Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
The patient with 20/20 vision who
can’t read
UBC Clinical Neuroophthalmology Day
Jason Barton
What do you need to read?
• 1. Low-level visual processes - intact central 5 degrees
• 2. Eye movements - steady fixation and accurate saccades
• 3. Attention
• 4. Higher level visual processes - to decode form into letters and words
• 5. Linguistic analysis - generating meaning and pronunciation from word
forms that are seen
Conclusion: reading can be derailed by a wide variety of problems.
A systematic approach to acquired reading disorders is useful.
1. Visual fields and reading
A. hemianopic dyslexia - central 5 degrees.
Left hemianopia: trouble finding the beginning of lines, since the left
margin disappears into the field defect as they scan rightwards.
• Marking their place with an L-shaped ruler helps.
Right hemianopia:
prolongs reading times, with increased numbers of fixations and reduced
amplitude of reading saccades to the right.
• Smaller type and learning to read obliquely with the page turned nearly
90 degrees may help.
• Reading performance can improve with time as both types of patients
learn adaptive strategies
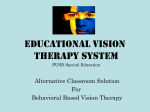
Hemianopic dyslexia- eye movements:
Trauzettel-Klosinski S, Brendler K. Eye movements in reading with hemianopic field
defects: the significance of clinical parameters. Graefe’s Arch Clin Exp Ophthalmol 1998;
236: 91-102
Normal
Left hemianopia
Right hemianopia
Case: Hemianopic dyslexia
37 year old man in MVA with brief LOC.
Complains of difficulty reading.
20/20 ou.
1. Visual fields and reading
B. hemifield slide, with
bitemporal hemianopia
absence of overlapping
regions of binocular visual
field leads to unstable
binocular alignment with
transient duplication or
disappearance of words
during reading.
Case: Hemifield slide.
35 year old woman with 3 days of episodic diplopia:
with reading, letters suddenly double, at other times they disappear.
across the room vertical steps appear in windowsills and doorframes.
She denied any visual loss.
20/20 OU. no RAPD. bilateral optic disc pallor.
2. Eye movements and reading.
A. Inability to maintain steady fixation:
(i) Nystagmus in primary position
- congenital (usually with reduced acuity)
- acquired
- vestibular (usually too dizzy to read)
- central (downbeat! - worse in downgaze)
(ii) Saccadic intrusions
- opsoclonus and ocular flutter
- square wave jerks - PSP
2. Eye movements and reading.
B. Inability to make accurate saccades:
(i) Saccadic dysmetria (cerebellar lesions)
(ii) Saccadic gaze palsy:
- acquired ocular motor apraxia
(bilateral frontal/parietal lesions)
- supranuclear downgaze palsy
(PSP, paramedian infarct)
* Note: smooth pursuit is irrelevant to reading
Case: Saccadic dysmetria and macrosaccadic oscillations
33 year-old woman with multiple sclerosis, presenting 12 years prior with optic
QuickTime™ and a
Cinepak decompressor
are needed to see this picture.
3. Attention and reading.
Neglect dyslexia.
Left hemi-neglect, right parietal or frontal lesions
• space-centered deficit: omit left side of lines or pages.
• object-centered deficit: omit left side of words.
- omissions ('bright' = 'right'),
- additions ('right' = 'bright')
- substitutions ('right' = 'light').
vertically printed text is not affected.
*may occur without
other signs of hemi-neglect
4. Higher level visual processes
Pure alexia (alexia without agraphia)
Spectrum of severity:
• global alexia:
cannot read numbers, letters and other abstract symbols
(musical notation, road signs and map symbols)
• letter-by-letter reading:
slow reading with occasional errors,
decipher words one letter at a time
characteristic = word-length effect:
reading time correlates with
the number of letters in the word
Associated signs (not invariable):
• right hemianopia/superior quadrantanopia
• anomia for colours and sometimes other visual objects.
• impaired verbal memory, other visual agnosias,
• optic ataxia: right hand has difficulty reaching to left visual field
Left medial occipitotemporal lesion (PCA infarct)
Two major explanations exist for pure alexia.
1. Disconnection alexia
Most commonly,
a) left occipital lesion = complete right hemianopia.
Therefore no visual input to left language areas from the left brain.
AND
b) splenium/forceps major/periventricular white matter occipital horn,
interrupt callosal fibers from the intact right occipital lobe.
Therefore no visual input to left language areas from the right brain.
Support: unusual cases with combination of a splenial lesion and
right hemianopia from left non-occipital lesions, e.g. LGN.
Two major explanations exist for pure alexia.
2. Word form agnosia
visual agnosia from dysfunction of the left ventral extrastriate cortex
fMRI shows activation of left “visual fusiform word area” by reading.
associated with impaired processing of local texture, identification of
complex objects in drawings
Support: pathologic reports showing left fusiform and lingual gyral lesion
but no splenial degeneration
5. Central (linguistic) dyslexia
Most often associated with aphasia, dementia
“Alexia with agraphia” - left angular gyrus lesion
may be associated with other signs of Gerstmann’s syndrome
(acalculia, right-left disorientation)
Linguistic variants:
• Phonological dyslexia - patients have lost the spelling rules but not
their dictionary.
problems only emerge when they have to spell novel words or
pseudo-words (‘grickle’, ‘centus’).
• Surface dyslexia - patients have lost the dictionary but not the rules
patients can only read if they can sound it out. Hence they have
trouble with irregular words (‘yacht’, ‘colonel’)
• Deep dyslexia - patients have lost spelling rules and also make
semantic errors (reading ‘cat’ for ‘dog’)
Alexia with agraphia
55 year-old right-handed man with several weeks of daily headaches.
Subtotal resection of left angular gyrus mass: glioblastoma.
Exam: fluent speech, normal comprehension, mild anomia. trouble with
calculations, right/left orientation.
20/30 od, 20/20 os. macular-splitting right hemianopia. Fundi normal.
Difficulty reading- made semantic errors: (beautiful = ‘pretty’, but = ‘and’)
Difficulty writing - spider = ‘sitre’, kite = ‘kibe’, hammer = ‘harer’
SUMMARY: When reading doesn’t work:
• Low-level visual processes:
hemianopic dyslexia (central 5 degrees)
hemifield slide
• Eye movements:
fixation - nystagmus, saccadic intrusions
saccades - dysmetria or palsy
• Attention:
hemineglect dyslexia
• Higher level visual processes:
pure alexia (disconnection, word-form agnosia)
• Linguistic analysis
alexia with agraphia, central dyslexias