Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Heart failure wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Electrocardiography wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
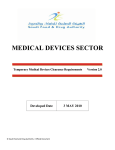
Exercise Performance and Activity Level in Children With Transposition of the Great Arteries Treated by the Arterial Switch Operation Elsje van Beek, MSca, Mathijs Binkhorst, MDa, Marieke de Hoog, MSca, Patricia de Groot, PhDa,*, Arie van Dijk, MD, PhDb, Michiel Schokking, MD, PhDb, and Maria Hopman, MD, PhDa The exercise capacity of children after arterial switch for transposition of the great arteries (TGA) is known to be at the lower limit of normal. We aimed to ascertain whether this results from compromised hemodynamics or deconditioning. A total of 17 children with TGA (12 male and 5 female children; age 12.1 ⴞ 2.0 years) treated with the arterial switch operation were compared with 20 age-matched controls (13 male and 7 female children; age 12.8 ⴞ 2.4 years) regarding their peak exercise capacity, peak workload, and peak heart rate, as assessed by cycle ergometry. The children’s physical activity level was monitored for a 7-day period using a pedometer and diary, and a questionnaire was used to assess physical activity participation and overprotection. The results demonstrated that TGA children showed a significantly reduced peak exercise capacity (47.4 ⴞ 6.4 vs 41.1 ⴞ 6.6 ml/kg/min; p <0.05), maximal workload (3.7 ⴞ 0.5 vs 3.1 ⴞ 0.6 W/kg; p <0.01), and maximal heart rate (189 ⴞ 9 vs 180 ⴞ 14 beats/min; p <0.05) compared to the controls. No significant differences were found in the physical activity pattern or overprotection. In conclusion, given the comparable physical activity level, but reduced exercise capacity in the TGA children, these children most likely fall short in their exercise performance because of restrictive hemodynamics rather than deconditioning from reduced daily life activity. © 2010 Elsevier Inc. All rights reserved. (Am J Cardiol 2010;105:398 – 403) Previous studies have shown that the exercise capacity of children after arterial switch for transposition of the great arteries (TGA) is, in general, slightly lower than that of their healthy peers.1–3 Although previous research focused on either exercise capacity or activity pattern (24-hour heart rate monitoring4 survey5), the present study has uniquely addressed both physical fitness and the physical activity pattern of children with TGA treated by the arterial switch operation (ASO). Moreover, the physical activity pattern was studied comprehensively in our participants using 7-day activity monitoring (pedometer and diary) and a questionnaire on physical activity and participation. We combined the approach of exercise testing and activity monitoring in an attempt to determine whether (1) the aerobic capacity is indeed reduced in children with TGA compared to that of healthy peers, and (2), if true, whether this resulted from reduced physical activity or cardiac restriction. The results of the present study might aid in the preparation of specific recommendations regarding participation in daily physical activity functioning, sports, and therapy for children with TGA that could improve their quality of life. a Department of Integrative Physiology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands; bDepartment of Pediatric Cardiology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands. Manuscript received July 9, 2009; revised manuscript received and accepted September 11, 2009. *Corresponding author: Tel: (⫹31) 0-24-361-3676; fax: (⫹31) 0-24354-0535. E-mail address: [email protected] (P. de Groot). 