Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
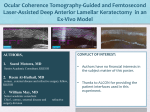
OCULAR SURGERY NEWS U.S. EDITION June 10, 2009 Femtosecond laser use in US increasing, but some still prefer microkeratomes While many U.S.-based refractive surgeons still prefer to use a microkeratome for creating a LASIK flap, market indicators appear to be pointing toward a shift to reliance on femtosecond technology. Published studies continue to show at least equal visual outcomes for the two technologies that are used to create LASIK flaps. However, whereas some surgeons consider femtosecond lasers to have an obvious safety advantage over microkeratomes, other surgeons are not convinced that the difference is significant. One factor in the shift toward laser in the United States may be the increasing demand by patients as consumers, according to Daniel S. Durrie, MD, OSN Refractive Surgery Section Editor. As patients research their options, he said, they note a growing body of evidence that suggests improved predictability and fewer negative outcomes, such as dry eye, after LASIK with flaps created by femtosecond laser. Then, when they come to the clinic, they more frequently request laser over blade for flap creation. “This is an elective procedure, and patients do have a choice, and I think they are choosing to go to doctors that have femtosecond lasers,” Dr. Durrie said. “They are really interested in something that uses a laser instead of a blade. Patients are starting to be knowledgeable enough to be asking for it.” Market shift Two independent surveys appear to indicate a shift in preference over the past decade toward femtosecond technology. In 2008, 33% of respondents to a survey by the American Society of Cataract and Refractive Surgery said they prefer to cut a LASIK flap using an Abbott Medical Optics IntraLase laser and 1% said they use a Ziemer Femto LDV femtosecond laser. Separately, about 40% of respondents to a survey by the International Society of Refractive Surgery of the American Academy of Ophthalmology indicated that they prefer to cut a LASIK flap with an IntraLase femtosecond laser (the survey report did not include data on the Ziemer device). In his study comparing femtosecond laser to microkeratome, Daniel S. Durrie, MD, found the femto laser either equal or significantly better in every outcome measure. Image: Botsford M Both the ISRS/AAO survey, which counted results from about 12% of its membership in 2008, and the ASCRS survey, which counted results from about 13% of its membership in 2008, indicate that use of any microkeratome is the preferred option among U.S. refractive surgeons. However, since 2003, the first year the ISRS/AAO collected data on use of femtosecond lasers to cut the LASIK flap, the percentage preferring femtosecond lasers has risen steadily, while use of any microkeratome has declined. The ASCRS started collecting data on femtosecond lasers a year earlier, in 2002, and the same trend has prevailed. According to Dr. Durrie, those numbers mirror what he has seen in his own observations of the market. “When I started using these in 2000, there were just a handful of people worldwide using it, and now it’s approaching 50% of all the procedures done in the U.S., and it’s spreading worldwide,” he said. To Dr. Durrie, this growth represents where the refractive surgery market is headed. For instance, he said, LCA-Vision — a market leader in vision correction that currently operates 75 laser-only vision correction centers in 34 states and 60 U.S. markets with joint ventures in Canada — has decided to exclusively offer femtosecond LASIK. Another indicator of the growing popularity of femtosecond lasers in the United States is interest from ophthalmic device manufacturers. Currently, AMO (IntraLase), Carl Zeiss Meditec (VisuMax), Technolas (Femtec) and Ziemer (Femto LDV) offer femtosecond lasers for U.S. distribution. In addition, Alcon and WaveLight unveiled a concept femtosecond laser at the 2009 ASCRS meeting. However, in an e-mail to Ocular Surgery News, a representative from Alcon Laboratories said that the company has not announced plans to enter the U.S. market with the technology. Growing evidence for femtosecond lasers Part of the driving force toward femtosecond technology, according to Dr. Durrie, is a growing body of evidence that femtosecond lasers produce at least equal visual outcomes compared with microkeratomes, but with more predictability in flap thickness and, perhaps, an improved safety profile. In 2005, Dr. Durrie published the first contralateral eye study comparing femtosecond laser vs. microkeratome. That study noted statistically significantly better uncorrected visual acuity with femtosecond laser. That difference disappeared, however, when postoperative astigmatism was controlled for, suggesting a difference in manifest refraction between the two cutting mechanisms. “When I started the study, I didn’t think I would