Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
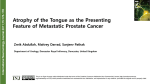
95 Cranial Nerve Disorders Ernest E. Wang KEY POINTS • The 12 cranial nerves supply motor and sensory innervation to the head and neck. • Cranial nerve disorders generally cause visual disturbances, facial weakness, or facial pain or paresthesias, depending on the nerve or nerves involved. • Trigeminal neuralgia and Bell palsy are common cranial nerve disorders. • A thorough history and physical examination should focus on assessing the potential for trauma (skull fracture), tumor, cerebrovascular accidents, vascular derangements (aneurysm, dissection, thrombosis), and infection (meningitis, abscess). • The presence of concomitant focal neurologic or systemic signs should heighten suspicion for a central rather than a peripheral cause of the neurologic dysfunction. PERSPECTIVE The 12 cranial nerves provide motor and sensory innervation to the head and neck. Some nerves serve purely motor functions (cranial nerves III, IV, VI, XI, and XII), some serve purely sensory functions (cranial nerves I, II, and VIII), and the remainder serve mixed motor and sensory functions (cranial nerves V, VII, IX, and X). In addition to somatic and visceral sensory components, the cranial nerves provide the special sensory functions of sight, smell, hearing, taste, and balance. Understanding the functions of individual cranial nerves aids in recognition of patterns of the clinical syndromes classically associated with disorders of specific cranial nerves. EPIDEMIOLOGY Cranial neuropathies are a heterogeneous group of disorders with a variety of causes. Trauma is a common cause, and 818 diabetes and hypertension are common comorbid conditions. Cranial nerves I, VI, and VII are the most frequently affected after minor head trauma.1 Trigeminal neuralgia is a common cause of facial pain that affects approximately 4.5 per 100,000 individuals; women are affected twice as often as men, and it is more common in those older than 60 years.2 Trigeminal neuralgia can be severely debilitating and has been termed the “suicide disease.”3 Bell palsy is the most common cause of acute facial paralysis worldwide. The peak age at incidence has been reported to be between 15 and 45 years,4 but other investigators have noted an increased incidence in individuals older than 70.5,6 Pregnant women and patients with diabetes have an associated increased incidence of the disease. A familial association of Bell palsy is noted in 4% of cases,4 and it can cause both significant psychologic and physical morbidity. PATHOPHYSIOLOGY CRANIAL NERVE I (OLFACTORY NERVE) Anatomy Cranial nerve I is a special sensory nerve that provides the sense of smell. Inhaled scents are detected by the olfactory epithelium lining the nasal cavity and transmitted to the olfactory bulb, which lies adjacent to the cribriform plate of the ethmoid bone. Olfactory sensations are relayed from the olfactory bulb to the brain via the olfactory tract. Presenting Signs and Symptoms The patient should be questioned about a history of head trauma. An anteroposterior skull fracture parallel to the sagittal suture or an anteroposterior shearing injury can tear the olfactory fibers traversing the cribriform plate and lead to disruption of the synapses from the olfactory epithelium to the olfactory bulb. A frontal lobe mass such as a tumor, meningioma, or abscess can compress the olfactory bulb as well, but the signs and symptoms associated with such masses tend to be more subacute. Treatment Treatment depends on the presence of concomitant injury. Basilar skull fracture and cerebrospinal fluid rhinorrhea associated with trauma require immediate neurosurgical consultation. A subacute mass or abscess should be managed in CHAPTER 95 consultation with neurosurgery, depending on the acuity of the findings. Patients with anosmia secondary to trauma and normal findings on head computed tomography (CT) can referred to neurology or neurosurgery for outpatient follow-up. CRANIAL NERVE II (OPTIC NERVE) Anatomy Visual stimuli are transmitted from the retina to the optic nerve through the optic chiasm to the lateral geniculate nucleus in the thalamus, where they synapse. From there, impulses are transmitted along the optic radiations (geniculocalcarine tracts, including the Meyer loop) to the primary visual cortex in the occipital lobes. Presenting Signs and Symptoms Unilateral loss of vision is most common with injuries to the optic nerve. Patients with bilateral visual loss may not be aware of any such injury until an examination is performed. Acute visual loss is often of vascular origin, including central retinal arterial or venous occlusion and cerebrovascular disease. Neurologic causes, such as multiple sclerosis, may be suggested by progression of the visual loss over a period of hours or days, pain, and a history of additional neurologic complaints with a recurrent waxing and waning pattern. Inflammatory processes such as optic neuritis may be the initial symptom of multiple sclerosis. Neuropathy from temporal arteritis usually occurs in elderly patients and is associated with progressive loss of vision (unilaterally or bilaterally), constitutional symptoms, jaw claudication, and headache. Idiopathic intracranial hypertension should be considered in patients with a history of headache, visual scotomata, and visual changes. The typical patient is a young, heavy-set woman who is taking oral contraceptives. The headache and visual changes are typically worsened by coughing, bend ing over, or performing techniques such as the Valsalva maneuver. Orbital compressive tumors or aneurysms cause mass effects that compromise optic nerve function. Differential Diagnosis The differential patterns of visual loss are described in Box 95.1. Treatment Treatment depends on the cause. Emergency ophthalmologic consultation is essential for vascular causes. Treatment of central retinal artery occlusion should focus on lowering intraocular pressure. Inpatient evaluation for neurologic causes is warranted depending on the clinical findings. Temporal arteritis requires high-dose steroid therapy. Idiopathic intracranial hypertension requires urgent diagnostic and therapeutic lumbar puncture. CRANIAL NERVE III (OCULOMOTOR NERVE) Anatomy The oculomotor nerve is a pure motor nerve that works in conjunction with cranial nerves IV and VI to coordinate extraocular movements. The oculomotor nerve controls the superior rectus (globe elevator), medial rectus (globe adductor), inferior rectus (globe depressor), and inferior oblique (globe elevator) muscles. It also