0002-9149/10/$ – see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.amjcard.2009.09.048 Methods Children eligible for participation in the present study were selected from a database of the Department of Pediatric Cardiology that includes patients with TGA who underwent surgery from 1990 to 1999 at the Radboud University Nijmegen Medical Centre (Nijmegen, The Netherlands). Patients with metabolic, neurologic, muscular, or orthopedic anomalies were excluded. Also, syndromes with congenital heart defects as one of the features, heart failure (New York Heart Association class ⱖI), cyanosis at rest (oxygen saturation ⬍90%), and severe cardiac arrhythmia were considered exclusion criteria. A total of 35 children were contacted by letter and invited to participate in the study. The siblings of these children were asked to participate in the control group. Of the 35 children, 5 could not be traced because of invalid address data. In total, 17 children with TGA aged 10 to 17 years and 20 gendermatched control subjects were included in the present study. The local ethical committee of the Radboud University Nijmegen approved the study, and the children and their parents provided written informed consent. Anthropometric measurements were taken and included height, weight, abdominal girth, and skin fold thickness. For each participant, body mass index was calculated. The abdominal girth was assessed to estimate the amount of abdominal fat and was measured 1 cm above the level of the iliac crest. A 4-site (biceps, triceps, subscapular, and suprailiac) skin fold thickness measurement of the nondominant body site was performed (Ponderal, Zoetermeer, The Netherlands). The sum of the 4 skin folds was used to www.AJConline.org Congenital Heart Disease/Exercise in Children With TGA 399 Table 1 Demographic and anthropometric values of both groups Variable Control Group (n ⫽ 20) TGA Group (n ⫽ 17) Gender Male 13 12 female 7 5 Age (years) 12.8 ⫾ 2.4 (10–17) 12.1 ⫾ 2.0 (10–17) Weight (kg) 49.5 ⫾ 10.6 (33.1–70.7) 47.3 ⫾ 14.1 (28.5–76.8) Length (cm) 159.9 ⫾ 12.2 (141–186) 156.2 ⫾ 14.6 (138–186) Body mass index 19.2 ⫾ 2.3 (16.4–23.8) 19.1 ⫾ 2.4 (14.8–23.5) (kg/m2) Lean body mass (kg) 40.9 ⫾ 9.4 (26.4–59.8) 38.5 ⫾ 11.5 (23.3–65.4) Systolic blood 110 ⫾ 11 (85–132) 119 ⫾ 13 (90–154) pressure (mm Hg) Diastolic blood 76 ⫾ 8 (60–114) 72 ⫾ 9 (60–90) pressure (mm Hg) Data are presented as mean ⫾ SD (minimum to maximum range). Table 2 Cardiac co-morbidities in children with transposition of the great arteries (TGA) treated by arterial switch operation (ASO) Deficiency Complete right bundle branch block Incomplete right bundle branch block First-degree atrioventricular block Homograft stenosis Pulmonary stenosis Pulmonary insufficiency Neoaortic insufficiency Aortic valve stenosis Pulmonary valve stenosis Tricuspid valve insufficiency Mitral valve insufficiency Narrowing of left ventricular outflow tract Enlarged neoaortic root diameter Figure 1. Peak aerobic capacity (ml/kg/min) in children with TGA after ASO (n ⫽ 15) and controls (n ⫽ 15). Values are presented as mean ⫾ SD. *p ⬍0.05. Patients (n) 1 5 1 1 13 1 5 1 1 1 1 1 2 determine the age- and gender-adjusted body fat percentage. Using the tables provided by Deurenberg et al6 and this information, the lean body mass was calculated. The blood pressure at rest was measured with a manual sphygmomanometer (Welch Allyn Max-Stabil 3, Jungingen, Germany). To measure cardiovascular fitness and exercise capacity, all children performed an incremental exercise test on a half-supine, electronically braked, cycle ergometer (Sensormedics BV, Bilthoven, The Netherlands) adhering to a standardized ramp protocol.7 During cycling, the workload was gradually increased by 10, 15, or 20 W/min (depending on the subject’s weight, age, gender, and exercise habits), and the cycling speed was maintained at approximately 65 rpm. The exercise was terminated at the subjects’ request, because of electrocardiographic changes associated with myocardial ischemia, physical exhaustion, dyspnea, or calf/thigh pain. To prevent decreases in systolic blood pressure from venous pooling after test termination, the subjects were instructed to continue cycling for 3 additional minutes at 30 rpm against a workload of 20 W.8 A 12-lead electrocardiogram was