find a difference. I had them both, and I was using them interchangeably,” Dr. Durrie said, noting that in every outcome measured, “the femtosecond laser was either equal or statistically significantly better.” The study was done with a femtosecond laser cutting at 15 kHz; the newest lasers cut at 150 kHz. Since the time of the study, improvements have also been made to microkeratome technology, but subsequent studies, according to Dr. Durrie, have continued to show that femtosecond laser has advantages over the microkeratome. “There hasn’t been a study to come out yet, at least that I have seen, that says the femtosecond laser isn’t as good” as microkeratome, Dr. Durrie said. “With all the other factors, especially with patient preference, and the general movement [toward femtosecond by] a large portion of the market, I think that’s the direction everything’s going.” Still a role for microkeratomes Richard A. Norden Other surgeons, such as Richard A. Norden, MD, still see a role for microkeratomes in refractive surgery, especially with the technology advances of the latest-generation devices, such as the Moria One Use-Plus SBK microkeratome. Dr. Norden also has a femtosecond laser in his center and said that his first results with the new microkeratome in 100-µm flap LASIK equal those of the femtosecond laser, with some additional, non-negligible advantages. “The time of procedure is shorter, about 8 minutes on average. Uncorrected visual acuity at 10 minutes postop is impressive, with no photodisruption-induced inflammation and no pain at all experienced by the patients,” he said. The SBK head and ring are single-use devices, which helps eliminate complications and risks associated with reusable heads. The elimination of sterilization and maintenance and the short suction time and overall procedure time allow for a fast patient turnover. Dr. Norden said flap thickness is extremely predictable, and contrary to most microkeratomes, the flap is planar, with no meniscus shape. Case-by-case basis For other surgeons, the choice of flap-cutting technology is done on a case-by-case basis. According to N. Timothy Peters, MD, FACS, there are cases for which a femtosecond laser is desirable, but the evidence is not abundant that it should be used in all cases. “There certainly are published articles showing better visual and wavefront outcomes with a femto than with microkeratome, but there are also studies that report the opposite,” he said. “Until you get a randomized, multicenter, controlled clinical trial, I don’t know that you answer that question for sure.” According to Dr. Peters, a microkeratome, because it is smaller than a femtosecond laser, is more suited for smaller or deeper eyes. Previous corneal incision may also indicate the need for microkeratome or refractive correction via PRK instead of LASIK. When the predictability of the flap thickness is crucial – such as in older patients, patients with dry eye, patients with underlying epithelial problems, and patients with steep or flat corneas – bladeless LASIK is the prudent choice. However, for the large percentage of patients who opt for a laser refractive correction, the natural anatomy of the eye does not obviate the choice. “In those people, where thickness is an issue, you absolutely have to have femtosecond,” Dr. Peters said, but “in terms of the average, run-of-the-mill thick cornea, I don’t think there is much of a difference.” The evidence is convincing, he said, that even the newest generation of microkeratomes has a larger standard deviation in flap thickness compared with femtosecond lasers, but “in someone with a very thick cornea and a small prescription, the accuracy of how deep that flap will cut is somewhat irrelevant.” Lucio Buratto, MD, who runs a large private practice in Milan, Italy, and who was influential in the development of the Hansatome microkeratome (Bausch & Lomb) as well as one of the first European IntraLase users, agrees with the individualized approach to flap-cutting technology. “If you asked me whether I prefer microkeratome LASIK or femtosecond-laser LASIK, I would honestly answer, for most of my patients, I have no preference. It’s a matter of selecting the best option for individual patients,” Dr. Buratto said. In his practice, he uses both kinds of devices, depending on the case he is operating on, and maintains that both are excellent instruments in expert hands, with specific advantages and drawbacks for each. Lucio Buratto “Generally speaking, for the average, uncomplicated cases, I still prefer microkeratomes. They are very good, perfectly safe and reliable instruments. The femtosecond laser is heavier on the eye and requires a slightly longer suction time, as well as some waiting time for bubble dissipation, which may cause some discomfort and anxiety in the patient,” he said. IntraLase, on the other hand, is Dr. Buratto’s first choice in eyes in which a micron-perfect centration