these tumors at the time of resection.78-81 Several studies have demonstrated a significant correlation between the presence of PNI in colorectal tumors and increased locoregional recurrence rates, a 5-year survival rates, and an increased likelihood of finding metastatic disease at the time of resection.78,80,82-84 In 1 study of 563 rectal and rectosigmoid cancers, the presence of PNI was associated with a 27% cancer-specific 5-year survival rate versus a 78% 5-year survival rate in PNI-negative tumors (P < .001).4 Similar results were reported by Krasna et al. in their review of 77 patients with colorectal carcinoma. In that series, not only was survival lower in PNI-positive patients, but those patients were almost 3 times more likely to have metastatic disease at the time of diagnosis (27% vs 73%; P < .01).84 These results suggest a correlation between PNI status and advanced tumor stage, a relation that also has been demonstrated in other studies. For instance, in a review of 373 patients with rectal cancer who underwent curative resection, the incidence of PNI in patients with stage III disease was 20%, which was twice the incidence reported in the overall study population (10%).85 Perhaps more noteworthy is the prognostic significance of PNI in lymph node-negative disease, particularly stage II, in which it has been demonstrated that chemotherapy has no survival benefit. In an analysis of 124 patients with lymph node-negative colorectal cancer who underwent curative resection, the 5-year survival rate was 87% for patients with PNI-negative tumors versus 57% for patients with PNI-positive tumors (P < .006).86 Other studies similarly have indicated that positive PNI status portends a worse outcome in patients with lymph node-negative colorectal tumors.87-89 This suggests that PNI indicates a more aggressive tumor phenotype and may be useful in selecting a subgroup of lymph nodeCancer August 1, 2009 Perineural Invasion in Cancer/Liebig et al negative patients who could benefit from adjuvant therapy. Some patients with stage II disease currently are offered adjuvant therapy after resection of PNI-positive tumors, but outcomes data are not yet available.90 There is scant information on PNI in malignancies other than those discussed above. The reported incidence of PNI in cholangiocarcinoma is approximately 75% to 85%, and at least 2 studies have noted a significant correlation between PNI and decreased survival in patients with this malignancy.6,91,92 One series of 354 gastric cancer specimens cited a PNI-positive rate of 60% and a significant correlation with disease progression and overall survival.7 Reported rates of PNI in breast cancer range from 3% to 38%.93-95 PNI is reported often in conjunction with lymphovascular invasion as 1 pathologic feature of breast cancer, confounding its significance as an independent prognostic variable. Some studies have demonstrated a correlation between lymphovascular invasion/ PNI and decreased survival in breast cancer, whereas other studies have failed to demonstrate a correlation between PNI and outcome.96-99 Underreporting of PNI remains an obstacle to gaining an adequate understanding of its true prognostic significance. First, several factors make nerve invasion very difficult to recognize. Inflammatory cells or large, mucinous pools may obscure the presence of tumor cells around nerves. Microscopic foci of nerve invasion are common and also may escape detection.72 It has been demonstrated that evaluating specimens after staining for nerve-specific antigens markedly increases PNI detection rates compared with standard hematoxylin and eosin staining techniques.46,79 On a re-review of slides from 40 patients with head and neck squamous cell carcinoma, the rate of detection of PNI almost tripled from 30% to 82% when specimens were stained for protein S100.46 It is conceivable that nerve-specific