controls the levator palpebrae Cranial Nerve Disorders BOX 95.1 Differential Patterns of Visual Loss A central retinal etiology of the fovea or optic disk compromises visual acuity or causes central loss of vision in the affected eye only. Unilateral blindness is usually associated with an optic nerve lesion, and only the affected eye has complete visual field loss. Unilateral nasal visual field loss can be caused by an internal carotid artery aneurysm compressing the lateral optic chiasm. Bitemporal hemianopia can be caused by a midchiasmatic lesion. Homonymous hemianopia from an optic tract lesion causes full contralateral visual field loss in both eyes. Homonymous quadrantanopia secondary to a Meyer loop lesion causes contralateral one-quarter visual field loss in both eyes. Fig. 95.1 This 60-year-old man had diabetes mellitus, hypertension, coronary artery disease, chronic renal failure, and multiple myeloma. He sought medical care because of double vision (he described the images as “a little side by side but mostly up and down”), diplopia, ptosis, and papillary sparing. Findings on laboratory tests, magnetic resonance imaging, and magnetic resonance angiography were negative. The patient was evaluated by a neurologist and an ophthalmologist, and diabetic cranial nerve palsy was ultimately diagnosed. He was given an eye patch and scheduled for ophthalmologic follow-up. superioris muscle (upper eyelid elevator) and the intrinsic visceral motor function of the sphincter pupillae muscles and the ciliary muscles, which perform pupillary constriction and accommodation, respectively. Presenting Signs and Symptoms The patient typically complains of double vision or difficulty seeing out of the affected eye. There may be mild photophobia in bright light. The patient may also complain of an inability to raise the eyelid (ptosis). Cranial nerve III palsy is more common in patients older than 60 years and in those with diabetes or hypertension (Fig. 95.1). Patients with herniation syndromes will have a history of trauma (Fig. 95.2), tumor, or other neurologic findings.7 Pain associated with unilateral mydriasis should alert the emergency physician (EP) to look for an aneurysm involving the terminal internal carotid artery. Computed tomographic 819 SECTION IX NERVOUS SYSTEM DISORDERS angiography is more reliable than magnetic resonance angiography.8 Patients with an abscess or cavernous sinus thrombosis may have headaches, altered mental status, and seizures. This diagnosis should be considered in patients with signs and symptoms in the contralateral eye, previous sinus or midface infection, fever, chemosis, eyelid or periorbital edema, and exophthalmos. Extension of internal carotid artery dissection intracranially into the cavernous sinus can result in third, fourth, and sixth cranial nerve palsies.9 Treatment Treatment is dependent on the cause. CT should be performed to exclude a herniating mass. Admission for magnetic resonance imaging (MRI) and neurology or neurosurgical consultation is indicated for acute-onset deficits. CRANIAL NERVE IV (TROCHLEAR NERVE) Anatomy The trochlear nerve innervates the superior oblique muscle of the eye and causes inward rotation and downward and lateral movement of the globe. It is the smallest cranial nerve but has the longest intracranial course. Fig. 95.2 Ptosis and mydriasis suggest a cranial nerve III palsy. The appearance of these signs after a crush injury indicates that a skull fracture is impinging on the nerve canal. (Reproduced with permission from Baker C, Cannon J. Images in clinical medicine. Traumatic cranial nerve palsy. N Engl J Med 2005;353:1955.) A Presenting Signs and Symptoms Patients with a fourth cranial nerve palsy have double vision exacerbated by looking downward. The classic complaint is difficulty going down stairs. Most commonly, a history of trauma is reported. On physical examination the patient may unconsciously tilt the head away from the affected side (Fig. 95.3). Etiologic mechanisms are similar to those for the third cranial nerve and include inflammatory processes, trauma, and vascular causes.10 Treatment Treatment of isolated fourth nerve palsy is generally conservative, and the patient should be referred to neurology or neurosurgery as appropriate.10 CT, MRI, and neurology consultation are warranted if multiple cranial nerves are involved. CRANIAL NERVE V (TRIGEMINAL NERVE) Anatomy The trigeminal nerve is a mixed motor and sensory nerve. It provides motor innervation to the muscles of mastication, as well as sensation from the face, scalp, conjunctiva, globe, mucous membranes of the sinuses, tongue, teeth, and part of the external tympanic membrane. The trigeminal sensory ganglion is located in the middle cranial fossa and branches into three divisions: the ophthalmic nerve (V1), the maxillary nerve (V2), and the mandibular nerve (V3). Presenting Signs and Symptoms Patients with trigeminal nerve dysfunction have either sensory or motor deficits. Sensory dysfunctions include paroxysmal pain, paresthesias (abnormal sensations such as burning, pricking, tickling, or tingling), dysesthesias (disagreeable, unpleasant, or painful sensations produced by ordinary stimuli), and anesthesia (loss of sensation). The motor dysfunction is usually described as difficulty chewing and difficulty swallowing. Peripheral lesions cause loss of sensation or pain in only one division. Positive findings in two or more divisions (e.g., loss of light touch in one division and loss of sensitivity to pain, temperature, or pinprick in another division) should raise suspicion for a central cause. B Normal eye rotation When the head tilts to the left, both eyes rotate in the opposite direction (right eye extorts, left eye intorts) Cranial nerve IV palsy (right eye) Right eye extorted and slightly elevated, causing double vision. To compensate, the patient tilts her head to the left Fig. 95.3 A, Normal eye rotation. When the head tilts, both eyes rotate in the opposite direction. B, Cranial nerve IV palsy (right eye). The right eye is extorted and slightly elevated, which is causing double vision. The patient compensates by tilting the head to the left. 820 CHAPTER 95 The presence of associated cranial nerve deficits (III, IV, IV, or any combination of these nerves) suggests cavernous sinus involvement. In the setting of trauma, if a bruit over the orbit can be detected, a carotid–cavernous sinus fistula may be present. Associated involvement of cranial nerve VII or VIII or gait ataxia should raise suspicion for a cerebellopontine angle or lateral pontine tumor (Table 95.1). Associated Horner syndrome