is needed, in eyes with abnormally large pupils, in nanophthalmic eyes and in eyes in which preoperative aberrations need to be treated. He emphasized that the latest-generation femtosecond lasers are overcoming previous problems. “They are faster, easier to use, extremely precise, and produce perfect cuts and even smoother surfaces. The creation of cavitation bubbles has been minimized, and the low-energy impact promotes a fast, uneventful and highly predictable recovery of vision,” he said. Thinner flaps and predictability To some, whether one technology is better remains unknown. However, some surgeons feel strongly that femtosecond technology offers a distinct advantage in the realm of safety, and because of that, surgeons should rely on that technology more often. “People expect to pay to get vision. They don’t expect to pay to get complications. We have two objectives in mind: to do an efficacious procedure and to do a safe procedure,” Louis E. Probst, MD, said. Dr. Probst said he has noted a 3% to 5% greater rate of 20/20 UCVA in patients after using IntraLase to cut the LASIK flap compared with microkeratome at his clinic, TLC Laser Eye Center in Westchester, Ill. Of greater significance, he said, there has been a reduction in both complication rates and severity of adverse outcomes with IntraLase. Louis E. Probst “With the IntraLase, not only are there four to six times less aborted procedures or adverse events, but similarly, if you do have an aborted procedure, it is generally nothing of visual significance, and so you can turn around and do a PRK procedure the same day, or within a week or so,” Dr. Probst said. Safety is one reason for the shift toward femtosecond technology, but the predictability of the flap thickness is also crucial. According to both the ISRS/AAO and ASCRS surveys, U.S. surgeons are increasingly opting for a thinner flap and a thicker residual stromal bed. In the ISRS/AAO survey, for instance, 39% said they prefer to cut the flap at 100 µm thickness or less, up from 11% since 2004, the first year the question on preferred flap thickness was asked, and an additional 50% said they cut the flap thickness at 120 µm to 130 µm. A similar trend was seen in the ASCRS numbers, in which just more than 32% of respondents said they prefer a 100-µm flap, up from 11% in 2004. Additionally, 50% said they regularly cut the flap to 120 µm to 130 µm. The surveys differed in the proportion that indicated a preference for a thicker flap, ranging from 150 µm to 180 µm or more: around 11% in the ISRS/AAO data and around 18% in the ASCRS data. Both studies showed a preference for a thicker residual stromal bed. Among both ISRS/AAO and ASCRS respondents, 52% said they routinely leave a 250-µm bed. Additionally, both surveys noted a decrease since 2004 in reliance on a 250-µm bed, with a concomitant rise in either a 275-µm or 300-µm residual stromal bed. The shift to a philosophy of retaining as much of the residual stromal bed as possible comes from published studies showing a negative correlation between bed thickness and risk of ectasia. Because the thinness of the flap and the thickness of the residual stromal bed are important, Dr. Probst said, the predictability of flap thickness offered by femtosecond technology becomes that much more important. “It’s important for leaving a consistent stromal bed,” he said. “The key is reduced standard deviation with IntraLase. It’s the variation in those deep flaps and those shallow beds.” Dr. Probst said he targets a 100-µm flap and an approximately 300-µm residual stromal bed. With the standard deviation in that flap thickness, which is somewhere in the area of ±10 µm, he said he is confident that the resulting flap will range from 90 µm to 110 µm. That compares favorably, he said, with experiences with the microkeratome. With a far less predictable variation, that same 100-µm target could yield an 80-µm to 150-µm flap. “If you’ve got a 150-µm flap, and you’re also doing a large excimer ablation, you may be down to a 250 µm, maybe even less, maybe down to 200 µm or less in the bed, and that is going to put that patient at greater risk of ectasia,” Dr. Probst said. Special uses of femtosecond laser Research is currently ongoing on uses for femtosecond lasers other than for LASIK flap creations. That could become important, according to Dr. Peters, for the surgeon considering purchasing one platform or the other. For instance, microkeratomes can also be used in preparation of the donor tissue during corneal transplant procedures. Research is also ongoing on alternative uses for femtosecond technology, including using it to reshape the cornea to achieve refractive correction. In the intraCOR treatment, according to Mark Tomalla, MD, of the Duisburg Niederrhein Clinic in Germany, the Femtec laser is used to make a series of concentric cuts within the intrastromal volume without affecting either the surface of the cornea or other