staining may become a routine part of the pathologic evaluation of malignancies in which PNI status affects treatment. In addition to problems with detection, to date, there are no concrete guidelines on the reporting of PNI in malignancies other than head and neck cancers. This contributes further to the underreporting of PNI. According to the latest protocols published by the College of American Pathologists, evaluation of PNI is not a required element in pancreatic, colorectal, or prostate cancer pathology reports.100 Cancer August 1, 2009 Conclusion Since PNI first was described over a century ago, there has been a paradigm shift in our understanding of its pathogenesis. Initially, it was believed that PNI represented lymphatic spread of tumor into nerves; however, studies performed in the mid-1900s called this theory into question. By the late 1900s, the predominant theory became that of the nerve sheath as a low-resistance path for tumor spread. Although the ‘‘path of low resistance’’ theory still persists in the literature today, evidence is emerging indicating that the PNI phenomenon is more like invasion than simple diffusion. New models have been developed that provide strong evidence for signaling between the nerves and invading tumor cells. Stromal elements, including fibroblasts, also seem to play a key role in the complex signaling interactions driving PNI. Studies involving neurotrophins and axonal guidance molecules have implicated a few of the molecular mediators involved in the process, although we have only just begun to scratch the surface. We have highlighted the clinical significance of PNI in those malignancies in which it has been studied best. These include cancers of the head and neck, pancreas, colon and rectum, and prostate. Overall, PNI portends a significantly lower 5-year survival rate and signifies more advanced disease. There are many malignancies, however, for which we have only begun to recognize the significance of PNI. Breast cancer and hepatobiliary cancers are among these malignancies; however, preliminary evidence suggests that, 1 day, PNI also will be recognized as a significant pathologic feature in these and other tumors. With a better understanding of the pathogenesis and through work using animal models, we can begin to target PNI in our treatment strategies against those malignances for which PNI is significant. Gene profiling already has been used to identify an expression profile predictive of PNI in biliary tract cancers.101 These expression profiles are being evaluated for use in risk stratification and in guiding the extent of surgical resection; however, 1 day, the candidate genes or their downstream molecular pathways could serve as therapeutic targets. Several neurotrophins, including NGF, BDNF, and NT-3, have been implicated in promoting tumor cell invasion and may be key mediators in the pathogenesis of PNI.34,36,38 Researchers have begun searching for viable therapeutic targets among these neurotrophins and their 3387 Review Article receptors.36,102-104 Both anti-NGF antibodies and small interfering RNA against NGF have demonstrated efficacy against cell proliferation and angiogenesis in a breast cancer murine model.104 Intratumoral and peritumoral injection with antibodies against receptors for NGF and NT-3 have produced significant growth inhibition in both human pancreatic cancer and prostate cancer xenografts in a nude mouse model.105 Although much of our research has focused on tumor cell invasion of nerves, the PNI story is beginning to include axonal growth and possibly nerve ‘‘invasion’’ of tumor. A study performed by Maru et al. indicated that PNI diameter, measured with an ocular micrometer and defined as the largest focus of PNI in a tumor, was a better predictor of outcome in prostate cancer than PNI status alone.55 There is no clear explanation why this is the case. It