may indicate a cervical or lateral brainstem lesion. The main categories of trigeminal nerve dysfunction are trigeminal neuralgia and trigeminal neuropathy. A sudden Cranial Nerve Disorders onset of symptoms should raise suspicion for a vascular, traumatic, or demyelinating cause, whereas a more indolent course suggests tumor or inflammation (Table 95.2). TRIGEMINAL NEUROPATHY Causes include compression by an extrinsic mass, trauma, and vascular, inflammatory, or demyelinating disorders. Symptoms include neuralgia or paresthesia (or both) involving half of the face. Unlike trigeminal neuralgia, the pain with trigeminal neuropathy is more constant. Loss of the corneal reflex is evident. The patient’s mouth may become more oval Table 95.1 Clinicoanatomic Correlation of Localization of Lesions of Cranial Nerve V ANATOMIC SITE OF DAMAGE CLINICAL FINDINGS OTHER NEUROLOGIC AND MEDICAL FINDINGS COMMON CAUSES Sensory cortex Facial numbness, paresthesias Neglect, apraxia, aphasia Stroke, tumor, hemorrhage Internal capsule Hemifacial sensory loss Hemiparesis of the arm Stroke, tumor, hemorrhage, MS Supranuclear Corona radiata Central seventh cranial nerve paresis VPM thalamus Facial numbness, paresthesias, pain; cheirooral syndrome Anosmia, hemisensory deficit Stroke, tumor, hemorrhage Midbrain Facial numbness, paresthesias, pain Ophthalmoparesis Stroke, MS, tumor, aneurysm Pons Facial numbness and weakness, paresthesias, pain; trigeminal neuralgia Ophthalmoparesis; CN VI, CN VII, CN VIII palsies; Horner syndrome Stroke, tumor, hemorrhage; MS, syringobulbia, abscess, trauma Medulla Facial numbness, paresthesias, pain; trigeminal neuralgia Ataxia, CN X palsy, ophthalmoparesis, nystagmus, Horner syndrome, Wallenberg syndrome Stroke, MS, tumor, aneurysm, abscess, vasculopathy Facial numbness CN VII, CN VIII palsies; headache, cerebellar dysergia Neuroma, meningioma, meningitis (bacterial, TB, cancer), aneurysm, trauma Gasserian ganglion Facial numbness and weakness Gradenigo syndrome; CN VI, CN VII palsies Tumor, infection, trauma Skull base Facial numbness and weakness Headache, meningismus Meningitis (bacterial, TB, cancer, sarcoid) Nuclear Preganglionic Cerebellopontine angle Middle cranial fossa Trigeminal Nerve Branches V1: Cavernous sinus Facial numbness, pain Headache, ophthalmoparesis; Horner syndrome Tumor, thrombosis, infection, trauma V1: Carotidcavernous fistula Facial numbness Proptosis, bruit, ophthalmoparesis Trauma V2: Maxillary region Facial numbness; numb cheek syndrome Tumor, infarct, vasculopathy, trauma V3: Mandibular region Weakness of mastication; numb chin syndrome Tumor, trauma, infarct CN, Cranial nerve; MS, multiple sclerosis; TB, tuberculosis; VPM, ventroposteromedial. 821 SECTION IX NERVOUS SYSTEM DISORDERS Table 95.2 Selected Specific Causes Associated with Trigeminal Nerve Disorders ETIOLOGIC CATEGORY SELECTED SPECIFIC CAUSES Structural Disorders Developmental Brainstem vascular loop, syringobulbia Degenerative and compressive Paget disease Hereditary and Degenerative Disorders Chromosomal abnormalities, neurocutaneous disorders Hereditary sensorimotor neuropathy type I, neurofibromatosis (schwannoma) Degenerative motor, sensory, and autonomic disorders Amyotrophic lateral sclerosis Acquired Metabolic and Nutritional Disorders Endogenous metabolic disorders Diabetes Exogenous disorders (toxins, illicit drugs) Trichloroethylene, trichloroacetic acid Nutritional deficiencies, syndromes associated with alcoholism Thiamine, folate, vitamin B12, pyridoxine, pantothenic acid, vitamin A deficiencies Infectious Disorders Viral infections Herpes zoster, unknown Nonviral infections Bacteria, tuberculous meningitis, brain abscess, Gradenigo syndrome, leprosy, cavernous sinus thrombosis HIV infection, AIDS Opportunistic infection; abscess, herpes zoster Stroke, hemorrhage, aneurysm Neurovascular Disorders Neoplastic Disorders Primary neurologic tumors Glial tumors, meningioma, schwannoma Metastatic neoplasms, paraneoplastic syndromes Lung, breast; lymphoma, carcinomatous meningitis Demyelinating Disorders Central nervous system disorders Multiple sclerosis, acute demyelinating encephalomyelitis Peripheral nervous system disorders Guillain-Barré syndrome, chronic inflammatory demyelinating polyneuropathy Tolosa-Hunt syndrome, sarcoidosis, lupus, orbital pseudotumor Autoimmune and Inflammatory Disorders Traumatic Disorders Carotid-cavernous fistula, cavernous sinus thrombosis, maxillary/ mandibular injury Epilepsy Focal seizures Headache and Facial Pain Raeder neuralgia, cluster headache Drug-Induced and Iatrogenic Neurologic Disorders Orbital, facial, dental surgery From Goetz CG, editor. Textbook of clinical neurology. 2nd ed. Philadelphia: Saunders; 2003. AIDS, Acquired immunodeficiency syndrome; HIV, human immunodeficiency virus. 822 CHAPTER 95 and oblique in appearance, and because of loss of masseter muscle strength, the chin may be deviated toward the affected side. Until proved otherwise, neuropathies of cranial nerve V, the chin (numb chin; V3), and the suborbital region (numb cheek) should be presumed to be due to malignancies.11 TIC DOULOUREUX The term tic douloureux was coined by Nicolaus André, a French surgeon, in 1756. Its mechanism is probably compression of the trigeminal nerve root within millimeters of entry into the pons.12 The maxillary and mandibular divisions are most commonly affected, either alone or in combination. In one longitudinal case series, no cases of trigeminal neuralgia affecting both the ophthalmic and mandibular divisions were reported.2 Causes of tic douloureux are listed in Box 95.2. The International Association for the Study of Pain defines tic douloureux as “a sudden usually unilateral, severe, brief, stabbing, recurrent pain in the distribution of one or more branches of the fifth cranial nerve.” The pain is classically precipitated by normal activities such as eating, talking, washing the face, or cleaning the teeth. Diagnostic Testing The presence or absence of a corneal reflex should be checked. An intact reflex indicates normal function of the afferent V1 division, as well as normal cranial nerve VII motor efferent function. Absence of a corneal reflex can be caused by tumors in the posterior fossa or cerebellopontine angle, multiple sclerosis, brainstem strokes (Wallenberg or lateral medullary syndrome), and Parkinson disease. Motor function is evaluated by having the patient open and close the mouth and laterally deviate the jaw against resistance. Loss of muscle bulk or the presence of fasciculations in the temporalis or masseter musculature indicates a lower motor neuron