obtained during each minute of exercise and recovery. The heart rate and rhythm were monitored continuously (GEMS IT Cardiosoft V4.2, Freiburg, Germany), and blood pressure was measured with 2-minute intervals. Gas exchange parameters were obtained throughout the exercise test and during the first 2 minutes of recovery on a breath-by-breath basis using a metabolic cart (Vmax Spectra 29, SensorMedics, Yorba Linda, California). The oxygen consumption and respiratory quotient were measured every 20 seconds. The peak oxygen uptake (VO2peak) was defined as the mean of the last 40 seconds of the ergometer test. The exercise test results were considered valid when the following criteria were met: (1) observed exhaustion of the child, (2) VO2peak leveling off, and (3) respiratory quotient ⬎1.00.9 The subjects were asked to repeat the cycle ergometer test 1 week later if the respiratory quotient had remained ⬍1.00. Only data meeting these criteria were analyzed. The daily physical activity level was assessed using an electronic pedometer (Yamax SW-200 DigiWalkers, Yamax, Japan) and an activity diary for 7 days, including 2 weekend days. The pedometer was clipped to the waistline at the right side according to the manufacturer’s instructions. The activity diary consisted of 7 timelines, 1 for each day. Each day was divided into 48 U, with 1 U representing 30 minutes. The activities were indicated using numbers drawn from a previously devised legend. Arrows were used to indicate the child’s waking hours. The activities were computed to the metabolic equivalent (MET) values (1 MET ⫽ 1 kcal/kg/hr) using the Compendium of Physical Activities, a coding scheme that classifies specific physical activity by the rate of energy expenditure.10 To obtain a questionnaire concerning physical fitness and participation in sports for children with coronary heart disease (CHD), the Haemophilia and Physical Fitness Questionnaire (Department of Paediatric Physical Therapy, Rad- 400 The American Journal of Cardiology (www.AJConline.org) Table 3 Exercise test results in both groups Variable VO2peak (ml/kg/min) VO2peak lean body mass (ml/kg/min) VO2peak (% of predicted) Respiratory quotient Peak workload (W) Peak workload (W/kg) Peak heart rate (beats/minute) Heart rate after 1 min (beats/minute) Heart rate after 3 min (beats/minute) Control Group (n ⫽ 15) TGA Group (n ⫽ 15) p Value 47.4 ⫾ 6.4 (39.3–58.4) 58.2 ⫾ 10.0 (46.1–85.4) 94.6 ⫾ 12.1 (75.6–111.5) 1.04 ⫾ 0.03 (0.98–1.09) 179.3 ⫾ 60.5 (96–320) 3.7 ⫾ 0.5 (2.7–4.7) 189 ⫾ 9 (168–200) 153 ⫾ 17 (113–178) 120 ⫾ 16 (83–146) 41.1 ⫾ 6.6* (32.1–55.5) 50.5 ⫾ 7.1* (32.1–55.5) 81.4 ⫾ 10.9* (63.0–103.8) 1.03 ⫾ 0.04 (0.98–1.12) 154.1 ⫾ 61.6 (80–312) 3.1 ⫾ 0.6* (2.5–4.2) 180 ⫾ 14 (155–202) 149 ⫾ 16 (126–179) 118 ⫾ 14 (89–146) 0.013 0.021 0.004 0.46 0.27 0.005 0.045 0.40 0.80 Data are presented as mean ⫾ SD (minimum to maximum range). * p ⬍0.05. Figure 2. Peak workload (W/kg) in children with TGA after ASO (n ⫽ 15) and controls (n ⫽ 15). Values are presented as mean ⫾ SD. *p ⬍0.05. boud University Nijmegen Medical Centre, Nijmegen, The Netherlands) was modified to suit our study purposes. This CHD and physical fitness questionnaire was used to acquire information on co-morbidities, the number of hours of sports participation at school and during leisure time, recreational exercise, other leisure activities, type of transport to and from school, self-rated fitness and health and physical activity, and overprotection. The results are expressed as the mean ⫾ SD, with the range. For comparison of the anthropometric measurements, exercise testing parameters, pedometer and activity measurements, unpaired Student’s t tests were applied. For comparison of frequencies, chi-square tests were administered. For intergroup comparison of ordinal variables, the nonparametric Mann-Whitney U test was used. Descriptive statistics were used for questions concerning overprotection. For all tests, a level of significance of p ⬍0.05 was used. All