is possible that tumors with larger foci of PNI are simply more advanced cancers, which we would expect to have worse outcomes; or perhaps there is nerve enlargement within these foci of PNI as a result of a cancer cell-promoted nerve growth phenomenon during PNI. Clearly, this aspect of PNI needs to be explored further; however, in vitro evidence certainly suggests that there is a reciprocal growth interaction occurring between nerves and tumors. It seems that progress in understanding PNI has been stymied by the lack of a concise definition for this pathologic process. We conclude that the definition offered by Batsakis in 1985—tumor cell invasion in, around, and through the nerves—leaves too much room for interpretation and is not precise enough to promote uniformity among researchers. After a thorough review of the literature, we have compiled criteria for the identification of PNI in a histologic specimen. Finding tumor cells within any of the 3 layers of the nerve sheath or tumor foci outside of the nerve with involvement of 33% of the nerve’s circumference are sufficient features for calling PNI. It is likely that, as our understanding of the pathogenesis of PNI evolves, so too will this definition. 2. Neumann E. Secondare cancroid infiltration des nervus mentalis bei einem. Arch Pathol Anat. 1862;24:201-201. 3. Ozaki H, Hiraoka T, Mizumoto R, et al. The prognostic significance of lymph node metastasis and intrapancreatic perineural invasion in pancreatic cancer after curative resection. Surg Today. 1999;29:16-22. 4. Law WL, Chu KW. Anterior resection for rectal cancer with mesorectal excision: a prospective evaluation of 622 patients. Ann Surg. 2004;240:260-268. 5. Beard CJ, Chen MH, Cote K, et al. Perineural invasion is associated with increased relapse after external beam radiotherapy for men with low-risk prostate cancer and may be a marker for occult, high-grade cancer. Int J Radiat Oncol Biol Phys. 2004;58:19-24. 6. Su CH, Tsay SH, Wu CC, et al. Factors influencing postoperative morbidity, mortality, and survival after resection for hilar cholangiocarcinoma. Ann Surg. 1996;223:384394. 7. Duraker N, Sisman S, Can G. The significance of perineural invasion as a prognostic factor in patients with gastric carcinoma. Surg Today. 2003;33:95-100. 8. Batsakis JG. Nerves and neurotropic carcinomas. Ann Otol Rhinol Laryngol. 1985;94(4 pt 1):426-427. 9. Hassan MO, Maksem J. The prostatic perineural space and its relation to tumor spread: an ultrastructural study. Am J Surg Pathol. 1980;4:143-148. Conflict of Interest Disclosures 16. Veness MJ. Perineural spread in head and neck skin cancer. Australas J Dermatol. 2000;41:117-119. The authors made no disclosures. References 1. Cruveilheir J. Maladies Des Nerfs Anatomie Pathologique Du Corps Humain. 2nd ed. Paris, France: JB Bailliere; 1835. 3388 10. Rodin AE, Larson DL, Roberts DK. Nature of the perineural space invaded by prostatic carcinoma. Cancer. 1967;20: 1772-1779. 11. Akert K, Sandri C, Weibel ER, et al. The fine structure of the perineural endothelium. Cell Tissue Res. 1976;165:281295. 12. Peters A. Connective tissue sheaths of peripheral nerves. In: Peters A, Palay SL, Webster H, eds. The Fine Structure of the Nervous System: Neurons and Their Supporting Cells, 3rd ed. New York, NY: Oxford University Press; 1991:494. 13. Stolinski C. Structure and composition of the outer connective tissue sheaths of peripheral nerve. J Anat. 1995; 186(pt 1):123-130. 14. Olsson Y. Microenvironment of the peripheral nervous system under normal and pathological conditions. Crit Rev Neurobiol. 1990;5:265-311. 15. Larson DL, Rodin AE, Roberts DK, et al. Perineural lymphatics: myth or fact? Am J Surg. 1966;112:488-492. 17. Fagan JJ, Collins B, Barnes L, et al. Perineural invasion in squamous cell carcinoma of the head and neck. Arch Otolaryngol Head Neck Surg. 1998;124:637-640. 