Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
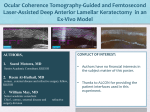
J CATARACT REFRACT SURG - VOL 31, NOVEMBER 2005 Anterior chamber gas bubbles after corneal flap creation with a femtosecond laser Tova Lifshitz, MD, Jaime Levy, MD, Itamar Klemperer, MD, Shmuel Levinger, MD A 48-year-old woman had bilateral wavefront-guided laser in situ keratomileusis for myopia with IntraLase corneal flap creation. In the right eye the cavitation bubbles were observed not only in the interface between the flap and the corneal bed but also in the anterior chamber disappearing after 30 minutes. After the procedure, uncorrected visual acuity is 20/25 in both eyes; and specular microscopy shows normal hexagonal cells and density. Although no postoperative complications were observed in our case, further follow-up is needed to examine the long-term effect of this phenomenon of IntraLase. J Cataract Refract Surg 2005; 31:2227–2229 Q 2005 ASCRS and ESCRS During the past 5 years, several reports have described the results in laboratory and clinical settings of the femtosecond laser for the creation of a corneal flap in laser in situ keratomileusis (LASIK) procedures and its advantages over current microkeratome systems.1–6 These reported advantages include the creation of more predictable flap dimensions, the use of low vacuum during suction, and the theoretical elimination of intraoperative flap complications such as incomplete flap, buttonhole perforation, and unpredictable thickness.2–4,6 In essence, the femtosecond laser is focused on a predetermined depth within the corneal stroma, delivering pulses of light in a raster pattern, creating focused cavitation spots within the stroma that will expand and result in a resection plane. Cavitation bubbles representing carbon dioxide and water can appear not only underneath the flap but also in the pocket, behind the hinge, and sometimes in the episclera or in the circumferential host tissue. After several seconds to minutes, the bubbles disappear and a standard LASIK procedure can be performed. Accepted for publication December 2, 2004. From the Department of Ophthalmology (Lifshitz, Levy, Klemperer), Soroka University Medical Center, Ben-Gurion University of the Negev, Beer-Sheva, Israel, and ‘‘Enaim’’ Ophthalmological Center (Lifshitz, Klemperer, Levinger), Jerusalem, Israel. No author has a financial or proprietary interest in any material or method mentioned. Reprint requests to Jaime Levy, MD, Department of Ophthalmology, Soroka University Medical Center, P.O. Box 151, Beer-Sheva 84101, Israel. E-mail: [email protected]. Q 2005 ASCRS and ESCRS Published by Elsevier Inc. Bubbles appearing in the anterior chamber are a known and infrequent complication during flap creation with a femtosecond laser, but to our knowledge they have not been reported in the literature. We describe the first reported case in the literature of bubbles in the anterior chamber during corneal flap creation with a femtosecond laser. No postoperative complications were observed. CASE REPORT A 48-year-old woman sought refractive surgery to correct myopia. The patient’s ocular history was unremarkable, with no history of contact lens wear. The uncorrected visual acuity (UCVA) was 20/200 in both eyes, the best spectacle-corrected visual acuity was 20/20 in the right eye and 20/25 in the left eye with a refraction of ÿ5.25 ÿ2.50 15 in the right eye and ÿ5.25 ÿ2.25 171 in the left eye. Central keratometry (Canon RK-2) measured 44.25 in both eyes, in the right eye and 44.50@171/47.00@81 in the left eye. Preoperative ultrasound pachymetry (Nidek US-1800, 10 MHz frequency) was 534 mm in the right eye and 540 mm in the left eye. Preoperative corneal topography and Orbscan (Bausch & Lomb) showed abnormalities in the posterior float or the thickness map. Before surgery, the patient received a full explanation of the procedure and a written informed consent was obtained. The patient had a bilateral wavefront-guided (Zyoptix Keracor 217, Bausch & Lomb) LASIK with IntraLase (IntraLase Corp.) corneal flap creation. A myopic final refraction was targeted for monovision. With an eyelid speculum, the eye was fixated with the standard IntraLase patient interface suction fixation ring. The IntraLase computer settings were a planned flap thickness of 100 mm, a planned flap diameter of 9.0 mm, a hinge angle of 45 degrees, raster energy of 2.2 mJ, beam separation of 11 mm, line separation of 9 mm, and a side-cut energy of 4.0 mJ. A superior pocket of 290 mm depth was created. The cornea was applanated with the disposable glass contact lens cone attached to the suction ring via an internal clamp. Following creation of the flap, the suction ring was released and the applanating contact lens was 0886-3350/05/$-see front matter doi:10.1016/j.jcrs.2004.12.069 2227 CASE REPORTS: LIFSHITZ removed. In the right eye, cavitation bubbles were observed not only in the interface and corneal stroma but also in the anterior chamber (Figure 1) and the flap was then lifted. Flap lifting was uneventful in the left eye. It was decided to continue with the laser treatment. The intended refraction was ÿ3.75 ÿ2.13 18 in the right eye and ÿ4.72 ÿ1.77 168 in the left eye. During the laser ablation in the right eye, the eyetracker had difficulty in detecting the center of the pupil owing to the bubbles in the anterior chamber and it had to be realigned several times. The procedure was eventually completed successfully. The cavitation bubbles disappeared after about 30 minutes. This was the only case with bubbles in the anterior chamber