statistical analyses were performed with Statistical Package for Social Sciences for Windows, version 16.0 (SPSS, Chicago, Illinois). Figure 3. Peak heart rate (beats/min) during exercise testing in children with TGA after ASO (n ⫽ 15) and controls (n ⫽ 15). Values are presented as mean ⫾ SD. *p ⬍0.05. Results Two subjects in the TGA group could not perform the cycle test because of practical problems. One child had a cold and difficulties breathing through the mask and one was too small and could not reach the pedals properly. The remaining children (n ⫽ 15) met the criteria for a valid exercise test, and physical exhaustion was the reason for test termination. Because the predicted VO2peak values were greater for the male children than for the female children, the exercise test results of the 15 TGA subjects who were able to complete the test were compared with the results of 15 gender- and age-matched control subjects. The pedometer, diary, and questionnaire results of the entire TGA group were compared with the results of 17 age- and gender-matched subjects. The data from 20 control subjects were used. No significant differences were found in age, Congenital Heart Disease/Exercise in Children With TGA 401 Table 4 Activity monitoring in both groups Variable Number of steps/day Metabolic equivalent score (without sleep) Metabolic equivalent score/hour awake Metabolic equivalent/hour/day Greatest metabolic equivalent score/hour Time awake (hour) Control Group (n ⫽ 17) TGA Group (n ⫽ 17) p Value 11,794 ⫾ 2,326 (9,024–16,629) 36.8 ⫾ 7.1 (26.0–54.4) 2.5 ⫾ 0.5 (1.3–3.5) 1.9 ⫾ 0.3 (1.4–2.6) 5.5 ⫾ 1.1 14.4 ⫾ 0.7 (13.3–15.6) 11,016 ⫾ 4,560 (5,598–26,227) 32.3 ⫾ 5.1* (25.5–43.2) 2.3 ⫾ 0.3 (1.9–2.9) 1.7 ⫾ 0.2 (1.5–2.1) 5.5 ⫾ 1.6 14.0 ⫾ 0.9 (12.7–15.8) 0.54 0.044 0.16 0.56 0.99 0.13 Values are presented as mean ⫾ SD (minimum to maximum range). * p ⬍0.05. Table 5 Congenital heart disease and physical fitness questionnaire results for both groups Variable Control Group (n ⫽ 17) TGA Group (n ⫽ 17) Self-rated health (scale 1–10) 8.5 ⫾ 1.2 (7–10) 8.4 ⫾ 1.2 (5–10) Self-rated fitness (scale 1–10) 7.6 ⫾ 0.9 (6–9) 7.2 ⫾ 1.2 (5–9) Participation in sports (hours/ 3.5 ⫾ 1.7 (0.5–7.5) 4.8 ⫾ 0.8 (0–11) week) Participation in sports 27.0 ⫾ 14.2 (3–47) 37.0 ⫾ 23.1 (4–75) (metabolic equivalent/ week) Participation in physical 17/17 (100%) 15/17 (88%) education class* Overprotection by self† 0/17 (0%) 1/17 (6%) Overprotection in past by 0/17 (0%) 4/17 (23%) environment‡ Overprotection in present by 0/17 (0%) 3/17 (18%) environment Data are presented as mean ⫾ SD (range), unless otherwise indicated. * Percentage of subjects who always participate in physical education class and do not stop during exercises. † Subject considers physical activity harmful. ‡ Environment considers physical activity harmful. weight, length, body mass index, lean body mass, or blood pressure between the TGA and control groups (Table 1). The mean age at surgery was 7.6 ⫾ 10.8 days. Of the 17 subjects with TGA, 15 underwent ASO during the first 2 months of life, with closure of an atrial septal defect and/or ventricular septal defect, if necessary. One subject with partial anomalous pulmonary venous return and left atrial isomerism underwent an ASO with correction of the partial anomalous pulmonary venous return. At 11 years of age, an atrial inhibited rate modulated pacemaker was implanted with a lower rate of 70 beats/min and an upper center rate of 180 beats/min because of an abnormal chronotropic response to exercise. One patient had TGA with a large subaortic ventricular septal defect and pulmonary stenosis. For this patient, a Blalock-Taussig shunt was placed as a palliative procedure 3 days after birth, followed by a Rastelli procedure 2 years later. Four patients required cardiac catheterization with balloon dilation to treat stenosis at the site at which the pulmonary artery was reconnected during the ASO. One subject underwent repeat surgery to close the remainder of