vital structures, such as the endothelium, Bowman’s layer or Descemet’s membrane. A localized reorganization of biomechanical forces is induced within the treatment area, leading to a central, intrastromal steepening with smooth transition zones and, consequently, increased depth of field. “A new mechanical equilibrium is generated, and the cornea is reshaped. The refractive power is locally changed, leading to significantly improved near vision and good intermediate vision without affecting distance vision,” Dr. Tomalla said. This treatment has had good results so far in trials, he said. Another promising option offered by femtosecond technology is FLEx (femtosecond lenticule extraction) with the VisuMax laser. The laser dissects a lenticule of corneal tissue and then creates a flap as a single-step procedure. The refractive lenticule is then manually removed by the surgeon, using special instruments. “This extraction creates the refractive effect,” Walter Sekundo, MD, of Philipps University of Marburg, Germany, said. Dr. Sekundo said that the VisuMax system can be used to create a conventional LASIK flap, but that the idea of going beyond simple flap making and eliminating the need for two lasers is appealing. – by Bryan Bechtel and Michela Cimberle References: Chan A, Ou J, Manche EE. Comparison of the femtosecond laser and mechanical keratome for laser in situ keratomileusis. Arch Ophthalmol. 2008;126(11):1484-1490. Duffey RJ, Leaming D. US Trends in Refractive Surgery: 2008 ASCRS Survey. Presented at: Annual Meeting of the American Society of Cataract and Refractive Surgery. April 3-8, 2009; San Francisco. Available at: http://duffeylaser.com/physicians_resources.php. Accessed May 1, 2009. Duffey RJ, Leaming D. US Trends in Refractive Surgery: The 2008 ISRS/AAO Survey. Presented at: Annual Meeting of the American Academy of Ophthalmology, November 8-12, 2008; Atlanta. Available at: http://duffeylaser.com/physicians_resources.php. Accessed May 1, 2009. Durrie DS, Kezirian GM. Femtosecond laser versus mechanical keratome flaps in wavefront-guided laser in situ keratomileusis: Prospective contralateral eye study. J Cataract Refract Surg. 2005;31(1):120-126. Norden RA. Patient and practice benefits of One Use-Plus SBK. Presented at: American Academy of Ophthalmology meeting; November 2008; Atlanta. Ruiz LA. Intrastromal refractive correction with no flap. Presented at: World Ophthalmology Congress; June 2008; Hong Kong. Schallhorn SC, Tanzer DJ, Kaupp SE, Brown M, Malady SE. Comparison of night driving performance after wavefront-guided and conventional LASIK for moderate myopia. Ophthalmology. 2009;116(4):702-709. Sekundo W, Kunert K, Russmann C, et al. First efficacy and safety study of femtosecond lenticule extraction for the correction of myopia: Six-month results. J Cataract Refract Surg. 2008;34(9):1513-1520. Stanley PF, Tanzer DJ, Schallhorn SC. Laser refractive surgery in the United States Navy. Curr Opin Ophthalmol. 2008;19(4):321-324. Lucio Buratto, MD, can be reached at CAMO, Piazza Repubblica 21, 20124 Milano, Italy; 39-02-6361191; fax: 39-02-6598875; e-mail: [email protected]. Dr. Buratto has no financial interest in any of the products mentioned in this article, nor is he a paid consultant for any company mentioned. Daniel S. Durrie, MD, can be reached at Durrie Vision, 5520 College Blvd., Suite 200, Overland Park, KS 66211; 913-491-3737; fax: 913-491-9650; email: [email protected]. Dr. Durrie is a clinical investigator for Abbott Medical Optics and Alcon. Richard A. Norden, MD, can be reached at Norden Laser Eye Associates, 1144 East Ridgewood Ave., Ridgewood, NJ 07450; 866-614-9220; fax: 201-444472; e-mail: [email protected]. Dr. Norden has no financial interest in any of the products mentioned in this article, nor is he a paid consultant for any company mentioned. N. Timothy Peters, MD, FACS, can be reached at Clear Advantage Laser Vision Center, 330 Borthwick Ave., Suite 306, Portsmouth, NH 03801; 603501-5000; fax: 603-501-5001; e-mail: [email protected]. Dr. Peters is a consultant for Technolas Perfect vision. Louis E. Probst, MD, can be reached at TLC Laser Eye Center, 4 Westbrook Corporate Center, Suite 111, Westchester, IL 60154; 708-562-2020; fax: 708562-4785; e-mail: [email protected]. Dr. Probst is a consultant for Abbott Medical Optics. Walter Sekundo, MD, can be reached at Philipps University, Department of Ophthalmology, Robert-Koch Strasse 4, 35037 Marburg, Germany; 49-64215866275; fax: 49-6421-5865678; e-mail: [email protected] or [email protected]. Dr. Sekundo’s research on FLEx has been supported by Carl Zeiss Meditec. Mark Tomalla, MD, can be reached at Klinik für Refraktive & OphthalmoChirurgie, Fahrner Strasse 133, 47169 Duisburg, Germany; 49-203-5801711; fax: 49-203-5081713; e-mail: [email protected]. Dr. Tomalla has no financial interest in any of the products mentioned in this article, nor is he a paid consultant for any company mentioned.