18. Bockman DE, Buchler M, Beger HG. Interaction of pancreatic ductal carcinoma with nerves leads to nerve damage. Gastroenterology. 1994;107:219-230. Cancer August 1, 2009 Perineural Invasion in Cancer/Liebig et al 19. Nagakawa T, Kayahara M, Ohta T, et al. Patterns of neural and plexus invasion of human pancreatic cancer and experimental cancer. Int J Pancreatol. 1991;10:113-119. 20. Reina MA, Lopez A, Villanueva MC, et al. Morphology of peripheral nerves, their sheaths, and their vascularization [in Spanish]. Rev Esp Anestesiol Reanim. 2000;47:464-475. 21. Ayala GE, Wheeler TM, Shine HD, et al. In vitro dorsal root ganglia and human prostate cell line interaction: redefining perineural invasion in prostate cancer. Prostate. 2001; 49:213-223. 22. Cornell RJ, Rowley D, Wheeler T, et al. Neuroepithelial interactions in prostate cancer are enhanced in the presence of prostatic stroma. Urology. 2003;61:870-875. 23. Chilton JK. Molecular mechanisms of axon guidance. Dev Biol. 2006;292:13-24. 24. Chedotal A, Kerjan G, Moreau-Fauvarque C. The brain within the tumor: new roles for axon guidance molecules in cancers. Cell Death Differ. 2005;12:1044-1056. 25. Boyd JG, Gordon T. Neurotrophic factors and their receptors in axonal regeneration and functional recovery after peripheral nerve injury. Mol Neurobiol. 2003;27:277-324. 26. Dalal R, Djakiew D. Molecular characterization of neurotrophin expression and the corresponding tropomyosin receptor kinases (trks) in epithelial and stromal cells of the human prostate. Mol Cell Endocrinol. 1997;134:15-22. 27. Ketterer K, Rao S, Friess H, et al. Reverse transcriptionPCR analysis of laser-captured cells points to potential paracrine and autocrine actions of neurotrophins in pancreatic cancer. Clin Cancer Res. 2003;9:5127-5136. 28. Okada Y, Eibl G, Guha S, Duffy JP, Reber HA, Hines OJ. Nerve growth factor stimulates MMP-2 expression and activity and increases invasion by human pancreatic cancer cells. Clin Exp Metastasis. 2004;21:285-292. 29. Okada Y, Takeyama H, Sato M, et al. Experimental implication of celiac ganglionotropic invasion of pancreatic-cancer cells bearing c-ret proto-oncogene with reference to glial-cell-line-derived neurotrophic factor (GDNF). Int J Cancer. 1999;81:67-73. 30. Okada Y, Eibl G, Duffy JP, et al. Glial cell-derived neurotrophic factor upregulates the expression and activation of matrix metalloproteinase-9 in human pancreatic cancer. Surgery. 2003;134:293-299. 31. Zhu Z, Friess H, diMola FF, et al. Nerve growth factor expression correlates with perineural invasion and pain in human pancreatic cancer. J Clin Oncol. 1999;17:24192428. 32. Zhang Y, Dang C, Ma Q, et al. Expression of nerve growth factor receptors and their prognostic value in human pancreatic cancer. Oncol Rep. 2005;14:161-171. 33. Zhu Z, Kleeff J, Kayed H, et al. Nerve growth factor and enhancement of proliferation, invasion, and tumorigenicity of pancreatic cancer cells. Mol Carcinog. 2002;35:138-147. 34. Geldof AA, De Kleijn MA, Rao BR, et al. Nerve growth factor stimulates in vitro invasive capacity of DU145 Cancer August 1, 2009 human prostatic cancer cells. J Cancer Res Clin Oncol. 1997;123:107-112. 35. Kowalski PJ, Paulino AF. Perineural invasion in adenoid cystic carcinoma: its causation/promotion by brain-derived neurotrophic factor. Hum Pathol. 2002;33:933-936. 36. Miknyoczki SJ, Lang D, Huang L, et al. Neurotrophins and Trk receptors in human pancreatic ductal adenocarcinoma: expression patterns and effects on in vitro invasive behavior. Int J Cancer. 1999;81:417-427. 37. Albini A. Tumor and endothelial cell invasion of basement membranes. The Matrigel chemoinvasion assay as a tool for dissecting molecular mechanisms. Pathol Oncol Res. 1998;4: 230-241. 38. Djakiew D, Pflug BR, Delsite R, et al. Chemotaxis and chemokinesis of human prostate tumor cell lines in response to human prostate stromal cell secretory proteins containing a nerve growth factor-like protein. Cancer Res. 1993;53:1416-1420. 