an atrial septal defect at 6 and 8 years of age. The residual postoperative cardiac co-morbidities are listed in Table 2. The VO2peak (ml/kg/min) and the adjusted per kilogram lean body mass were significantly lower in the TGA group than in the controls (Figure 1, Table 3). In addition, the peak workload (Figure 2) and peak heart rate (Figure 3) were significantly lower in the TGA subjects than in the controls (Table 3). No significant differences were evident between the TGA and control group in the total number of steps or MET scores per hour (Table 4). The MET score during awakening was significantly lower for the TGA children than for the controls (p ⫽ 0.044). However, the MET score per hour awake did not differ between the 2 groups. No differences were observed regarding self-rated fitness and health, participation in sports and activities at and after school, physical activity level, or overprotection between the TGA and control groups (Table 5). Discussion This is the first study to compare children with TGA to their healthy peers regarding both the physical activity pattern and fitness late after the ASO. Our findings have demonstrated that the VO2peak, peak heart rate, and peak workload were significantly lower in the TGA group than in the control group. In contrast, the physical activity patterns were not different between the 2 groups, suggesting that physical hemodynamic restrictions are more important causal factors for the lower exercise capacity levels than reduced physical activity. Our findings demonstrated that VO2peak (ml/kg/min) adjusted for lean body mass and VO2peak, expressed as a percentage of the predicted, were significantly lower in the TGA group (81%) than in the controls (95%). Subnormal values of maximal heart rate during exercise (chronotropic impairment) and subnormal exercise capacity in children after ASO have been previously reported,1,2 although VO2peak values within the normal range have also been reported.3 Pasquali et al1 determined the maximal exercise capacity in 53 children after ASO. Variant coronary artery patterns were present in 30%, and the investigators reported that VO2peak was lower than predicted in subjects with usual and variant coronary artery patterns (89 ⫾ 20% and 80 ⫾ 17%, respectively).1 Furthermore, multivariate analyses revealed that a variant coronary artery pattern and ventricular septal defect were predictors of chronotropic impairment 402 The American Journal of Cardiology (www.AJConline.org) and associated with a trend toward lower a VO2peak (p ⬍ 0.09). However, we did not have this information for our participants and were unable to sort the data in a similar matter. The physical activity pattern in daily living, as indicated by the total number of steps or MET score did not differ between TGA group and the age- and gender-matched controls. A lower total MET score during awaking hours was found for the TGA group. However, it is important to correct this score for the actual hours that the children were awake. Because the TGA children in the present study spent more hours sleeping than did the controls, this difference was no longer evident when the MET score was expressed per hour awake (p ⫽ 0.16). Previous studies of children with CHD, including TGA, have indicated that these children were significantly less active than controls. Massin et al4 investigated the activity patterns of 52 children with TGA 7 to 14 years after ASO using 24-hour heart rate monitoring and compared the results to those from 127 age-matched healthy peers. The TGA group emerged as significantly less active than the control group regarding moderate and vigorous activities. However, because chronotropic impairment can be present in TGA, continuous heart rate monitoring does not seem to be the most suitable method to assess exercise intensity and physical activity patterns in these children. In the present study, exercise intensity was calculated as the average greatest MET score per hour, and