observed in our center after several hundred procedures. One day after LASIK, the UCVA was 20/30 in both eyes with bilateral clear corneas, improving to 20/25 in both eyes after 1 week. Three months after the procedure, the UCVA was 20/25 in both eyes. Specular microscopy 1 week and 1 month after the procedure revealed normal hexagonal cells and density of 2850 cells/mm2 in the right eye and 2629 cells/mm2 in the left eye. DISCUSSION More than 100 000 procedures worldwide have been performed with the IntraLase technology (IntraLase Corp. data, July 2004). Data on file of complications include thin flaps, perforations of the flap with flap elevation instruments, and the dispersion of gas bubbles from the interface through the anterior stroma via defects in Bowman’s layer into the subepithelial space interfering with additional laser treatment. The near-infrared neodynium-glass laser pulse (1053 nm) passes through the superficial corneal tissue unabsorbed, unlike argon–fluoride excimer lasers, until it is focused to a small spot size at a desire depth.1 When the laser pulse reaches this focal point, a process called Figure 1. Intraoperative photograph of the right eye after the creation of the flap with the IntraLase. Cavitation bubbles can be observed in the anterior chamber. 2228 laser-induced optical breakdown is initiated.1,2 Due to plasma ignition and its explosive expansion, a shockwave is generated. In media with high aqueous saturation, such as the cornea, a vapor-filled bubble develops at the breakdown region without interfering with surface cell layers.1,2,5 Due to the photodissociation of involved water, the bubble contains hydrogen. Femtosecond laser–induced optical breakdown requires very low energy and produces virtually no thermal damage or shockwave transmission to surrounding tissue. The spots are placed 5 to 12 mm apart side to side6 and 7 to 15 mm in front of each other (line separation). As the microcavitation bubbles expand, the spots coalesce, forming a resection plane. The byproducts are carbon dioxide and water, which are absorbed by the action of the endothelial pump. The created bubbles may remain within the stroma for several seconds to minutes and can interfere with subsequent laser pulses. If 2 successive laser pulses are placed too close to each other, the produced bubbles merge, leading to large intrastromal bubbles that will deflect following laser pulses, resulting in remaining tissue bridges.5 To overcome this problem, the pulses of very low energy threshold are delivered in a raster pattern, resulting in microcavitation bubbles and allowing nearly contiguous placement of laser pulses without almost collateral shockwave effects. The reported histologic data of corneas after femtosecond corneal flap creation show that with pulse energy of 4 mJ and spot separation of 15 mJ, the tissue effects are minor, with bubbles in the anterior stroma created by the merging of many single bubbles, in which there is loose collagen debris.1 Up to the present and with the reported laboratory data, the exact dynamics of the bubbles and their interaction is not fully understood. In this case, the IntraLase initial settings were similar to those previously reported.3,6 We speculate that many small bubbles coalesced and created larger bubbles that migrated through the posterior stroma and endothelium without being absorbed by the endothelial pump, and these bubbles appeared in the anterior chamber. Theoretically, the laser shockwave might push the air bubbles posteriorly, and if stromal lamellae are weak or endothelial junctions are not too tight, the bubbles can appear in the anterior chamber. Large bubbles could also be created near the pocket and then would migrate to the posterior stroma and anterior chamber. Another mechanism might be a retrograde passage of the bubbles from the perilimbal area to the trabecular meshwork into the anterior chamber. During the wavefront-guided laser procedure, the eyetracker was unable to follow the pupil because of the presence of the bubbles in the anterior chamber. In this case, the bubbles disappeared after about 30 minutes, so it is advisable to wait for spontaneous resolution of the bubbles before starting with the excimer laser procedure. J CATARACT REFRACT SURG - VOL 31, NOVEMBER 2005 CASE REPORTS: LIFSHITZ Future laboratory investigations are needed to examine possible endothelial damage after femtosecond corneal flap creation in refractive surgery and to clarify whether preoperative endothelial anomalies can predispose to the presence of cavitation bubbles in the anterior chamber. REFERENCES 1. Lubatschowski H, Maatz G, Heisterkamp A, et al. Application of ultrashort laser pulses for intrastromal refractive surgery. Graefes Arch Clin Exp Ophthalmol 2000; 238:33–39 2. Sugar A. Ultrafast (femtosecond) laser refractive surgery. Curr Opin Ophthalmol 2002; 13:246–249 3. Nordan LT, Slade SG, Baker RN, et al. Femtosecond laser flap creation for laser in situ keratomileusis: six-month follow-up of initial U.S. clinical series. J Refract Surg 2003; 19:8–14 4. Ratkay-Traub I, Ferincz IE, Juhasz T, et al. First clinical results with the femtosecond neodymium-glass laser in refractive surgery. J Refract Surg 2003; 19:94–103 5. Heisterkamp A, Mamom T, Kermani O, et al. Intrastromal refractive surgery with ultrashort laser pulses: in vivo study on the rabbit eye. Graefes Arch Clin Exp Ophthalmol 2003; 241:511–517 6. Binder PS. Flap dimensions created with the IntraLase FS laser. J Cataract Refract Surg 2004; 30:26–32 J CATARACT REFRACT SURG - VOL 31, NOVEMBER 2005 2229