39. Tonge DA, Golding JP, Edbladh M, et al. Effects of extracellular matrix components on axonal outgrowth from peripheral nerves of adult animals in vitro. Exp Neurol. 1997; 146:81-90. 40. Pour PM, Egami H, Takiyama Y. Patterns of growth and metastases of induced pancreatic cancer in relation to the prognosis and its clinical implications. Gastroenterology. 1991;100:529-536. 41. Eibl G, Reber HA. A xenograft nude mouse model for perineural invasion and recurrence in pancreatic cancer. Pancreas. 2005;31:258-262. 42. Cabanillas R, Secades P, Rodrigo JP, et al. Orthotopic murine model of head and neck squamous cell carcinoma [in Spanish]. Acta Otorrinolaringol Esp. 2005;56:89-95. 43. Bosland MC, Prinsen MK, Dirksen TJ, et al. Characterization of adenocarcinomas of the dorsolateral prostate induced in Wistar rats by N-methyl-N-nitrosourea, 7,12dimethylbenz(a)anthracene, and 3,20 -dimethyl-4-aminobiphenyl, following sequential treatment with cyproterone acetate and testosterone propionate. Cancer Res. 1990;50:700709. 44. Carter RL, Foster CS, Dinsdale EA, et al. Perineural spread by squamous carcinomas of the head and neck: a morphological study using antiaxonal and antimyelin monoclonal antibodies. J Clin Pathol. 1983;36:269-275. 45. Soo KC, Carter RL, O’Brien CJ, et al. Prognostic implications of perineural spread in squamous carcinomas of the head and neck. Laryngoscope. 1986;96:1145-1148. 46. Kurtz KA, Hoffman HT, Zimmerman MB, et al. Perineural and vascular invasion in oral cavity squamous carcinoma: increased incidence on re-review of slides and by using immunohistochemical enhancement. Arch Pathol Lab Med. 2005;129:354-359. 47. Goepfert H, Dichtel WJ, Medina JE, et al. Perineural invasion in squamous cell skin carcinoma of the head and neck. Am J Surg. 1984;148:542-547. 3389 Review Article 48. O’Brien CJ, Lahr CJ, Soong SJ, et al. Surgical treatment of early stage carcinoma of the oral tongue—would adjuvant treatment be beneficial? Head Neck Surg. 1986;8:401-408. 65. Endrizzi J, Seay T. The relationship between early biochemical failure and perineural invasion in pathological T2 prostate cancer. BJU Int. 2000;85:696-698. 49. Shah N, Saunders MI, Dische S. A pilot study of postoperative CHART and CHARTWEL in head and neck cancer. Clin Oncol (R Coll Radiol). 2000;12:392-396. 66. Merrilees AD, Bethwaite PB, Russell GL, et al. Parameters of perineural invasion in radical prostatectomy specimens lack prognostic significance. Mod Pathol. 2008;21:10951100. 50. Brandwein-Gensler M, Teixeira MS, Lewis CM, et al. Oral squamous cell carcinoma: histologic risk assessment, but not margin status, is strongly predictive of local disease-free and overall survival. Am J Surg Pathol. 2005;29:167-178. 51. Garcia-Serra A, Hinerman RW, Mendenhall WM, et al. Carcinoma of the skin with perineural invasion. Head Neck. 2003;25:1027-1033. 52. Mendenhall WM, Amdur RJ, Williams LS, et al. Carcinoma of the skin of the head and neck with perineural invasion. Head Neck. 2002;24:78-83. 53. Mendenhall WM, Amdur RJ, Hinerman RW, et al. Skin cancer of the head and neck with perineural invasion. Am J Clin Oncol. 2007;30:93-96. 54. Pilch BZ, Gillies E, Houck JR, et al. Upper Aerodigestic Tract Cancer Protocols and Checklists. Northfield, Ill: College of American Pathologists, 2005. 55. Maru N, Ohori M, Kattan MW, et al. Prognostic significance of the diameter of perineural invasion in radical prostatectomy specimens. Hum Pathol. 2001;32:828-833. 56. Ayala GE, Dai H, Ittmann M, et al. Growth and survival mechanisms associated with perineural invasion in prostate cancer. Cancer Res. 2004;64:6082-6090. 57. Villers A, McNeal JE, Redwine EA, et al. The role of perineural space invasion in the local spread of prostatic adenocarcinoma. J Urol. 1989;142:763-768. 