lesion. The jaw jerk reflex test determines the integrity of the V3 division. The examiner places a thumb on the patient’s chin, after which the patient is instructed to relax the jaw completely with the mouth closed, and the examiner then taps the chin to elicit the jaw jerk reflex. The reflex will be diminished BOX 95.2 Causes of Tic Douloureux Vascular compression by an artery or vein Saccular aneurysm Arteriovenous malformation Vestibular schwannomas Meningioma Epidermoid cyst Tumor Primary demyelinating disorders • Multiple sclerosis • Charcot-Marie-Tooth disease (rare) Infiltrative disorders • Trigeminal amyloidoma Nondemyelinating lesions • Small infarct or angioma in the brainstem Familial Cranial Nerve Disorders in patients with a lower motor neuron lesion and accentuated in patients with a supranuclear lesion. Treatment A trial of carbamazepine can be therapeutic as well as diagnostic because failure to improve with carbamazepine suggests some other cause. Treatment options are listed in Box 95.3.3 Surgical approaches are considered when medication cannot control the pain or pain medication is not tolerated.13 CRANIAL NERVE VI (ABDUCENS NERVE) Anatomy The abducens nerve is a pure motor nerve that supplies the ipsilateral lateral rectus muscle of the eye and controls globe abduction. PRESENTING SIGNS AND SYMPTOMS Patients with an abducens nerve palsy usually complain of double vision. The head may be turned away from the affected side to maintain binocularity. Diabetes and hypertension are common risk factors. Another common sign is “crossed eyes” (esotropia or strabismus) (Fig. 95.4).14 Differential Diagnosis Children are more likely to have a tumor as the principal cause, and older individuals are more likely to have an ischemic cause such as temporal arteritis. An abducens nerve palsy occurring in isolation is rare. Usually, the seventh and eighth cranial nerves are also involved, which signals a central cause. Causes of abducens nerve palsy are listed in Box 95.4. BOX 95.3 Treatment of Trigeminal Neuralgia First-Line Agent Carbamazepine (Tegretol)—Start at 150 mg daily and increase by 100 mg every 3 days as needed to a total daily dose of 800 to 1600 mg divided into three doses. Second-Line Agents Oxcarbazepine (Trileptal)—Start at 300 mg daily and increase by 300 mg every 3 days as needed to a total daily dose of 1200 to 1800 mg divided into two doses. Gabapentin (Neurontin)—Start at 300 mg three times daily and increase as needed to a total daily dose of 3600 mg divided into three doses. Also commonly used as first-line therapy. Phenytoin (Dilantin)—Start at 300 mg daily and increase as needed, divided into two or three doses. Third-Line Agents (Add-On Therapy or Monotherapy) Lamotrigine (Lamictal)—Start at 25 mg daily and increase by 25 mg every 7 days as needed to a total daily dose of 200 to 400 mg divided into two doses. Baclofen (Lioresal)—Start at 15 mg daily and increase by 5 mg every 3 days as needed to a total daily dose of 60 to 80 mg divided into three doses. Reprinted with permission from Prasad S, Galetta S. Trigeminal neuralgia: historical notes and current concepts. Neurologist 2009;15:87-94. 823 SECTION IX NERVOUS SYSTEM DISORDERS BOX 95.4 Causes of Abducens Nerve Palsy A B Trauma—a blowout fracture of the orbit may result in a trapped medial rectus muscle and mimic a sixth nerve palsy Subarachnoid disorders—hemorrhage, infection (meningitis), tumor Vascular—intracavernous aneurysms; sixth nerve palsies are almost always the first clinical feature because of this nerve’s close relationship to the carotid artery and the fact that it is unsupported by a fibrous covering Giant cell arteritis Pontine glioma (in children) Pseudotumor cerebri—may be manifested as an isolated abducens nerve palsy in 30% of cases Inflammatory (postviral or demyelinating) leptomeningeal involvement secondary to carcinomatous meningitis; inflammatory or infiltrating lesions of the cavernous sinus Metabolic—vitamin B deficiency, Wernicke-Korsakoff syndrome Congenital absence of cranial nerve VI (Duane syndrome) C Fig. 95.4 This 62-year-old man reported acute left retroorbital pain of 1 week’s duration. Double vision developed, a rash appeared on his forehead, and he had restricted abduction in his left eye; this finding is diagnostic of a left sixth cranial nerve palsy (right, center, and left gaze seen in panels A, B, and C, respectively) and binocular horizontal diplopia. A diagnosis of herpes zoster ophthalmicus was made. The patient was treated with gabapentin and acyclovir for 1 week. Six weeks later, he had minimal residual diplopia with no postherpetic neuralgia. (Reproduced with permission from Jude E, Chakraborty A. Images in clinical medicine. Left sixth cranial nerve palsy with herpes zoster ophthalmicus. N Engl J Med 2005;353:e14.) Treatment Truly isolated sixth nerve palsies are often caused by microvascular ischemia secondary to hypertension or diabetes. A thorough work-up must be performed to rule out a central, inflammatory, infectious, or neoplastic cause. Close follow-up by a neurologist over a 6-month period is indicated; most cases resolve within 3 to 6 months. CRANIAL NERVE VII (FACIAL NERVE)— BELL PALSY Mechanisms The pathophysiology of Bell palsy has not been clearly established. Several theories have been proposed, including infectious or ischemic inflammation leading to nerve compression within the narrow canal as the nerve exits the stylomastoid foramen. Because the nerve is encased in a tight dural sheath within the temporal bone, this edema then causes additional compression of the vascular supply to the nerve.15 The cause of Bell palsy is most commonly idiopathic (66%).4 Numerous observed associations have been described 824 in the literature. The palsy is often preceded by a viral syndrome, and a correlation has been noted with herpes simplex virus (HSV). Its association with shingles and the characteristic blistering (from varicella-zoster virus [VZV]) is given the designation Ramsay Hunt syndrome. Reactivation of VZV has also been theorized as a cause. In addition, Bell palsy may be seen in patients with Lyme disease in places where the disease is endemic. Diabetes, hypertension, human immunodeficiency virus infection, sarcoidosis, Sjögren syndrome, parotid nerve tumors, eclampsia, amyloidosis, and the intranasal influenza vaccine have been associated with the development of Bell palsy.5,16 Other common triggers include stress, trauma, fever, tooth extraction, and a chilling episode from exposure to drafts and cold. Complete facial weakness, severe non–ear-related pain (e.g., retroauricular, cheek), late