this outcome was similar in both groups. Apparently, children with TGA are as physically active as healthy control children and do not refrain from physically demanding tasks. Self-perceived restrictions, overprotection by parents, or altered self-perception are factors that might explain the observed lower physical activity levels of children with CHD as reported in previous studies.11–13 Although overprotection by parents is often described as an explanation for the lower physical activity levels in children with cardiac defects,12 our findings have not supported this assumption. Four children with TGA (24%) reported overprotection by their environment in the past, 3 (18%) reported overprotection by the environment in the present, and 1 (6%) considered physical activity to be harmful. However, the person being overprotective for the child with CHD was never a parent or sibling. Using the outcomes of the questionnaires completed by our subjects, no differences in participation in sports and leisure activities between the TGA group and healthy peers were present. Furthermore, physical fitness and general health status were rated equally in both groups, suggesting that an altered self-perception is not present. These results are in concordance with the absence of any differences in physical activity as recorded in the diary and by the pedometer between the 2 study groups. Cardiac/hemodynamic restrictions that can adversely affect exercise capacity in children with TGA include chronotropic impairment, which emerged during peak exercise in the present study. These subnormal maximal heart rate values can be caused by partial cardiac sympathetic denervation after transection of the great arteries during ASO.3,14 From exercise studies in the spinal cord-injured population with cervical lesions, it is known that substantially lower peak heart rates (ie, 120 to 140 beats/min) occur during exercise.15 Also, it has been shown previously that patients who underwent surgery ⬎55 days after birth had a lesser amount of reinnervation, which might have affected their exercise tolerance years after surgery.14 A subnormal maximal heart rate could also be caused by conduction defects secondary to cardiopulmonary bypass.16 Other potential mechanism that could relate to cardiac/hemodynamic restrictions and compromised physical capacity in children with TGA include residual hemodynamic defects, such as a mild to moderate degree of supravalvular pulmonary stenosis, which was present in all but 2 of the 15 children with TGA completing the cycle test. Also, decreased right and left ventricular ejection fractions in patients with TGA could equally contribute to reduced exercise capacity.17 Finally, an abnormal coronary flow reserve caused by manipulation of the coronary arteries during the ASO could alter the balance between myocardial oxygen supply and demand, thereby reducing exercise capacity. A previous study documented a prevalence of coronary lesions in 6.8% of 324 patients, 7 years after ASO.18 The long-term development of coronary circulation in these patients, including the evolution of atherosclerosis and coronary flow reserve, is still unknown.19 In conclusion, the findings of the present study have demonstrated that the exercise capacity of children with TGA after ASO is significantly reduced compared to that of their age- and gender-matched healthy peers. The daily life activity pattern and sport participation did not differ between the 2 groups. Hence, it appears that the decrease in exercise capacity in children with TGA mainly results from compromised hemodynamic restrictions rather than a reduced physically active lifestyle. Future studies on the clinical consequences for cardiovascular health of altered hemodynamics in children with congenital heart diseases are recommended. 1. Pasquali SK, Marino BS, McBride MG, Wernovsky G, Paridon SM. Coronary artery pattern and age impact exercise performance late after the arterial switch operation. J Thorac Cardiovasc Surg 2007;134: 1207–1212. 