58. Bastacky SI, Walsh PC, Epstein JI. Relationship between perineural tumor invasion on needle biopsy and radical prostatectomy capsular penetration in clinical stage B adenocarcinoma of the prostate. Am J Surg Pathol. 1993;17:336-341. 59. de la Taille A, Katz A, Bagiella E, et al. Perineural invasion on prostate needle biopsy: an independent predictor of final pathologic stage. Urology. 1999;54:1039-1043. 60. Rubin MA, Mucci NR, Manley S, et al. Predictors of Gleason pattern 4/5 prostate cancer on prostatectomy specimens: can high grade tumor be predicted preoperatively? J Urol. 2001;165:114-118. 61. Ali TZ, Epstein JI. Perineural involvement by benign prostatic glands on needle biopsy. Am J Surg Pathol. 2005;29: 1159-1163. 62. Harnden P, Shelley MD, Clements H, et al. The prognostic significance of perineural invasion in prostatic cancer biopsies: a systematic review. Cancer. 2007;109:13-24. 67. Ng JC, Koch MO, Daggy JK, et al. Perineural invasion in radical prostatectomy specimens: lack of prognostic significance. J Urol. 2004;172(6 pt 1):2249-2251. 68. Miyake H, Sakai I, Harada K, et al. Limited value of perineural invasion in radical prostatectomy specimens as a predictor of biochemical recurrence in Japanese men with clinically localized prostate cancer. Hinyokika Kiyo. 2005; 51:241-246. 69. Ito K, Nakashima J, Mukai M, et al. Prognostic implication of microvascular invasion in biochemical failure in patients treated with radical prostatectomy. Urol Int. 2003;70:297302. 70. van den Ouden D, Hop WC, Kranse R, et al. Tumour control according to pathological variables in patients treated by radical prostatectomy for clinically localized carcinoma of the prostate. Br J Urol. 1997;79:203-211. 71. Takahashi T, Ishikura H, Motohara T, et al. Perineural invasion by ductal adenocarcinoma of the pancreas. J Surg Oncol. 1997;65:164-170. 72. Pour PM, Bell RH, Batra SK. Neural invasion in the staging of pancreatic cancer. Pancreas. 2003;26:322-325. 73. Hirai I, Kimura W, Ozawa K, et al. Perineural invasion in pancreatic cancer. Pancreas. 2002;24:15-25. 74. Noto M, Miwa K, Kitagawa H, et al. Pancreas head carcinoma: frequency of invasion to soft tissue adherent to the superior mesenteric artery. Am J Surg Pathol. 2005;29: 1056-1061. 75. Kayahara M, Nagakawa T, Futagami F, et al. Lymphatic flow and neural plexus invasion associated with carcinoma of the body and tail of the pancreas. Cancer. 1996;78: 2485-2491. 76. Nakao A, Harada A, Nonami T, et al. Clinical significance of carcinoma invasion of the extrapancreatic nerve plexus in pancreatic cancer. Pancreas. 1996;12:357-361. 77. Nagakawa T, Kayahara M, Ueno K, et al. A clinicopathologic study on neural invasion in cancer of the pancreatic head. Cancer. 1992;69:930-935. 78. Horn A, Dahl O, Morild I. Venous and neural invasion as predictors of recurrence in rectal adenocarcinoma. Dis Colon Rectum. 1991;34:798-804. 63. Lee IH, Roberts R, Shah RB, et al. Perineural invasion is a marker for pathologically advanced disease in localized prostate cancer. Int J Radiat Oncol Biol Phys. 2007;68:1059-1064. 79. Bellis D, Marci V, Monga G. Light microscopic and immunohistochemical evaluation of vascular and neural invasion in colorectal cancer. Pathol Res Pract. 1993;189:443447. 64. Ozcan F. Correlation of perineural invasion on radical prostatectomy specimens with other pathologic prognostic factors and PSA failure. Eur Urol. 2001;40:308-312. 80. Matsushima T, Mori M, Kido A, et al. Preoperative estimation of neural invasion in rectal carcinoma. Oncol Rep. 1998;5:73-76. 3390 Cancer August 1, 2009 Perineural Invasion in Cancer/Liebig et al 81. Moore PA, Dilawari RA, Fidler WJ. Adenocarcinoma of the colon and rectum in patients less than 40 years of age. Am Surg. 1984;50:10-14. 94. Elmore JG, Moceri VM, Carter D, et al. Breast carcinoma tumor characteristics in black and white women. Cancer. 1998;83:2509-2515. 