onset of recovery or no recovery by 3 weeks, diabetes, pregnancy, age older than 60 years, hypertension, and Ramsay Hunt syndrome are risk factors for incomplete recovery.17,18 Electroneurographic studies demonstrate a steady decline in electrical activity on days 4 to 10. When excitability is retained, 90% of patients recover fully, but when excitability diminishes to absence, only 20% of patients recover completely.5 Anatomy Cranial nerve VII is a mixed motor and sensory cranial nerve, which accounts for the varied symptoms. It travels adjacent to cranial nerves V, VI, and VIII as it traverses the cerebellopontine angle, the internal auditory meatus, and the temporal bone. Motor function involves the muscles of facial expression, the posterior digastric muscle, the stylohyoid muscle, and the stapedius muscle of the inner ear. CHAPTER 95 Fig. 95.5 “Raise your eyebrows.” A patient with a peripheral seventh nerve palsy (i.e., Bell palsy) will have loss of forehead wrinkles at rest and an inability to wrinkle the forehead and raise the eyebrow on the affected side (right side in this patient). Parasympathetic innervation includes the lacrimal glands, the mucous membranes of the nose, the hard and soft palate, and the submandibular and sublingual glands. The geniculate ganglion contains the nerve cell bodies of the sensory taste fibers of the anterior two thirds of the tongue.19 Presenting Signs and Symptoms To the patient, the most alarming symptom of Bell palsy is the abrupt onset of unilateral facial paralysis. Approximately 50% of patients believe that they have suffered a stroke, 25% think that they have an intracranial tumor, and the remaining 25% have no clear conception of what is wrong but are extremely anxious.4 The EP may note drooping of the eyebrow or the corner of the mouth (or both) and loss of wrinkles on the forehead or the nasolabial folds (or both). Inability to raise the eyebrow and furrow the forehead is a cardinal sign of Bell palsy (Fig. 95.5). Preservation of forehead motor neuron innervation should raise suspicion for a central cause.17 Because the forehead receives bilateral upper motor neuron innervation, a central stroke will spare the forehead and allow the patient to raise the eyebrow. If the patient can do this, it is not Bell palsy. Loss of nasolabial fold and nasal flaring is common. Loss of buccinator strength causes an inability to blow out the cheeks. An inability to close the eye on the affected side is a hallmark of Bell palsy. Speech is affected and may sound slurred or garbled, similar to dysarthria from a stroke. An asymmetric smile is often noted on examination (Fig. 95.6). The signs and symptoms vary depending on the site of the affected nerve. They are listed in Box 95.5. Cranial Nerve Disorders Fig. 95.6 “Show me your teeth”; “wrinkle your nose.” The risorius and orbicularis oris muscles are denervated. Notice the inability to corrugate the nose on the affected right side because of loss of function of the nasal and buccal musculature. BOX 95.5 Signs and Symptoms of Bell Palsy Ipsilateral tongue numbness Loss of taste or a dull taste Overt paralysis preceded by a sensation of subjective numbness or weakness on the affected side Ear pain in the external auditory canal Retroauricular pain Occipital headache Hyperacusis Fullness or snapping sound in the affected ear Tinnitus Drooling Inability to keep liquids in the mouth or chew Noticeable dryness of the oral and nasal mucous membranes on the affected side Anxiety Diagnostic Testing and Differential Diagnosis The “blow out your cheeks” test (Fig. 95.7) demonstrates loss of buccinator function. A sensitive variation of this test is to ask patients to hold water in their mouth and contract the buccal muscles. The water will either dribble out of the corner of the mouth or shoot across the room. On testing of hearing, hyperacusis may be observed on the affected side because of denervation of the stapedius. The patient should have no hearing loss. 825 SECTION IX NERVOUS SYSTEM DISORDERS Fig. 95.7 “Blow out your cheeks.” Loss of buccinator function prevents pursing of the lips and allows air (and food and liquids) to escape. Fig. 95.9 Characteristic auricular rash of Ramsay Hunt syndrome. Fig. 95.8 Buccal herpetic lesions in an individual with Ramsay Hunt syndrome. To evaluate taste sensation, a few granules of sugar are placed on the tip of the patient’s tongue on the affected side. Decreased taste sensation may be noted. Other cranial nerves should be normal. The abducens nucleus lies at the level of the genu of cranial nerve VII; infarction in the area can cause concomitant palsy of cranial nerve VI, which signals an upper motor neuron lesion rather than Bell palsy. No evidence of expressive or receptive aphasia should be present. The presence of vesicles on the tympanic membrane or in the oropharynx (Fig. 95.8) or the presence of grouped vesicular lesions on the face or around the ear (Fig. 95.9) suggests a diagnosis of Ramsay Hunt syndrome. Residual synkinesis can result from abnormal regeneration of nerve fibers. This can be manifested as abnormal motor function (e.g., blinking causes involuntary contracture of the risorius); as abnormal parasympathetic function, which is classically accompanied by “crocodile tears”—lacrimation after a salivary stimulus; or as hemifacial spasm, which can be bothersome, especially when the patient is tired. 826 Treatment The algorithm shown in Figure 95.10 outlines the treatment of patients with Bell palsy. Patients can be discharged home with oral medication, instructions for eye care, and expedited follow-up with a neurologist. Additional investigation for Lyme disease may be indicated for patients at risk. The evidence available indicates that steroids are safe and effective in shortening the course of the neurologic deficit and improving facial function.5,20-24 Patients receiving steroid therapy are up to 1.2 times more likely to attain good functional outcomes than untreated patients are.25 Corticosteroids reduce the risk for unsatisfactory recovery by 9%, with the number needed to benefit (NNTB) being 11.21 Corticosteroids were also associated with a 14% absolute reduction in risk for synkinesis and autonomic dysfunction, with an NNTB of 7.22 No studies have demonstrated significantly worse facial functional outcomes in patients treated with steroids.21,22,25 The most commonly reported treatment regimen is oral prednisone, 1 mg/kg up to 70 mg/day for a 10-day course. Dosing can be once daily or split into twice daily. The starting dose is continued for 6 days and tapered over the next 4 days.22,25 