2. Reybrouck T, Eyskens B, Mertens L, Defoor J, Daenen W, Gewillig M. Cardiorespiratory exercise function after the arterial switch operation for transposition of the great arteries. Eur Heart J 2001;22:1052–1059. 3. Mahle WT, McBride MG, Paridon SM. Exercise performance after the arterial switch operation for D-transposition of the great arteries. Am J Cardiol 2001;87:753–758. 4. Massin MM, Hovels-Gurich HH, Gerard P, Seghaye MC. Physical activity patterns of children after neonatal arterial switch operation. Ann Thorac Surg 2006;81:665– 670. 5. Lunt D, Briffa T, Briffa NK, Ramsay J. Physical activity levels of adolescents with congenital heart disease. Aust J Physiother 2003;49: 43–50. 6. Deurenberg P, Pieters JJ, Hautvast JG. The assessment of the body fat percentage by skinfold thickness measurements in childhood and young adolescence. Br J Nutr 1990;63:293–303. 7. Cooper CB, Storer TW. Exercise testing and interpretation. A practical approach. New York: Cambridge University Press, 2001. 8. Fletcher GF, Balady GJ, Amsterdam EA, Chaitman B, Eckel R, Fleg J, Froelicher VF, Leon AS, Pina IL, Rodney R, Simons-Morton DA, Williams MA, Bazzarre T. Exercise standards for testing and training: a statement for healthcare professionals from the American Heart Association. Circulation 2001;104:1694 –1740. 9. Rowlands AV, Eston RG, Ingledew DK. Measurement of physical activity in children with particular reference to the use of heart rate and pedometry. Sports Med 1997;24:258 –272. Congenital Heart Disease/Exercise in Children With TGA 10. Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O’Brien WL, Bassett DR Jr, Schmitz KH, Emplaincourt PO, Jacobs DR Jr, Leon AS. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc 2000;32: S498 –S504. 11. Hovels-Gurich HH, Konrad K, Wiesner M, Minkenberg R, HerpertzDahlmann B, Messmer BJ, Von Bernuth G. Long term behavioural outcome after neonatal arterial switch operation for transposition of the great arteries. Arch Dis Child 2002;87:506 –510. 12. Shonkoff CJ. Reactions to the threatened loss of a child: a vulnerable child syndrome, by Morris Green, MD, and Albert A Solnit, MD, Pediatrics, 1964;34:58 – 66. Pediatrics 1998;102:239 –241. 13. Wray J, Sensky T. How does the intervention of cardiac surgery affect the self-perception of children with congenital heart disease? Child Care Health Dev 1998;24:57–72. 14. Kondo C, Nakazawa M, Momma K, Kusakabe K. Sympathetic denervation and reinnervation after arterial switch operation for complete transposition. Circulation 1998;97:2414 –2419. 15. Takahashi M, Matsukawa K, Nakamoto T, Tsuchimochi H, Sakaguchi A, Kawaguchi K, Onari K. Control of heart rate variability by cardiac 16. 17. 18. 19. 403 parasympathetic nerve activity during voluntary static exercise in humans with tetraplegia. J Appl Physiol 2007;103:1669 –1677. Perrault H, Drblik SP, Montigny M, Davignon A, Lamarre A, Chartrand C, Stanley P. Comparison of cardiovascular adjustments to exercise in adolescents 8 to 15 years of age after correction of tetralogy of Fallot, ventricular septal defect or atrial septal defect. Am J Cardiol 1989;64:213–217. Martin RP, Qureshi SA, Ettedgui JA, Baker EJ, O’Brien BJ, Deverall PB, Yates AK, Maisey MN, Radley-Smith R, Tynan M. An evaluation of right and left ventricular function after anatomical correction and intra-atrial repair operations for complete transposition of the great arteries. Circulation 1990;82:808 – 816. Legendre A, Losay J, Touchot-Kone A, Serraf A, Belli E, Piot JD, Lambert V, Capderou A, Planche C. Coronary events after arterial switch operation for transposition of the great arteries. Circulation 2003;108(Suppl 1):II186 –II190. Hauser M, Bengel FM, Kuhn A, Sauer U, Zylla S, Braun SL, Nekolla SG, Oberhoffer R, Lange R, Schwaiger M, Hess J. Myocardial blood flow and flow reserve after coronary reimplantation in patients after arterial switch and Ross operation. Circulation 2001; 103:1875–1880.