82. Bentzen SM, Balslev I, Pedersen M, et al. Time to locoregional recurrence after resection of Dukes’ B and C colorectal cancer with or without adjuvant postoperative radiotherapy. A multivariate regression analysis. Br J Cancer. 1992;65:102-107. 95. Cowan WK, Kelly P, Sawan A, et al. The pathological and biological nature of screen-detected breast carcinomas: a morphological and immunohistochemical study. J Pathol. 1997;182:29-35. 83. Ross A, Rusnak C, Weinerman B, et al. Recurrence and survival after surgical management of rectal cancer. Am J Surg. 1999;177:392-395. 84. Krasna MJ, Flancbaum L, Cody RP, et al. Vascular and neural invasion in colorectal carcinoma. Incidence and prognostic significance. Cancer. 1988;61:1018-1023. 85. Shirouzu K, Isomoto H, Kakegawa T. Prognostic evaluation of perineural invasion in rectal cancer. Am J Surg. 1993;165:233-237. 86. Onate-Ocana LF, Montesdeoca R, Lopez-Graniel CM, et al. Identification of patients with high-risk lymph nodenegative colorectal cancer and potential benefit from adjuvant chemotherapy. Jpn J Clin Oncol. 2004;34:323-328. 87. Burdy G, Panis Y, Alves A, et al. Identifying patients with T3-T4 node-negative colon cancer at high risk of recurrence. Dis Colon Rectum. 2001;44:1682-1688. 88. Horn A, Dahl O, Morild I. The role of venous and neural invasion on survival in rectal adenocarcinoma. Dis Colon Rectum. 1990;33:598-601. 89. Di Fabio F, Nascimbeni R, Villanacci V, et al. Prognostic variables for cancer-related survival in node-negative colorectal carcinomas. Dig Surg. 2004;21:128-133. 90. De Dosso S, Sessa C, Saletti P. Adjuvant therapy for colon cancer: present and perspectives. Cancer Treat Rev. 2009; 35:160-166. 91. He P, Shi JS, Chen WK, et al. Multivariate statistical analysis of clinicopathologic factors influencing survival of patients with bile duct carcinoma. World J Gastroenterol. 2002;8:943-946. 92. Nagakawa T, Mori K, Nakano T, et al. Perineural invasion of carcinoma of the pancreas and biliary tract. Br J Surg. 1993;80:619-621. 93. Ho CM, Mak CK, Lau Y, et al. Skin involvement in invasive breast carcinoma: safety of skin-sparing mastectomy. Ann Surg Oncol. 2003;10:102-107. Cancer August 1, 2009 96. McCready DR, Chapman JA, Hanna WM, et al. Factors affecting distant disease-free survival for primary invasive breast cancer: use of a log-normal survival model. Ann Surg Oncol. 2000;7:416-426. 97. McCready DR, Chapman JA, Hanna WM, et al. Factors associated with local breast cancer recurrence after lumpectomy alone: postmenopausal patients. Ann Surg Oncol. 2000;7:562-567. 98. Mate TP, Carter D, Fischer DB, et al. A clinical and histopathologic analysis of the results of conservation surgery and radiation therapy in stage I and II breast carcinoma. Cancer. 1986;58:1995-2002. 99. Roses DF, Bell DA, Flotte TJ, et al. Pathologic predictors of recurrence in stage 1 (T1N0M0) breast cancer. Am J Clin Pathol. 1982;78:817-820. 100. College of American Pathologists. Cancer Protocols and Checklists. Northfield, Ill: College of American Pathologists; 2007. 101. Murakawa K, Tada M, Takada M, et al. Prediction of lymph node metastasis and perineural invasion of biliary tract cancer by selected features from cDNA array data. J Surg Res. 2004;122:184-194. 102. Papatsoris AG, Liolitsa D, Deliveliotis C. Manipulation of the nerve growth factor network in prostate cancer. Expert Opin Investig Drugs. 2007;16:303-309. 103. Desmet CJ, Peeper DS. The neurotrophic receptor TrkB: a drug target in anticancer therapy? Cell Mol Life Sci. 2996l63(7-8):755-759. 104. Adriaenssens E, Vanhecke E, Saule P, et al. Nerve growth factor is a potential therapeutic target in breast cancer. Cancer Res. 2008;68:346-351. 105. Miknyoczki SJ, Wan W, Chang H, et al. The neurotrophin-trk receptor axes are critical for the growth and progression of human prostatic carcinoma and pancreatic ductal adenocarcinoma xenografts in nude mice. Clin Cancer Res. 2002;8:1924-1931. 3391