Alternatively, prednisone, 1 mg/kg/day, may be given for 7 days without a taper.4 Recent studies and metaanalyses have questioned the benefit of using antivirals for the treatment of Bell palsy.20-24,26 Antiviral agents used alone did not provide any benefit over placebo, and their use as the sole therapeutic agent is not recommended.20 When combined with corticosteroid therapy, antiviral therapy may have incremental benefit,21 but this remains to be shown conclusively. Therefore, until definitive studies are performed, clinical judgment will probably guide the use of antiviral therapy in cases in which a viral cause is strongly suspected (i.e., patients in whom HSV or VZV is CHAPTER 95 more significant than the physical disability. Patients report self-consciousness about the facial disfigurement, fear of permanent disfigurement, loss of self-esteem, and social ostracism. Acute facial weakness Central or peripheral? Peripheral Central Herpes zoster oticus No Bell palsy Ramsay Hunt syndrome Cranial Nerve Disorders 1) MRI to evaluate for ischemia and for infectious and inflammatory diseases 2) Consider: a. CSF b. ESR c. Serologic studies for syphilis, HIV, and vasculitis 3) Admit patient 1) Prednisone (started within 2-14 days of onset), 1 mg/kg/day for 7-14 days. Taper to 10 mg/day if more than 7 days 2) Valacyclovir 1000 mg three times daily for 7 days as clinically indicated and only in conjunction with corticosteroids Fig. 95.10 Algorithm outlining the treatment of patients with Bell palsy. CSF, Cerebrospinal fluid; ESR, erythrocyte sedimentation rate; HIV, human immunodeficiency virus; MRI, magnetic resonance imaging. contributory). Valacyclovir, 1 g three times daily for 7 days, can be prescribed in conjunction with corticosteroids. An eye shield or an eye patch should be worn during the night to prevent drying of the cornea. Liberal use of artificial tears during the day and an ophthalmic ointment such as Lacri-Lube at night should be prescribed to prevent drying of the cornea. Pain medication should be prescribed because the otalgia and cephalgia can be debilitatingly painful. Prognosis In a prospective study describing the spontaneous untreated course of idiopathic peripheral nerve palsy in patients with diabetes, 38% of patients had complete palsies, and only 25% regained normal facial muscle function.4 This is significantly worse than the observed rate of spontaneous full recovery in nondiabetic patients.27 Recurrence is rare (6.3%28) and should prompt a work-up for other causes such as myasthenia gravis, lymphoma, sarcoidosis, Lyme disease, and rarely, GuillainBarré syndrome.5,29,30 Although the prognosis for recovery is good, the psychologic consequences can be long-lasting and are perhaps CRANIAL NERVE VIII (VESTIBULOCOCHLEAR NERVE) Anatomy The vestibulocochlear nerve is a special sensory nerve that transmits auditory signals from the cochlea (hearing) and signals from the semicircular canals (balance). The vestibular apparatus also sits in the petrous temporal bone and is composed of a body consisting of the saccule and utricle and three semicircular canals aligned in three different planes. Hair cells within the endolymph of the canals detect angular movement and transmit the impulses to the vestibular nuclear complex in the floor of the fourth ventricle. The hair cells collectively combine to form the vestibular ganglion. Presenting Signs and Symptoms Patients with vestibulocochlear nerve dysfunction usually exhibit various degrees of hearing loss, tinnitus, vertigo, falling, and imbalance. The mechanism is asymmetric integration of vestibular input to the central nervous system or asymmetric disruption of sensory input from the vestibular organs.31 If the vertigo is severe, nausea and vomiting also occur. Symptoms may be constant or episodic. Vestibular neuronitis causes vertigo that lasts for weeks, and central vertigo may persist for years.32 Patients should be asked about triggers, particularly positional triggers because this may indicate benign paroxysmal positional vertigo. Recent viral and upper respiratory tract infections may be significant because they predispose to vestibular neuronitis. The history should also include the use of medications such as anticonvulsants, antihypertensives, sedatives, and ototoxic drugs. The examination should be focused on determining reproducibility of the symptoms, gait, balance, and ataxia; on evaluation of possible acute stroke symptoms; and on the character of the nystagmus and severity of the ataxia. The presence or absence of associated cerebellar signs such as lateralizing dysmetria, motor weakness, sensory loss, and abnormal reflexes should be noted, as well as the Babinski reflex and cranial nerve abnormalities such as ophthalmoplegia, dysarthria, and Horner syndrome.31 Abnormalities in cerebellar function should prompt consideration of a central cause. Patients should also be examined for vertical and rotatory nystagmus, which are not typically present in patients with peripheral vertigo; their presence warrants imaging and neurologic evaluation. Diagnostic Testing and Differential Diagnosis The Dix-Hallpike maneuver is commonly used to elicit positional nystagmus (see Fig. 96.1), which is associated with benign paroxysmal positional vertigo and usually lasts 5 to 60 seconds. Prolonged nystagmus is unlikely to be a result of this disorder. Gait and balance can be assessed with tandem walking and the Romberg test. Ataxia and lateralizing dysmetria can be assessed with finger-to-nose and heel-knee-shin testing. Hearing can be evaluated with the finger rub or finger snap, the Weber test, and the Rinne test. The ear and external auditory canal should be examined for evidence of cerumen, 827 SECTION IX NERVOUS SYSTEM DISORDERS otitis media, perforation of the tympanic membrane, and mass lesions. CT lacks sensitivity in the evaluation of cranial nerve VIII disorders but may be useful in evaluating the bony temporal region. MRI with gadolinium enhancement is useful in identifying acoustic neuroma. When a central cause is suspected because of abnormalities on cerebellar testing or clinical suspicion, MRI or magnetic resonance angiography (or both) should be performed to rule out a posterior circulation stroke as a central cause of the vertigo. The differential diagnosis should include other cranial nerve deficits that are not typically present in benign causes of cranial nerve VIII dysfunction. Acoustic neuromas may compress the trigeminal nerve when they attain a size of 3 cm or greater; patients with complaints of facial numbness should therefore be evaluated for trigeminal neuropathy, as well for a mass lesion. Because large tumors can affect cranial nerves IX, X, and XI, these nerves should also be tested. Treatment Some patients who come to the emergency department with sudden or severe symptoms may not be able to comply with testing because the severity of the symptoms limits the ability to open their eyes and turn their head without experiencing nausea and vomiting or exacerbating the symptoms. In these cases it is appropriate to treat the patient symptomatically, initiate a work-up, and reassess clinically for improvement before attempting to move the patient or perform provocative testing. CRANIAL NERVE IX (GLOSSOPHARYNGEAL NERVE) Anatomy The glossopharyngeal nerve provides branchial motor function to the stylopharyngeus muscle; visceral motor function to the otic ganglion and parotid gland; visceral sensory function from the carotid body; somatic sensory function to the posterior third of the tongue, the skin of the external ear, and the internal surface of the tympanic membrane; and the special sensory function of taste sensation from the posterior third of the tongue. Presenting Signs and Symptoms Patients with glossopharyngeal nerve palsy usually have associated symptoms involving other cranial nerves, most commonly cranial nerves X and XI. The most common symptoms are dysphagia and choking. If the vagus nerve is involved, the patient complains of hoarseness and demonstrates ipsilateral paralysis of the soft palate. Head, neck, and oral trauma or surgery can cause acute dysfunction of cranial nerve IX. Glossopharyngeal nerve palsy is a known complication of tonsillectomy surgery.33 Glossopharyngeal neuralgia is a rare disorder consisting of paroxysms of pain in the back of the throat and tongue. The pain is similar to that of trigeminal neuralgia in that the attacks are brief, lasting seconds to minutes. It is unilateral and usually triggered by chewing, swallowing, coughing, or sneezing. Treatment CT scanning is warranted to evaluate for a cerebrovascular event or tumor. Rarely, vasovagal syncope can result from 828 bradycardia or asystole caused by vagus nerve cardioinhibitory input. Medical management is similar to that for trigeminal neuralgia. If involvement of other cranial nerves is evident on examination, the patient should be admitted for further evaluation and neurologic consultation. CRANIAL NERVE X (VAGUS NERVE) Anatomy The vagus nerve is a mixed motor and sensory nerve that provides motor function to striated muscle of the pharynx, tongue, larynx, and tensor veli palatini, as well as motor function to smooth muscle and glands of the pharynx, larynx, and thoracic and abdominal viscera. Cranial nerve X provides general sensation from the skin at the back of the ear, the external auditory meatus, the pharynx, and part of the external surface of the tympanic membrane, as well as visceral sensation from the larynx, trachea, esophagus, and thoracic and abdominal viscera; from chemoreceptors in the aortic bodies; and from stretch receptors in the walls of the aortic arch. Presenting Signs and Symptoms Patients with palsies of the vagus nerve generally have hoarseness or difficulty swallowing. A history of recent carotid or thyroid surgery should prompt suspicion for a recurrent laryngeal nerve injury. The patient may also complain of regurgitation of food and liquid into the nose. Oropharyngeal examination usually reveals a drooped arch of the soft palate and uvular deviation away from the affected side. Treatment A CT scan of the head without contrast enhancement should be performed to evaluate for a cerebrovascular accident (hemorrhagic or ischemic) or skull-based lesions. Further inpatient evaluation may include MRI of the head and neck and workups for metabolic, infectious, or inflammatory disorders as warranted. CRANIAL NERVE XI (ACCESSORY NERVE) Anatomy The accessory nerve provides motor function to the sternocleidomastoid and trapezius muscles. Presenting Signs and Symptoms Patients with accessory nerve palsies have neck and shoulder weakness on the affected side. Inspection may reveal a “dropped” shoulder—that is, the affected shoulder lying downward and in lateral rotation. Testing of the sterno cleidomastoid reveals weakness when turning the head against resistance to the contralateral side. Because of the proximity of cranial nerves IX and X, particular attention should be paid to these nerve functions on examination. The most common causes are postoperative trauma (e.g., from cervical lymph node dissection) and a cerebrovascular accident. Treatment Treatment and disposition are similar to that for cranial nerves IX and X. CHAPTER 95 CRANIAL NERVE XII (HYPOGLOSSAL NERVE) Anatomy The hypoglossal nerve provides motor function to all the intrinsic tongue muscles and three of the four extrinsic tongue muscles: the genioglossus, styloglossus, and hypoglossus. Presenting Signs and Symptoms Patients with hypoglossal nerve palsies usually have unilateral tongue weakness. Differential Diagnosis The primary diagnostic consideration is distinguishing an upper from a lower motor neuron lesion. An upper motor TIPS AND TRICKS Patients with palsies of any of the 12 cranial nerves have heterogeneous symptoms reflecting the intrinsic function of each nerve. Patients with cranial nerve disorders generally have visual disturbances, facial weakness or pain, or paresthesias, depending on the nerve or nerves involved. Knowledge of the function of each of the cranial nerves helps the emergency physician recognize the classic signs and symptoms of cranial nerve palsies. Trigeminal neuralgia and Bell palsy are common cranial nerve disorders encountered in the emergency department. Corticosteroids are beneficial in the treatment of Bell palsy. Additional benefit of antiviral therapy is unclear. The majority of patients with an acute onset of facial weakness are concerned about a stroke. A thorough history and physical examination should be focused on assessing the potential for trauma (skull fracture), tumor, cerebrovascular accident, vascular derangements (aneurysm, dissection, thrombosis), and infection (meningitis, abscess). Morbidity primary results from these entities. The diagnostic work-up and disposition depend on the clinical findings. The presence of concomitant focal neurologic or systemic signs should heighten suspicion for a central rather than a peripheral cause of the neurologic dysfunction. Cranial Nerve Disorders neuron lesion causes contralateral tongue deviation and fasciculations, and tongue atrophy is absent. A lower motor neuron lesion causes ipsilateral tongue deviation and fasciculations, and tongue atrophy is present. A 26-year review of 100 cases of hypoglossal nerve palsy revealed that tumors, predominantly malignant ones, produced nearly half of the palsies. Only 15% of patients made a complete or nearly complete recovery.34 External lesions that cause compression or stretching of the nerve include internal carotid artery dissection or aneurysm, intracranial tumor, abscess, and other pharyngeal space tumors. Treatment Treatment and disposition are similar to that for cranial nerves IX, X, and XI. If there is concern for a cerebrovascular accident or space-occupying lesion, the patient should be admitted for evaluation. SUGGESTED READINGS de Almeida JR, Al Khabori M, Guyatt GH, et al. Combined corticosteroid and antiviral treatment for Bell palsy: a systematic review and meta-analysis. JAMA 2009;302:985-93. Engström M, Berg T, Stjernquist-Desatnik A, et al. Prednisolone and valaciclovir in Bell’s palsy: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet Neurol 2008;7:993-1000. Gilden DH. Clinical practice. Bell’s palsy. N Engl J Med 2004;351:1323-31. Gilden D. Treatment of Bell’s palsy—the pendulum has swung back to steroids alone. Lancet Neurol 2008;7:976–7. Salinas RA, Alvarez G, Daly F, et al. Corticosteroids for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev 2010;3:CD001942. Sherbino J. Evidence-based emergency medicine: clinical synopsis. Do antiviral medications improve recovery in patients with Bell’s palsy? Ann Emerg Med 2010;55:475-6. Worster A, Keim SM, Sahsi R, et al; Best Evidence in Emergency Medicine (BEEM) Group. Do either corticosteroids or antiviral agents reduce the risk of long-term facial paresis in patients with new-onset Bell’s palsy? J Emerg Med 2010;38:518-23. REFERENCES References can be found www.expertconsult.com. on Expert Consult @ 829 CHAPTER 95 REFERENCES 1. Coello AF, Canals AG, Gonzalez JM, et al. Cranial nerve injury after minor head trauma. J Neurosurg 2010;113:547-55. 2. Katusic S, Beard CM, Bergstralh E, et al. Incidence and clinical features of trigeminal neuralgia, Rochester, Minnesota, 1945-1984. Ann Neurol 1990;27:89-95. 3. Prasad S, Galetta S. Trigeminal neuralgia: historical notes and current concepts. Neurologist 2009;15:87-94. 4. Peitersen E. Bell’s palsy: the spontaneous course of 2500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol Suppl 2002;549:4-30. 5. Gilden DH. Clinical practice. Bell’s palsy. N Engl J Med 2004;351:1323-31. 6. Katusic SK, Beard CM, Wiederholt WC, et al. Incidence, clinical features, and prognosis in Bell’s palsy, Rochester, Minnesota, 1968-1982. Ann Neurol 1986;20:622-7. 7. Baker C, Cannon J. Images in clinical medicine. Traumatic cranial nerve palsy. N Engl J Med 2005;353:1955. 8. Chaudhary N, Davagnanam I, Ansari SA, et al. Imaging of intracranial aneurysms causing isolated third cranial nerve palsy. J Neuroophthalmol 2009;29:238-44. 9. Menon RK, Norris JW. Cervical arterial dissection: current concepts. Ann N Y Acad Sci 2008;1142:200-17. 10. Brazis PW. Isolated palsies of cranial nerves III, IV, and VI. Semin Neurol 2009;29:14-28. 11. Vahedi K, Bousser MG. Clinical examination of paralysis of the cranial nerves and principal etiologies. In: Doyon D, Marsot-Dupuch K, Francke JP, editors. The cranial nerves. Teterboro, NJ: Icon Learning Systems; 2004. p. 1-6. 12. Love S, Coakham HB. Trigeminal neuralgia: pathology and pathogenesis. Brain 2001;124:2347-60. 13. Toda K. Operative treatment of trigeminal neuralgia: review of current techniques. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:788-805. 14. Jude E, Chakraborty A. Images in clinical medicine. Left sixth cranial nerve palsy with herpes zoster ophthalmicus. N Engl J Med 2005;353:e14. 15. Gacek RR. Hilger: The nature of Bell’s palsy (Laryngoscope 1949;59:228-35). Laryngoscope 1996;106:1465-58. 16. Mutsch M, Zhou W, Rhodes P, et al. Use of the inactivated intranasal influenza vaccine and the risk of Bell’s palsy in Switzerland. N Engl J Med 2004;350:896-903. 17. Allen D, Dunn L. Aciclovir or valaciclovir for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev 2004;3:CD001869. 18. Holland NJ, Weiner GM. Recent developments in Bell’s palsy. BMJ 2004;329:553-7. Cranial Nerve Disorders 19. Wilson-Pauwels L, Akesson EJ, editors. Cranial nerves—anatomy and clinical comments. Toronto: BC Decker; 1988. p. 177. 20. Engström M, Berg T, Stjernquist-Desatnik A, et al. Prednisolone and valaciclovir in Bell’s palsy: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet Neurol 2008;7:993-1000. 21. de Almeida JR, Al Khabori M, Guyatt GH, et al. Combined corticosteroid and antiviral treatment for Bell palsy: a systematic review and meta-analysis. JAMA 2009;302:985-93. 22. Salinas RA, Alvarez G, Daly F, et al. Corticosteroids for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev 2010;3:CD001942. 23. Worster A, Keim SM, Sahsi R, et al; Best Evidence in Emergency Medicine (BEEM) Group. Do either corticosteroids or antiviral agents reduce the risk of long-term facial paresis in patients with new-onset Bell’s palsy? J Emerg Med 2010;38:518-23. 24. Sherbino J. Evidence-based emergency medicine: clinical synopsis. Do antiviral medications improve recovery in patients with Bell’s palsy? Ann Emerg Med 2010;55:475-6. 25. Grogan PM, Gronseth GS. Practice parameter: steroids, acyclovir, and surgery for Bell’s palsy (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2001;56:830-6. 26. Gilden D. Treatment of Bell’s palsy—the pendulum has swung back to steroids alone. Lancet Neurol 2008;7:976-7. 27. Kanazawa A, Haginomori S, Takamaki A, et al. Prognosis for Bell’s palsy: a comparison of diabetic and nondiabetic patients. Acta Otolaryngol 2007;127:888-91. 28. Katusic SK, Beard CM, Wiederholt WC, et al. Incidence, clinical features, and prognosis in Bell’s palsy, Rochester, Minnesota, 1968-1982. Ann Neurol 1986;20:622-7. 29. Keane JR. Bilateral seventh nerve palsy: analysis of 43 cases and review of the literature. Neurology 1994;44:1198-202. 30. English JB, Stommel EW, Bernat JL. Recurrent Bell’s palsy. Neurology 1996;47:604-5. 31. Delaney KA. Bedside diagnosis of vertigo: value of the history and neurological examination. Acad Emerg Med 2003;10:1388-95. 32. Hain TC. Cranial nerve VIII: vestibulocochlear system. In: Goetz CG, editor. Textbook of clinical neurology. 2nd ed. Philadelphia: Saunders; 2003. p. 195-210. 33. Windfuhr JP, Schlöndorff G, Sesterhenn AM, et al. From the expert’s office: localized neural lesions following tonsillectomy. Eur Arch Otorhinolaryngol 2009;266:1621-40. 34. Keane JR. Twelfth-nerve palsy. Analysis of 100 cases. Arch Neurol 1996;53:561-6. 829.e1